
Abstract
Ta** is a common technique used to address proprioceptive deficits in both healthy and patient population groups. Although there is increasing interest in ta** to address proprioceptive deficits, little is known about its effects on the kinetic aspects of proprioception as measured by force sense accuracy. To address this gap in the literature, the present systematic review and meta-analysis was conducted to evaluate the impact of ta** on force sense accuracy. A search for relevant literature was conducted following PRISMA guidelines across seven databases and one register. Eleven studies with 279 participants were included in the review out of 7362 records. In the between-group analyses, we found a significant improvement in absolute (p < 0.01) and relative (p = 0.01) force sense accuracy with ta** compared to no comparator. Likewise, a significant improvement in absolute (p = 0.01) force sense accuracy was also observed with ta** compared to placebo tape. In the within group analysis, this reduction in the absolute (p = 0.11) force sense accuracy was not significant. Additional exploratory subgroup analyses revealed between group improvement in force sense accuracy in both healthy individuals and individuals affected by medial epicondylitis. The findings of this meta-analysis should be interpreted with caution due to the limited number of studies and a lack of blinded randomized controlled trials, which may impact the generalizability of the results. More high-quality research is needed to confirm the overall effect of ta** on force sense accuracy.
Similar content being viewed by others


Introduction
Ta** has gained widespread attention in rehabilitation and performance science [1]. The earliest use of ta** in rehabilitation dates back to as early as 1969, as documented in the literature [2]. Its integration in modern practice was prominently observed during the 2012 London Olympics, where Kinesiota** was identified as one of the most frequently used treatment modalities by the Olympians [3]. The intervention entails the application of specialized adhesive tape to the body to achieve various therapeutic and performance-related outcomes [4]. The growing use of this intervention is largely due to its viability [5], ease of application [6], availability [7], and cost-effectiveness [8, 9]. Owing to these factors, the application of ta** in the existing literature extends across a range of medical conditions including chronic ankle instability [10], patellofemoral pain syndrome [11], low back pain [12], lymphedema [13], Parkinson’s disease [14], and stroke [15]. Likewise, the application of ta** also extends across a range of sports including, Judo [16], athletics [17], Taekwondo [18], soccer [19], and Karate [20].
Researchers have put forth various explanations concerning the effects of ta** in the literature [10, 21,22,23,24,25]. For instance, adhesive patellar ta** has been reported to alternate muscle function by facilitating muscle kinematics such as, torque, moment, and power [21]. Similarly, in individuals with patellofemoral pain syndrome [26], the application of adhesive patellar ta** has been reported to allocate knee extensor moment arm in an advantageous position which results in facilitated muscle activity. Additionally, facilitating ergonomic movement strategies including trunk engagement, and improvement of vastus medialis obliques and vastus lateralis ratio have been reported with rigid Leuko ta** to be supplementary mechanisms that could facilitate muscle function [27]. Likewise, “microcirculatory” effects of Kinesiota** interventions have also been proposed as a mechanism in the literature that could facilitate recovery. Studies have suggested that the “skin lifting” associated with ta** interventions could facilitate local circulation [28], augment lymphatic and venous drainage [29, 30] which might result in enhanced recovery and performance. Moreover, ta** has also been reported to pertain with psychological effects, primarily centered around boosting the wearer’s confidence and perception of stability [10, 31, 32]. Researchers have indicated that heightened confidence and a sense of stability through rigid sports ta** could enable individuals with joint instability to perform challenging tasks more effectively than without the tape [10, 31].
Furthermore, an additional advantage attributed to ta** is the enhancement of joint proprioception. This aspect has been linked to ta**’s potential to improve recovery and performance [33,34,35]. Research has suggested that the tactile feedback provided by ta** activates mechanoreceptors, which can enhance proprioception through increased input to the central pathways [34, 36]. Eventually, this amplified afferent input consequently aids in bolstering the efferent neuromuscular response, which increases both the speed and the quality of the muscle reaction (i.e., reduced reaction time) [37, 38]. Konishi [36] suggested that reduced proprioceptive activity due to injury or weakness might impede the ability of mechanoreceptors to provide regular afferent feedback to gamma motor neurons. This deficiency in afferent feedback could disrupt the modulation of primary afferents and hinder the recruitment of high-threshold motor units [39]. The author suggested that ta**’s tactile stimulation might offer a potential solution by bypassing this deficit and rescuing alpha motor activity [36].
Additionally, elastic tapes such as Kinesiotape have been reported to induce a phenomenon known as “skin stretch”, which alters underlying tissue and improves proprioception [40, 41]. This ability of the ta** to influence underlying tissue is believed to modify the musculoskeletal kinetics, ultimately leading to improved muscular activation [42,43,44], and increased comfort [45]. For instance, Franettovich Smith, Coates [46] proposed that the elastic tape’s recoil properties could potentially offer mechanical support or opposition (such as deceleration or acceleration) to movement. This, in turn, could alleviate the strain on musculotendinous units by decreasing the load demands, while simultaneously allowing for the execution of a complete range of motion. Also, proprioceptive enhancement due to ta** is identified as an effective means of prophylaxis to prevent injury [47, 48]. In this context, the improved proprioception and the resistive properties of athletic and Kinesiotape, may also help prevent movement into potentially injury-prone ranges ultimately reducing further risk of injury [32, 47, 49, 50]. Moreover, patellar ta** has demonstrated non-biomechanical neurological effects that enhance motor performance [10, 51, 52]. An fMRI study revealed heightened activity in the cerebellum, primary somatosensory cortex, supplementary motor area, primary sensory cortex, and cingulate motor area due to ta** [51]. The authors posited that the increased activation observed was indicative of improvements in coordination, sensation, decision-making, and coordination of non-conscious aspects of proprioception [51]. Similarly, recent electrophysiological data indicated that ta** might facilitate proprioception by desynchronizing waves in the β-band in the motor cortex, aiding in precise force control during movement execution [52].
Conventionally, clinical assessment of proprioceptive acuity is conducted by tests evaluating kinematic and kinetic aspects of movement [53, 54]. The kinematic assessment by means of joint re-positioning accuracy measurement, the threshold to detection of passive motion, and active movement extent discrimination accuracy are widely evaluated in the existing literature [54]. However, the kinetic assessment of proprioception through force sense accuracy measurement has received less attention [55,56,57]. Force sense accuracy refers to a person’s active ability to sense and reproduce muscle tension or force [57, 58]. The assessment of force sense accuracy involves selecting a specific target force level, such as 50% of maximum voluntary isometric contraction and instructing the participant to reproduce this level of force during a muscle contraction at a specific joint angle [59, 60]. The discrepancy between the force produced by the participant and the target force level is then calculated and reported as the error in the sense of force. In the existing literature, the control of force sense has been hypothesized to exist due to an interplay between central feed-forward and peripheral feedback mechanisms [57]. Simon, Garcia [57] suggested that peripheral feedback mechanisms dominate during the initial phases of learning, whereas this dominance switches to feed-forward pathways upon gaining task-specific expertise [61]. In injuries when inherent proprioceptive accuracy is low, a larger dependence on peripheral feedback mechanisms is expected [62, 63]. Under such circumstances, the use of ta** to facilitate force reproduction via peripheral feedback mechanisms makes sense. Docherty and Arnold [58] suggested that any improvement in force reproduction might signify an enhanced ability of a muscle to support the joint during movement, thereby reducing its predisposition towards injury [64].
Despite mounting evidence suggesting the beneficial influence of ta** on proprioception and its gaining popularity, a lack of consensus exists in the literature regarding its efficacy, specifically concerning force sense accuracy. This lack of consensus exists primarily at the level of individual clinical trials. For instance, some individual trials have suggested the beneficial influence of ta** on improving force sense accuracy [49, 65,66,67], whereas others have indicated that ta** does not affect force sense accuracy [52, 57, 68]. Besides, several other outcomes need to be evaluated to determine the overall influence of ta** on force sense accuracy outcomes. For instance, there is a need to evaluate the impact of ta** on force sense from both between- and within-group perspectives. These findings could be significant because the analyses between the groups can provide insights into the contrasting results observed between ta** and both the absence of a comparator and placebo ta**. In contrast, the within-group analyses could explain the magnitude of change in proprioceptive parameters before and after the ta**. Moreover, it is also important to classify the influence of ta** in different population groups (i.e., healthy individuals and individuals with musculoskeletal/ neurological disorders). Evaluating this outcome is essential to understand the effectiveness of ta** in various health conditions and could be helpful for both clinicians and patient population groups. Likewise, it is also crucial to assess separately the influence of different tapes on force sense accuracy. Ta** interventions (i.e., Leuko, Kinesio, athletic, Zinc oxide tape) reported in the literature have been found to exhibit different elastic properties [69]. The literature suggests that different mechanisms are involved in modulating movement kinematics due to a change in the tape’s elasticity [46, 70]. Therefore, it makes sense that the influence of tapes is separately evaluated.
Research aims and questions
-
1.
To investigate the effects of ta** on force sense accuracy in terms of absolute and relative accuracy from between- and within-group analyses.
-
2.
To conduct exploratory subgroup meta-analyses of individual studies to investigate the potential impact of various factors such as study design, health status, ta** elasticity on force sense accuracy.
Material and methods
We followed PRISMA 2020 guidelines to conduct this systematic review and meta-analysis [71]. The checklist is presented in Supplementary Table S1. This systematic review was pre-registered at PROSPERO (CRD42022383616).
Sources of data and search strategy
The systematic literature search was carried out across seven databases (Web of Science, PEDro, Pubmed, EBSCO, Scopus, EMBASE, Psychinfo) and one registry (Cochrane Central Register of Controlled Trials) from January 1946 until December 2022. These databases were chosen based on access provided by the academic organization. The search strategies according to each database have been provided in the Supplementary file. Furthermore, the authors conducted an extra search through the bibliography section of the relevant studies.
Inclusion criteria
The inclusion criteria for the studies to be included in the review were developed according to the PICOS approach (Population, intervention, comparator, outcome of interest, and study design). The inclusion criteria were determined by two researchers (S.G, I.G). The inclusion criteria were as follows:
-
1)
Incorporation of studies involving healthy individuals.
-
2)
Inclusion of studies involving population groups affected by musculoskeletal disorders (such as a sprain, strain, tendinitis, repeated stress injuries, degenerative joint diseases, and traumatic injuries).
-
3)
Inclusion of studies involving population groups affected by neurological disorders (such as stroke, Parkinson’s disease, cerebral palsy, multiple sclerosis, traumatic injuries, degenerative neurological disorders).
-
4)
Inclusion of studies that evaluated the influence of ta** on force sense accuracy. This encompassed various forms of ta**, including tape, Kinesiotape, leuko tape, orthotic tape, adhesive tape, and others.
-
5)
Inclusion of studies that assessed proprioception acuity through the analysis of active and relative force sense accuracy.
-
6)
Inclusion of studies that compared ta** intervention outcomes with a control group utilizing placebo tape and/or no tape.
-
7)
Inclusion of all types of quantitative clinical study designs such as, randomized controlled trials, controlled clinical trials, crossover trials, longitudinal studies, cohort analyses, feasibility studies.
-
8)
Inclusion of studies that achieved more than or equal to 4 on the PEDro quality appraisal scale [72].
-
9)
Inclusion of studies published in peer-reviewed academic journals, theses, and conference proceedings.
-
10)
Inclusion of studies published in English, French, German, or Hindi languages.
The intent behind maintaining a broad scope for the inclusion criteria was to ensure a comprehensive exploration of the subject matter. For example, the decision to encompass individuals with and without medical conditions stemmed from the goal of thoroughly investigating the potential variations in the effects of ta** based on differing health statuses. Similarly, in acknowledging the diversity of study designs in existing research, we recognized the absence of a singular dominant design. By incorporating various study designs, our aim was to encompass a wider array of evidence and insights. Finally, the inclusion of diverse types of tapes was intended to scrutinize the potential distinct effects of these interventions based on their inherent elastic properties.
Selection and extraction of data
The screening of the titles, abstracts, and full texts of the articles were conducted independently by two authors (S.G, I.G). During the screening process, both the authors were blinded from each other. In cases where there were disagreements about the inclusion of pertinent articles, the third author (S.N) participated in discussions to facilitate consensus. The following information was extracted from the articles: author names, country of research, participant information (age, sample size, gender distribution, health status), assessed joint, ta** method, ta** technique, application by physiotherapist, assessment periods, ta** frequency, and results.
Evaluation of the methodological quality
The PEDro quality appraisal scale was used to assess the quality of the studies included in our review [73]. The appraisal by the PEDro scale can be interpreted as follows: studies scoring between 9 to 11 are categorized as “excellent quality”, those with scores between 6 to 8 are considered “good quality”, scores between 4 to 5 indicate “fair quality”, and scores equal to or less than 3 signify “poor quality”. The appraisal of the studies was carried out by two researchers (S.G, I.G) independently. In instances of discrepancies, the researchers engaged in discussions, and if a unanimous decision couldn’t be reached, a third researcher (S.N) was consulted to achieve a consensus.
Data analysis
In the present review, a between-group (ta** vs. no comparator, ta** vs. placebo ta**) and a within-group (pre- vs. post-ta**) random effect meta-analysis was conducted with Comprehensive meta-analysis (V 4.0) [74]. For the between-group analysis, we utilized mean change scores (i.e., post–pre performance outcomes) extracted from the respective studies. The data extracted from the studies were separately distributed and analyzed for force sense, encompassing active and relative accuracy. The meta-analysis outcomes reported comprise weighted and adjusted effect sizes (Hedge’s g), 95% confidence intervals (C.I.), and significance levels. The threshold for the interpretation of effect size were as follows: 0.16 denoted a small effect, 0.38 indicated a medium effect, and 0.76 signified a large effect [75]. Forest plots were generated to illustrate the results. Besides, the included studies’ heterogeneity was quantified using I2 statistics. The threshold for interpreting the heterogeneity with I2 statistics were defined as follows: between 0 and 40% indicated negligible heterogeneity, 30% to 60% denoted moderate heterogeneity, 50% to 90% represented substantial heterogeneity, and 75% to 100% indicated considerable heterogeneity [76]. In the present study, subgroup analyses were conducted based on study design (i.e., repeated measures design, quasi experimental studies), health status (i.e., healthy individuals, individuals with chronic ankle instability), and elasticity of ta** (i.e., elastic, rigid tapes). An assessment of publication bias for the primary outcome was carried out according to the trim and fill procedure by Duval and Tweedie [77]. Additionally, we also conducted “leave-one-out” sensitivity analyses to test the robustness of our findings. The leave-one-out method systematically removes each study from the meta-analysis and re-analyzes the data to assess the influence of individual studies on the overall results [78]. This helps to identify studies that may be driving the results and assess the robustness of the findings. The significance level for the study was set at 0.05.
Included studies
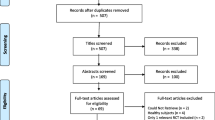
The initial search across seven databases and one registry yielded a total of 7362 articles, which after implementing the PICOS inclusion criteria, were reduced to 11 articles (Fig. 1). Thereafter, qualitative, and quantitative data were extracted from all included studies.

PRISMA flowchart of study selection (made from [79])
Study design
Of the 11 included studies, five studies reported a repeated measures design [49, 52, 65, 80, 81], while four studies reported that they adhered to a case control format within a repeated measures design [57, 66, 82, 83]. Moreover, one study each reported to adhere to a pretest–posttest cross sectional design [68], and a pretest–posttest quasi-experimental design [67].
Methodological quality
The individual PEDro scoring for each included study has been tabulated in Table 1. The average PEDro quality score of the 11 included studies was (5.8 ± 0.9), suggesting the overall quality of the included studies to be “fair”. The two researchers (S.G, I.G) appraised the articles with a 97.3% agreement. In terms of individual scores, one study scored eight [68], seven studies received a score of 6 [49, 52, 57, 65, 66, 80, 82], two studies achieved a score of 5 [81, 83], and one studies attained a score of 4 [67]. The methodological quality across the studies has also been illustrated in Fig. 2.

Illustrating the methodological quality according to the PEDro scale
Publication bias
The incidence of publication bias according to Duval and Tweedie’s trim and fill procedure is shown in Fig. 3. The method identified two missing studies on the right side of the mean effect, whereas no study was missing on the left side. In the analysis, under the random effect model, the point estimate and the 95% C.I. for the combined studies was -0.79, -1.27 to -0.31. Based on the trim and fill procedure, the imputed point estimates are -0.54 (-1.04 to -0.05).

A trim and fill funnel plot illustrating the publication bias. Blue circle: individual studies, red circle: imputed studies, funnel plot: 95% area of the pseudo-confidence intervals, vertical midline: estimated overall effect size (i.e., empirical studies + imputed studies)
Results
Systematic review report
Participants
Among the 11 included studies, data from a total of 279 (128F, 94M) people was reported. The difference in sex distribution was because two studies had not reported these values for their sample [82, 83]. The average age of the entire sample was 24.5 ± 11.7 years. A comprehensive depiction of the health status of the participants featured in this review is provided in Table 2.
Countries
Four of the 11 studies were conducted in Taiwan [52, 65, 66, 82], two in South Korea [49, 83], two in Iran [67, 68], one in Australia [80], one in China [84], and one in USA [57].
Tape
There are three different types of tapes evaluated in the included studies. A total of nine studies used Kinesiotape [49, 52, 57, 65,66,67,68, 82, 84], one used Zinc oxide tape [83], and one used rigid sports tape [80]. As per established literature, Kinesiotape is categorized as an elastic tape [85], whereas zinc oxide and rigid sports tape are classified as rigid tapes [86].
Force sense accuracy assessment
The included studies reported absolute and relative force sense accuracy outcomes. All 11 included studies reported the absolute force sense accuracy values [49, 52, 57, 65,66,67,68, 80, 82,83,84], with an additional subset of five studies also offering insights into relative force sense accuracy values [65, 66, 68, 82, 84].
Joints assessed
Six of the included studies evaluated the efficacy of ta** on the wrist joint [52, 65, 66, 68, 82, 83]. In contrast, only five studies reported the influence of ta** on the ankle joint [49, 57, 67, 80, 84].
Ta** application
Five of the included studies did not report the person who applied the tape [52, 65,66,67,68], and five reported that a physiotherapist applied the ta** [49, 80, 82,83,84]. Furthermore, one study reported that a healthcare practitioner applied the tape [57].
Outcome
The details of the included studies and their respective outcomes are mentioned in Table 3.
Outcomes based on type of comparator
Ta** vs. no comparator
Absolute accuracy: Nine studies compared the efficacy of ta** intervention with no ta** [49, 52, 65, 66, 68, 80,81,82,83]. Two studies reported significant improvement in force sense accuracy outcomes with ta** compared to the absence of a comparator [49, 65]. Additionally, one study reported a significant improvement in force sense accuracy outcomes within their sample of healthy individuals, but not among individuals with medial epicondylitis [82]. Conversely, another study reported a significant improvement in force sense accuracy outcomes within their sample of individuals with medial epicondylitis, but not among healthy individuals [66]. Moreover, five studies did not report any significant differences between the ta** intervention and the absence of a comparator [52, 68, 80, 81, 83].
Relative accuracy: Three studies had compared the efficacy of ta** intervention with no ta** [66, 68, 82]. Two studies reported no significant difference between the ta** and the no ta** group [66, 82]. One study reported a significant improvement in force sense accuracy between their origin to insertion ta** subgroup as compared to the no ta** group [68]. However, no significant differences were observed between insertion to origin ta** and no ta** comparator [68].
Ta** vs. placebo ta**
Absolute accuracy: Five studies had compared the efficacy of ta** intervention with placebo ta** [49, 65, 66, 81, 82]. Among these, two studies reported a significant improvement in force sense accuracy outcomes with ta** compared to the placebo comparator [49, 65]. One study indicated a significant improvement in force sense accuracy outcomes within their sample of healthy individuals but not among those with medial epicondylitis [82]. Furthermore, two studies did not report any significant difference between ta** and the placebo comparator [66, 81].
Relative accuracy: Two studies compared the efficacy of ta** intervention with a placebo comparator [66, 82]. Neither of these studies found a significant difference between the ta** intervention and the placebo comparator.
Pre vs. post differences
Three studies evaluated the within group differences after the application of the ta** intervention [57, 67, 83]. Among these, two studies reported no significant differences in force sense accuracy after the application of ta** [57, 83], while one study reported a significant improvement in force sense accuracy after the ta** application [67].
Meta-analysis report
The meta-analysis findings are detailed in Table 4, Figs. 4 and 5, offering an extensive perspective on the between-group analysis. Similarly, Table 5 and Fig. 6 visually depict the within-group meta-analysis outcomes. Additionally, Table 6 provides an in-depth report on the leave one out sensitivity analysis.

Forest plot in this study illustrates the effect of ta** on absolute force sense improvement in accuracy. Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improvement in force sense accuracy for the no-ta** group, negative effect size: improvement in force sense accuracy for the ta** group

Forest plot illustrating the effect of ta** on relative force sense accuracy. Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improvement in force sense accuracy for the no-ta** group, negative effect size: improvement in force sense accuracy for the ta** group

Forest plot illustrating the within-group effect of ta** on force sense improvement in accuracy. Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: deterioration in force sense accuracy, negative effect size: improvement in force sense accuracy. (FAI: Functional ankle instability)
Sensitivity analysis
A summary of the leave-one-out sensitivity analysis has been provided in Table 6. Specifically, studies were reported if the overall analysis yielded a p-value less than 0.05, and the removal of a specific study increased the p-value above this threshold. Conversely, studies were also reported if the overall analysis yielded a p-value greater than 0.05 and the removal of any study decreased the p-value below this threshold.
Discussion
The current systematic review and meta-analysis aimed to comprehensively evaluate the effect of ta** on force sense accuracy in healthy and patient population groups. Our meta-analysis confirms these findings, as we observed a significant effect improvement in both absolute (Hedge’s g: -0.77) and relative (g: -0.59) force sense accuracy with ta** as compared to no comparator in the between-group analysis. Moreover, we also observed a significant improvement in absolute (g: -0.51) force sense accuracy with ta** as compared to placebo ta**. However, the within-group analysis revealed a non-significant small effect improvement in absolute force sense accuracy. The sub-sections below have discussed our further subgroup analyses concerning various population groups and tape types.
Influence of ta** on different population groups
Our findings suggest that augmentation of proprioceptive afferent by ta** is more beneficial for individuals with poorer inherent proprioception than individuals with good proprioception. The reason being that ta** augmented proprioceptive afferent information might overload the “inherently good” proprioceptive pathways in healthy individuals [33]. In contrast, individuals with poorer proprioception (i.e., medial epicondylitis) might benefit from augmented afferent information [90, 91]. We believe two main reasons might explain this differential result in our study. First, there was a large difference in the number of studies in our meta-analysis that included different population groups. For instance, in the between-group analysis, the influence of ta** was evaluated on healthy individuals within eight studies. In comparison, only two studies evaluated ta**’s impact on individuals with medial epicondylitis. Second, in the analyses of healthy population groups, we did not conduct separate sub-group analyses to assess the differential influence on individuals with excellent and poor inherent proprioception (i.e., inherent force sense accuracy). The analysis was not performed because only one included study had classified their healthy cohort based on their innate proprioceptive levels [52]. Future studies are strongly recommended to organize the proprioceptive level of their population groups to help understand the actual influence of ta** on force sense accuracy among healthy individuals.
Furthermore, ta** improved force sense accuracy in population groups with injuries, such as individuals with medial epicondylitis, lateral epicondylitis, and functional ankle instability. One potential explanation for the improved force sense accuracy in this sample is that ta** may have restricted the injured musculoskeletal tissue to its anatomical limits, leading to an enhanced sense of force at the joint [32]. The work of Seo also supports this hypothesis, who suggested that ta** allows injured ligaments to heal in their proper position, reducing the risk of chronic instability, while non-taped injuries may heal in a stretched, weakened state [92]. Simon, Garcia [57] demonstrated that Kinesiota** compensated for deficits in force sense accuracy in individuals with functional ankle instability (pre-tape: 2.6N, post-tape: 2.2N, 72 h: 1.8N). The authors hypothesized that the Kinesiotape could have allowed their sample to establish a new perceptual trace that allowed them to process the afferent information more efficiently, thereby improving their ability to sense force [57]. Chang, Wang [82] too reported the beneficial influence of ta** among individuals with medial epicondylitis. The authors hypothesized that Kinesiotape could have alleviated deficits in force sense reproduction by stimulating the mechanoreceptors in the skin and fascia to perceive better changes in shear forces, stretch, pressure, and load [82, 93]. In this context, the central nervous system could have utilized this improved perception facilitated by ta** to fine-tune the feed-forward models. This, in turn, contributed to an augmentation in the accuracy of force sensation [57, 82]. Besides, one of our included studies also suggested that perhaps the increments in force sense resulted from the pain-relieving properties of ta** [83]. Studies have indicated that because of noxious muscle input, the excitability at the motor cortex level is reduced together with the inhibition of spinal motor neurons [94, 95]. Under such circumstances, ta** could have modulated the pain through the pain gait control mechanism [96]. This could involve an increased flow of sensory signals from low-threshold peripheral mechanoreceptors, which might have countered the transmission of pain signals to central nociceptive cells, ultimately leading to a reduction in pain perception [97, 98]. Additionally, the observation of significant improvement in force sense accuracy with actual ta** as compared to no ta**, as well as ta** as compared to placebo ta**, suggests that the effects of ta** might go beyond the realm of a simple placebo effect. While the placebo effect of ta** can indeed influence an individual’s perception and performance [99], the fact that actual ta** shows a more pronounced improvement indicates that there might be additional physiological mechanisms at play. Nevertheless, the conclusive determination of ta**’s true effects, potentially extending beyond placebo responses, necessitates future studies.
Influence of ta** elasticity on force sense accuracy
Various tapes have been used in the existing literature to influence force sense accuracy outcomes in healthy and patient population groups. Some studies have directly compared the influence of different types of tapes on proprioceptive results [45, 100, 101]. However, uncertainty still looms regarding which tape is the most effective. The literature suggests that tapes with lower elastic modulus (i.e., high rigidity) function primarily by limiting the range of motion at a joint rather than facilitating its neuromuscular functioning [102, 103]. Rigid tapes are suggested to be beneficial for individuals who need additional stability to participate in certain activities or to protect an injured area.
Nonetheless, the restrictive nature of such rigid tapes has been suggested to predispose someone to higher risks of injury, as the tape can alter joint kinematics, such as excessive talocrural movement restriction [104]. Besides, as these tapes lack sufficient adhesive capabilities to cope with functional activities, their use is repeatedly questioned in sporting and rehabilitation contexts [101, 105]. On the contrary, tapes with high elastic modulus have been reported to support and stabilize the joints without restricting the joint’s range of motion. Due to their increased flexibility, elastic tapes can conform to the body’s contours, allowing for a greater range of motion. This elasticity can be beneficial specifically for individuals who need to perform functional activities. A study included in our review suggested that Kinesiotape differed from conventional rigid tapes in addition to the enhanced elasticity as it also embedded a specialized wave-like grain design [65]. According to the authors, this specialized design and the tape’s elasticity could have facilitated proprioception by exerting a pulling force on the skin while generating space by lifting the underlying fascia and soft tissue [25, 65].
In our between-group meta-analyses, we observed that elastic tapes (p = 0.009) led to a significantly improved absolute force sense accuracy, whereas rigid tapes did not show a significant effect (p = 0.069). Furthermore, when we performed subgroup analyses considering health status, we found a greater degree of enhancement, although not statistically significant, in the accuracy of absolute force sensing among healthy individuals who used elastic tape (effect size: -0.60) compared to those who used rigid tape (effect size: -0.38). We did not perform a comparative analysis on the effectiveness of rigid tape in reducing relative force sense accuracy due to limited available data. Nevertheless, several potential explanations for the observed variance in the degree of force sense accuracy between elastic and rigid tapes can be considered. Firstly, it is possible that healthy individuals who used elastic tape did not require the restrictive support provided by rigid tapes but benefited from the functional support offered by elastic tapes, which improved joint movement and proprioception. Secondly, the smaller number of studies included in the analysis of rigid tapes (only two) compared to elastic tape (six) may have contributed to greater variability in the data or an increased risk of a type II error. Therefore, we recommend that future studies be conducted with high-quality trials and sufficient sample sizes to further investigate and compare the efficacy of elastic and rigid tapes in more detail.
Limitations
The main goal of our study was to understand the impact of ta** on force sense accuracy. However, our analysis had some limitations. Some studies included in our review evaluated the immediate effects of ta** [49, 65,66,67, 82, 83], while others examined the impact of prolonged ta** on force sense accuracy [57, 68]. As our study did not precisely aim to explore the effect of prolonged ta** on proprioception, we did not perform separate analyses to compare the impact of prolonged ta** on force sense accuracy. Studies have shown that prolonged ta** may have a greater effect on proprioception’s kinematic and kinetic aspects than ta** applied immediately [106,107,108]. Therefore, future studies are strongly recommended to evaluate the differential influence of the prolonged application of ta** on force sense accuracy. Secondly, substantial heterogeneity was also prominent regarding the different ta** application methods. This heterogeneity could be an essential aspect the reader should consider while interpreting the results. For instance, some studies included in our review adhered to a specific technique, such as Kenzo Kase’s technique [57, 65, 66, 68, 82], whereas the majority had applied ta** without following any standardized approach [49, 52, 67, 80]. This heterogeneous approach to using tape complicates the understanding regarding which method of ta** is more influential in improving force sense accuracy. Therefore, we recommend that future studies adhere to standardized ta** applications as they can help develop practical, evidence-based guidelines. Thirdly, despite employing a broad inclusion criterion, we did not come across any high-quality, blinded, randomized controlled trials that had assessed the impact of ta** on force sense accuracy. The absence of randomized controlled trials in our analysis could potentially raise concerns about the reliability and validity of our findings. Consequently, we strongly recommend that future studies further expand upon our current findings by evaluating the effects of ta** interventions on force sense accuracy through well-designed, high-quality, blinded randomized controlled trials. Fourthly, while our primary objective was to assess how ta** affects accuracy parameters in force sensing, we did not analyze its impact on other kinetic measures of maximum voluntary contraction, such as dynamometry and surface electromyography. Exploring the effects of ta** on these measures could have provided additional insights relating to the heterogeneity of the results. We recommend that future reviews to examining the impact of ta** on other kinetic indicators as the findings from these studies will enhance our comprehension of how ta** influences proprioceptive control related to force. Another major limitation of our study was that fewer studies were included in our meta-analyses, such as between-group analyses of individuals with medial epicondylitis (i.e., two studies) and within-group analyses of individuals with functional ankle instability (two studies). Fewer studies could increase the chances of a type II error [109]. Again, the reader is advised to infer these results with caution.
Future directions
Although the number of studies incorporating ta** for improving proprioception in healthy and patient population groups has increased in the past decade, a few aspects still warrant exploration. For instance, limited research has evaluated the long-term retention of force sense reproduction after the application of ta** [57, 68]. Conventionally, ta** has been identified as a transient approach that facilitates performance transiently by guiding the movement when it is being worn. However, once its removed, the lack of guidance (see guidance hypothesis [110]) by ta** forces improved accuracy back to initial levels [111]. We presume that an effective means by which this feedback dependency of ta** could be countered by tapering the extent of tactile feedback provided over time. Here, perhaps reducing the length of ta** applied [112], or even the tension with which ta** is used, could reduce the extent of feedback being provided to the performer and allow them to form robust internal feed-forward models concerning the task at hand. Future studies should try to evaluate these outcomes to ascertain whether tapering the feedback by ta** can promote learning in terms of force sense reproduction compared to performance.
Conclusions
Our exploratory meta-analysis of a limited number of studies reports the positive influence of ta** on absolute force sense accuracy outcomes when compared to no compared to both no ta** and placebo ta**. The improvements in relative force sense accuracy was only significant with ta** when compared to no ta**. Collectively, the advancement in accuracy for both relative and absolute force sensing through ta** potentially indicates the potential for improved performance and a lowered risk of injury. Specifically, the improved accuracy in perceiving relative force might facilitate precise fine-tuning of force while engaging in various activities, while the enhanced absolute force perception could suggest accurate application of force. This heightened precision becomes particularly valuable in dynamic high-risk environments where maintaining balance and executing complex movements are necessary.
Moreover, we observed a significant improvement in force sense accuracy for elastic tapes as compared to rigid tapes for absolute force sense accuracy. Unfortunately, due to the predominance of studies with a repeated measures design within our pooled data, and the relatively fewer studies employing cross-sectional or quasi-experimental designs, a comprehensive comparative analysis based on study design could not be performed. Lastly, healthy individuals and individuals with medial epicondylitis were observed to significantly improve their absolute force sense accuracy with ta** when compared to ta**, as compared to no ta**. However, when compared to placebo ta** a significant improvement in force sense accuracy was only observed for healthy individuals.
Despite the sensitivity analyses confirming the robustness of our findings, we recommend our reader interpret these results cautiously as the studies included in our review were of “fair” methodological quality, and high levels of heterogeneity were observed in our meta-analyses. Future studies are recommended to further evaluate the efficacy of ta** on force sense accuracy outcomes in high-quality randomized controlled trials to ascertain the true effects of ta** on force sense accuracy outcomes.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Qin Y, Li M, Han J, Cui G, Du W, Yang K. Research hotspots and trends of Kinesio Ta** from 2011 to 2020: a bibliometric analysis. Environ Sci Pollut Res Int. 2023;30(1):2029–41. https://doi.org/10.1007/s11356-022-22300-9. Epub 2022 Aug 4.
Simon JE. Study of the comparative effectiveness of ankle ta** and ankle wrap** on the prevention of ankle injuries. J Nat Athl Trainers Assoc. 1969;4:6–7.
Grant M-E, Steffen K, Glasgow P, Phillips N, Booth L, Galligan M. The role of sports physiotherapy at the London 2012 Olympic Games. Br J Sports Med. 2014;48(1):63–70.
Cupler ZA, Alrwaily M, Polakowski E, Mathers KS, Schneider MJ. Ta** for conditions of the musculoskeletal system: an evidence map review. Chiropr Man Therap. 2020;28(1):52.
Yoshida A, Kahanov L. The effect of kinesio ta** on lower trunk range of motions. Res Sports Med. 2007;15(2):103–12.
Kim S-Y, Oh D-W, Kim T-Y. Functional ta** technique for chronic back pain and lower extremity pain-McConnell’s approach. J Korean Acad Orthop Man Phys Ther. 2008;14(2):50–9.
Gardner MJ, Parada S, Routt Jr MLC. Internal rotation and ta** of the lower extremities for closed pelvic reduction. J Orthop Trauma. 2009;23(5):361–4.
Franettovich MM, Murley GS, David BS, Bird AR. A comparison of augmented low-Dye ta** and ankle bracing on lower limb muscle activity during walking in adults with flat-arched foot posture. J Sci Med Sport. 2012;15(1):8–13.
Bennell K, Coburn S, Wee E, Green S, Harris A, Forbes A, et al. Efficacy and cost-effectiveness of a physiotherapy program for chronic rotator cuff pathology: a protocol for a randomised, double-blind, placebo-controlled trial. BMC Musculoskelet Disord. 2007;8(1):86.
Delahunt E, McGrath A, Doran N, Coughlan GF. Effect of ta** on actual and perceived dynamic postural stability in persons with chronic ankle instability. Arch Phys Med Rehabil. 2010;91(9):1383–9.
Logan CA, Bhashyam AR, Tisosky AJ, Haber DB, Jorgensen A, Roy A, et al. Systematic review of the effect of ta** techniques on patellofemoral pain syndrome. Sports Health. 2017;9(5):456–61.
Xue X, Chen Y, Mao X, Tu H, Yang X, Deng Z, et al. Effect of kinesio ta** on low back pain during pregnancy: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2021;21(1):1–11.
Kasawara KT, Mapa JMR, Ferreira V, Added MAN, Shiwa SR, Carvas N Jr, et al. Effects of Kinesio Ta** on breast cancer-related lymphedema: a meta-analysis in clinical trials. Physiother Theory Pract. 2018;34(5):337–45.
Capecci M, Serpicelli C, Fiorentini L, Censi G, Ferretti M, Orni C, et al. Postural rehabilitation and Kinesio ta** for axial postural disorders in Parkinson’s disease. Arch Phys Med Rehabil. 2014;95(6):1067–75.
Jaraczewska E, Long C. Kinesio® ta** in stroke: improving functional use of the upper extremity in hemiplegia. Top Stroke Rehabil. 2006;13(3):31–42.
Kwon M, Lee S, Lee J, Lee A, Lee H. The effects of functional ankle ta** on postural stability in elite judo players. Appl Sci. 2022;12(21):10779.
Schiffer T, Möllinger A, Sperlich B, Memmert D. Kinesio ta** and jump performance in elite female track and field athletes. J Sport Rehabil. 2015;24(1):47–50.
Sanioglu A, Ergun S, Erkmen N, Taskin H, Goktepe AS, Kaplan T. The effect of ankle ta** on isokinetic strength and vertical jum** performance in elite taekwondo athletes. Isokinet Exerc Sci. 2009;17(2):73–8.
dos Santos Gloria IP, Politti F, Leal Junior ECP, Lucareli PRG, Herpich CM, Antonialli FC, et al. Kinesio ta** does not alter muscle torque, muscle activity or jum** performance in professional soccer players: a randomized, placebo-controlled, blind, clinical trial. J Back Musculoskelet Rehabil. 2017;30(4):869–77.
Momtazfar P, Ghazalian F, Nikbakht H. Effect of kinesio ta** on hand muscles strength of Karatekaman man. Sport Sciences for Health. 2015;11:257–61.
Crossley K, Cowan SM, Bennell KL, McConnell J. Patellar ta**: is clinical success supported by scientific evidence? Man Ther. 2000;5(3):142–50.
Bishop C, Arnold JB, May T. Effects of ta** and orthoses on foot biomechanics in adults with flat-arched feet. Med Sci Sports Exerc. 2016;48(4):689–96.
Tobin S, Robinson G. The effect of McConnell’s vastus lateralis inhibition ta** technique on vastus lateralis and vastus medialis obliquus activity. Physiotherapy. 2000;86(4):173–83.
Joscha K, Julian M. What is the current level of evidence and the efficacy of medical ta** on circulation, muscle function, correction, pain, and proprioception? Amsterdam: Professional Assignment Project, European School of Physiotherapy, Hogeschool van Amsterdam; 2010.
Kase K, Wallis J, Kase T. Clinical Therapeutic Applications of the Kinesio Ta** Method. Tokyo: Ken Ikai Co Ltd; 2003.
Salsich GB, Brechter JH, Farwell D, Powers CM. The effects of patellar ta** on knee kinetics, kinematics, and vastus lateralis muscle activity during stair ambulation in individuals with patellofemoral pain. J Orthop Sports Phys Ther. 2002;32(1):3–10.
Ernst GP, Kawaguchi J, Saliba E. Effect of patellar ta** on knee kinetics of patients with patellofemoral pain syndrome. J Orthop Sports Phys Ther. 1999;29(11):661–7.
Liu K, Duan Z, Chen L, Wen Z, Zhu S, Qu Q, et al. Short-term effect of different ta** methods on local skin temperature in healthy adults. Front Physiol. 2020;11:488.
Taradaj J, Halski T, Zduńczyk M, Rajfur J, Pasternok M, Chmielewska D, et al. Evaluation of the effectiveness of kinesio ta** application in a patient with secondary lymphedema in breast cancer: a case report. Menopause Rev/Prz Menopauzalny. 2014;13(1):73–7.
Hörmann J, Vach W, Jakob M, Seghers S, Saxer F. Kinesiota** for postoperative oedema – what is the evidence? A systematic review. BMC Sports Sci Med Rehabil. 2020;12(1):14.
Smith MD, Vitharana TN, Wallis GM, Vicenzino B. Response profile of fibular repositioning tape on ankle osteokinematics, arthrokinematics, perceived stability and confidence in chronic ankle instability. Musculoskelet Sci Pract. 2020;50:102272.
Hall EA, Simon JE, Docherty CL. Using ankle bracing and ta** to decrease range of motion and velocity during inversion perturbation while walking. J Athl Train. 2016;51(4):283–90.
Ghai S, Driller M, Ghai I. Effects of joint stabilizers on proprioception and stability: a systematic review and meta-analysis. Phys Ther Sport. 2017;25:65–75.
Morrissey D. Proprioceptive shoulder ta**. J Bodyw Mov Ther. 2000;4(3):189–94.
Cho H-Y, Kim E-H, Kim J, Yoon YW. Kinesio ta** improves pain, range of motion, and proprioception in older patients with knee osteoarthritis: a randomized controlled trial. Am J Phys Med Rehabil. 2015;94(3):192–200.
Konishi Y. Tactile stimulation with Kinesiology tape alleviates muscle weakness attributable to attenuation of Ia afferents. J Sci Med Sport. 2013;16(1):45–8.
Lee D-H, Kim W-J, Oh J-S, Chang M. Ta** of the elbow extensor muscle in chronic stroke patients: comparison between before and after three-dimensional motion analysis. J Phys Ther Sci. 2015;27(7):2101–3.
Ferreira A, Monteiro P, Carvalho P, Moreira C. Influence of two ta**s on the reaction time of the peroneal muscles. In: International conference on biomechanics in sports 2011. 2011. p. 651–4.
Martin PG, Weerakkody N, Gandevia SC, Taylor JL. Group III and IV muscle afferents differentially affect the motor cortex and motoneurones in humans. J Physiol. 2008;586(5):1277–89.
Cimino SR, Beaudette SM, Brown SHM. Kinesio ta** influences the mechanical behaviour of the skin of the low back: a possible pathway for functionally relevant effects. J Biomech. 2018;67:150–6.
Pamuk U, Yucesoy CA. MRI analyses show that kinesio ta** affects much more than just the targeted superficial tissues and causes heterogeneous deformations within the whole limb. J Biomech. 2015;48(16):4262–70.
Yam TTT, Wong MS, Fong SSM. Effect of Kinesio ta** on electromyographic activity of leg muscles during gait in children with developmental coordination disorder: a randomized controlled trial. Medicine. 2019;98(6):e14423.
Yam TTT, Or PPL, Ma AWW, Fong SSM, Wong MS. Effect of Kinesio ta** on Y-balance test performance and the associated leg muscle activation patterns in children with developmental coordination disorder: a randomized controlled trial. Gait Posture. 2019;68:388–96.
Kelly LA, Racinais S, Tanner CM, Grantham J, Chalabi H. Augmented low dye ta** changes muscle activation patterns and plantar pressure during treadmill running. J Orthop Sports Phys Ther. 2010;40(10):648–55.
Long Z, Wang R, Han J, Waddington G, Adams R, Anson J. Optimizing ankle performance when taped: effects of kinesiology and athletic ta** on proprioception in full weight-bearing stance. J Sci Med Sport. 2017;20(3):236–40.
Franettovich Smith MM, Coates SS, Creaby MW. A comparison of rigid tape and exercise, elastic tape and exercise and exercise alone on pain and lower limb function in individuals with exercise related leg pain: a randomised controlled trial. BMC Musculoskelet Disord. 2014;15(1):328.
Sarvestan J, Svoboda Z. Acute effect of ankle Kinesio and athletic ta** on ankle range of motion during various agility tests in athletes with chronic ankle sprain. J Sport Rehabil. 2019;29(5):527–32.
Mostafavifar M, Wertz J, Borchers J. A systematic review of the effectiveness of Kinesio ta** for musculoskeletal injury. Phys Sportsmed. 2012;40(4):33–40.
Han J-T. Immediate effect of calf muscle Kinesio ta** on ankle joint reposition sense and force sense in healthy elderly. 대한물리치료학회지 (JKPT). 2020;32(4):193–7.
Cordova ML, Ingersoll CD, LeBlanc MJ. Influence of ankle support on joint range of motion before and after exercise: a meta-analysis. J Orthop Sports Phys Ther. 2000;30(4):170–82.
Callaghan MJ, McKie S, Richardson P, Oldham JA. Effects of patellar ta** on brain activity during knee joint proprioception tests using functional magnetic resonance imaging. Phys Ther. 2012;92(6):821–30.
Lin Z-M, Yang J-F, Lin Y-L, Cheng Y-C, Hung C-T, Chen C-S, et al. Effect of Kinesio ta** on hand sensorimotor control and brain activity. Appl Sci. 2021;11(22):10522.
Proske UWE. What is the role of muscle receptors in proprioception? Muscle Nerve. 2005;31(6):780–7.
Han J, Waddington G, Adams R, Anson J, Liu Y. Assessing proprioception: a critical review of methods. J Sport Health Sci. 2016;5(1):80–90.
Arnold BL, Docherty CL. Low-load eversion force sense, self-reported ankle instability, and frequency of giving way. J Athl Train. 2006;41(3):233.
Docherty CL, Arnold BL, Hurwitz S. Contralateral force sense deficits are related to the presence of functional ankle instability. J Orthop Res. 2006;24(7):1412–9.
Simon J, Garcia W, Docherty CL. The effect of Kinesio tape on force sense in people with functional ankle instability. Clin J Sport Med. 2014;24(4):289–94.
Docherty CL, Arnold BL. Force sense deficits in functionally unstable ankles. J Orthop Res. 2008;26(11):1489–93.
Amirshakeri B, Khalkhali Zavieh M, Rezasoltani A, Khademi Kalantari KH, Akbarzadeh A. The effect of lower leg sensory impulses on the force sense of knee extensor muscles in healthy adults: the accuracy of sense-of-force studies. J Bodyw Mov Ther. 2019;23(4):739–45.
Turkmen C, Harput G, Kinikli GI, Kose N, Guney DH. Correlation of force sense error test measured by a pressure biofeedback unit and EMG activity of quadriceps femoris in healthy individuals. J Electromyogr Kinesiol. 2019;49:102366.
Stelmach GE. Motor control and motor learning: the closed-loop perspective. In: JAS Kelso, editor. Human motor behavior—an introduction. Hillsdale: Lawrence Erlbaum Associates; 1982. p 93–95.
Harris DJ, Vine SJ, Wilson MR, McGrath JS, LeBel ME, Buckingham G. Action observation for sensorimotor learning in surgery. Br J Surg. 2018;105(13):1713–20.
Takeoka A, Arber S. Functional local proprioceptive feedback circuits initiate and maintain locomotor recovery after spinal cord injury. Cell Rep. 2019;27(1):71–85.e3.
Proske U, Gandevia SC. The proprioceptive senses: their roles in signaling body shape, body position and movement, and muscle force. Physiol Rev. 2012;92(4):1651–97.
Chang H-Y, Chou K-Y, Lin J-J, Lin C-F, Wang C-H. Immediate effect of forearm Kinesio ta** on maximal grip strength and force sense in healthy collegiate athletes. Phys Ther Sport. 2010;11(4):122–7.
Chang HY, Cheng SC, Lin CC, Chou KY, Gan SM, Wang CH. The effectiveness of Kinesio ta** for athletes with medial elbow epicondylar tendinopathy. Int J Sports Med. 2013;34(11):1003–6.
Momeni-lari H, Ghasemi M, Khademi-kalantari K, Akbarzadeh-baghban A. The short-term effects of Kinesio tape on joint position sense, sense of force and postural control in patients with functional ankle instability. J Babol Univ Med Sci. 2018;20(8):51–5.
Hosseini SM, Salehi Dehno N, Rezaiian F, Kalantari KK, Tabatabaee SM. Effect of kinesio ta** direction on force sense in wrist flexor muscles in healthy persons. Res Sports Med. 2019;27(3):273–82.
Matheus JPC, Zille RR, Gomide Matheus LB, Lemos TV, Carregaro RL, Shimano AC. Comparison of the mechanical properties of therapeutic elastic tapes used in sports and clinical practice. Phys Ther Sport. 2017;24:74–8.
Jung H-j, Lee J-y, Hwang J-k, Choi B-r. Comparison of efficiency of elastic and non-elastic ta** on induced quadriceps fatigue by knee extension exercise. J Phys Ther Sci. 2017;29(12):2199–200.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88:105906.
Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003;83(8):713–21.
Moseley AM, Rahman P, Wells GA, Zadro JR, Sherrington C, Toupin-April K, et al. Agreement between the Cochrane risk of bias tool and Physiotherapy Evidence Database (PEDro) scale: a meta-epidemiological study of randomized controlled trials of physical therapy interventions. PLoS One. 2019;14(9):e0222770.
Borenstein M. Comprehensive meta‐analysis software. Systematic reviews in health research: meta‐analysis in context. 2022. pp. 535–48.
Brydges CR. Effect size guidelines, sample size calculations, and statistical power in gerontology. Innov Aging. 2019;3(4):igz036.
Higgins JPT, Green S. Cochrane handbook for systematic reviews of interventions. 2008.
Duval S, Tweedie R. Trim and fill: a simple funnel-plot–based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000;56(2):455–63.
Fangfang Z, Lili L, Chundong Z, Shiliang J, Zubing M, Tian L. Association of metabolic syndrome and its components with risk of stroke recurrence and mortality. Neurology. 2021;97(7):e695.
Haddaway NR, Page MJ, Pritchard CC, McGuinness LA. PRISMA2020: an R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and Open Synthesis. Campbell Syst Rev. 2022;18(2):e1230.
Hopper DM, Grisbrook TL, Finucane M, Nosaka K. Effect of ankle ta** on angle and force matching and strength of the plantar flexors. Phys Ther Sport. 2014;15(4):254–60.
Li P, Wei Z, Zeng Z, Wang L. Acute effect of kinesio tape on postural control in individuals with functional ankle instability following ankle muscle fatigue. Front Physiol. 2022;13. https://www.frontiersin.org/articles/10.3389/fphys.2022.980438, https://doi.org/10.3389/fphys.2022.980438. ISSN=1664-042X.
Chang H-Y, Wang C-H, Chou K-Y, Cheng S-C. Could forearm Kinesio ta** improve strength, force sense, and pain in baseball pitchers with medial epicondylitis? Clin J Sport Med. 2012;22(4):327–33.
Lee W-H, Kwon O-Y, Yi C-H, Jeon H-S, Ha S-M. Effects of ta** on wrist extensor force and joint position reproduction sense of subjects with and without lateral epicondylitis. J Phys Ther Sci. 2011;23(4):629–34.
Lee S-M, Lee J-H. The immediate effects of ankle balance ta** with kinesiology tape on ankle active range of motion and performance in the Balance Error Scoring System. Phys Ther Sport. 2017;25:99–105.
Kim JY, Kim SY. Effects of kinesio tape compared with non-elastic tape on hand grip strength. J Phys Ther Sci. 2016;28(5):1565–8.
Verhagen EALM, van der Beek AJ, van Mechelen W. The effect of tape, braces and shoes on ankle range of motion. Sports Med. 2001;31(9):667–77.
Lee J-h, Yoo W-g. Treatment of chronic Achilles tendon pain by Kinesio ta** in an amateur badminton player. Phys Ther Sport. 2012;13(2):115–9.
Hopper DM, McNair P, Elliott BC. Landing in netball: effects of ta** and bracing the ankle. Br J Sports Med. 1999;33(6):409.
Kase K, Hashimoto T, Okane T. Kinesio perfect ta** manual. Amazing ta** therapy to eliminate pain and muscle disorders. 1996:1998.
Hosp S, Bottoni G, Heinrich D, Kofler P, Hasler M, Nachbauer W. A pilot study of the effect of Kinesiology tape on knee proprioception after physical activity in healthy women. J Sci Med Sport. 2015;18(6):709–13.
Birmingham TB, Kramer JF, Inglis JT, Mooney CA, Murray LJ, Fowler PJ, et al. Effect of a neoprene sleeve on knee joint position sense during sitting open kinetic chain and supine closed kinetic chain tests. Am J Sports Med. 1998;26(4):562–6.
Denegar CR, Miller SJ 3rd. Can chronic ankle instability be prevented? Rethinking management of lateral ankle sprains. J Athl Train. 2002;37(4):430–5.
Schleip R. Fascial plasticity–a new neurobiological explanation: part 1. J Bodyw Mov Ther. 2003;7(1):11–9.
Le Pera D, Graven-Nielsen T, Valeriani M, Oliviero A, Di Lazzaro V, Tonali PA, et al. Inhibition of motor system excitability at cortical and spinal level by tonic muscle pain. Clin Neurophysiol. 2001;112(9):1633–41.
Proske U, Gregory JE, Morgan DL, Percival P, Weerakkody NS, Canny BJ. Force matching errors following eccentric exercise. Hum Mov Sci. 2004;23(3):365–78.
Aytar A, Ozunlu N, Surenkok O, Baltacı G, Oztop P, Karatas M. Initial effects of kinesio® ta** in patients with patellofemoral pain syndrome: a randomized, double-blind study. Isokinet Exerc Sci. 2011;19(2):135–42.
Banerjee G, Briggs M, Johnson MI. The effects of kinesiology ta** on experimentally-induced thermal and mechanical pain in otherwise pain-free healthy humans: a randomised controlled repeated-measures laboratory study. PLoS One. 2019;14(12):e0226109.
Melzack R, Katz J. The gate control theory: reaching for the brain. Pain Psychol Perspect. 2004:13–34.
Sawkins K, Refshauge K, Kilbreath S, Raymond J. The placebo effect of ankle ta** in ankle instability. Med Sci Sports Exerc. 2007;39(5):781–7.
Brogden CM, Marrin K, Page RM, Greig M. The efficacy of elastic therapeutic tape variations on measures of ankle function and performance. Phys Ther Sport. 2018;32:74–9.
Grütters K, Narciss S, Beaudette SM, Oppici L. Reducing lumbar flexion in a repetitive lifting task: Comparison of leukotape and kinesio tape and their effect on lumbar proprioception. 2022.
Shaheen AF, Bull AMJ, Alexander CM. Rigid and Elastic ta** changes scapular kinematics and pain in subjects with shoulder im**ement syndrome; an experimental study. J Electromyogr Kinesiol. 2015;25(1):84–92.
Bozkurt T, Kilic RT, Yosmaoglu HB. The effect of elastic therapeutic ta** and rigid ta** on pain, functionality, and tissue temperature in lumbar radiculopathy: a randomized controlled study. Somatosens Mot Res. 2021;38(4):373–80.
Hals T-MV, Sitler MR, Mattacola CG. Effect of a semi-rigid ankle stabilizer on performance in persons with functional ankle instability. J Orthop Sports Phys Ther. 2000;30(9):552–6.
Forbes H, Thrussell S, Haycock N, Lohkamp M, White M. The effect of prophylactic ankle support during simulated soccer activity. J Sport Rehabil. 2013;22(3):170–6.
Kim J, Kim S, Lee J. Longer application of kinesio ta** would be beneficial for exercise-induced muscle damage. J Exerc Rehabil. 2016;12(5):456.
Ucuzoglu ME, Unver B, Sarac DC, Cilga G. Similar effects of two different external supports on wrist joint position sense in healthy subjects: a randomized clinical trial. Hand Surgery and Rehabilitation. 2020;39(2):96–101.
Alawna M, Mohamed AA. Short-term and long-term effects of ankle joint ta** and bandaging on balance, proprioception and vertical jump among volleyball players with chronic ankle instability. Phys Ther Sport. 2020;46:145–54.
Button KS, Ioannidis J, Mokrysz C, Nosek BA, Flint J, Robinson ESJ, et al. Power failure: why small sample size undermines the reliability of neuroscience. Nat Rev Neurosci. 2013;14(5):365–76.
Park J-H, Shea CH, Wright DL. Reduced-frequency concurrent and terminal feedback: a test of the guidance hypothesis. J Mot Behav. 2000;32(3):287–96.
Pinto BL, Beaudette SM, Brown SHM. Tactile cues can change movement: an example using tape to redistribute flexion from the lumbar spine to the hips and knees during lifting. Hum Mov Sci. 2018;60:32–9.
Yu R, Yang Z, Witchalls J, Adams R, Waddington G, Han J. Kinesiology tape length and ankle inversion proprioception at step-down landing in individuals with chronic ankle instability. J Sci Med Sport. 2021;24(9):894–9.
Acknowledgements
Not applicable.
Funding
Open access funding provided by Karlstad University. This work was partly funded by the German Research Foundation (DFG, Deutsche Forschungsgemeinschaft) as part of Germany’s Excellence Strategy—EXC 2050/1—Project ID 390696704—Cluster of Excellence “Centre for Tactile Internet with Human-in-the-Loop” (CeTI) of Technische Universität Dresden.
Author information
Authors and Affiliations
Contributions
SG conceptualized the study and was responsible for designing and implementing the research. SG, IG acted as the independent reviewers and performed the statistical analysis. SG, SN wrote the initial version of the manuscript. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
PRISMA checklist. Figure S1. Forest plot illustrating the effect of ta** on absolute force sense accuracy (repeated measures design). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improved force sense accuracy for the no-ta** group, negative effect size: improved force sense accuracy for the ta** group. Figure S2. Forest plot illustrating the effect of ta** on absolute force sense accuracy (elastic tape). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improved force sense accuracy for the no-ta** group, negative effect size: improved force sense accuracy for the elastic ta** group. Figure S3. Forest plot illustrating the effect of ta** on absolute force sense accuracy (rigid tape). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improved force sense accuracy for the no-ta** group, negative effect size: improved force sense accuracy for the rigid ta** group. Figure S4. Forest plot illustrating the effect of ta** on absolute force sense accuracy (healthy individuals). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improved force sense accuracy for the no-ta** group, negative effect size: improved force sense accuracy for the ta** group. Figure S5. Forest plot illustrating the effect of ta** on absolute force sense accuracy (individuals with medial epicondylitis). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improved force sense accuracy for the no-ta** group, negative effect size: improved force sense accuracy for the ta** group. Figure S6. Forest plot illustrating the effect of ta** on absolute force sense accuracy (healthy individuals with elastic tape). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improved force sense accuracy for the no-ta** group, negative effect size: improved force sense accuracy for the elastic ta** group. Figure S7. Forest plot illustrating the effect of ta** on absolute force sense accuracy (healthy individuals with rigid tape). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improved force sense accuracy for the no-ta** group, negative effect size: improved force sense accuracy for the rigid ta** group. Figure S8. Forest plot illustrating the effect of ta** on relative force sense accuracy (repeated measures design). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improved force sense accuracy for the no-ta** group, negative effect size: improved force sense accuracy for the ta** group. Figure S9. Forest plot illustrating the effect of ta** on relative force sense accuracy (healthy individuals). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improved force sense accuracy for the no-ta** group, negative effect size: improved force sense accuracy for the ta** group. Figure S10. Forest plot illustrating the effect of ta** on relative force sense accuracy (individuals with medial epicondylitis). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improved force sense accuracy for the no-ta** group, negative effect size: improved force sense accuracy for the ta** group. Figure S11. Forest plot illustrating the effect of ta** on absolute force sense accuracy. Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improved force sense accuracy for the placebo ta** group, negative effect size: improved force sense accuracy for the ta** group. Figure S12. Forest plot illustrating the effect of ta** on absolute force sense accuracy (healthy individuals). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improved force sense accuracy for the placebo ta** group, negative effect size: improved force sense accuracy for the ta** group. Figure S13. Forest plot illustrating the effect of ta** on absolute force sense accuracy (individuals with medial epicondylitis). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improved force sense accuracy for the placebo ta** group, negative effect size: improved force sense accuracy for the ta** group. Figure S14. Forest plot illustrating the effect of ta** on relative force sense accuracy. Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improved force sense accuracy for the placebo ta** group, negative effect size: improved force sense accuracy for the ta** group. Figure S15. Forest plot illustrating the effect of ta** on relative force sense accuracy (healthy individuals). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improved force sense accuracy for the placebo ta** group, negative effect size: improved force sense accuracy for the ta** group. Figure S16. Forest plot illustrating the effect of ta** on relative force sense accuracy (individuals with medial epicondylitis). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improved force sense accuracy for the placebo ta** group, negative effect size: improved force sense accuracy for the ta** group. Figure S17. Forest plot illustrating the effect of ta** on absolute force sense accuracy (repeated measures design). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: deterioration in force sense accuracy, negative effect size: improvement in force sense accuracy. Figure S18. Forest plot illustrating the effect of ta** on absolute force sense accuracy (elastic tape). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: deterioration in force sense accuracy, negative effect size: improvement in force sense accuracy. Figure S19. Leave-one-out sensitivity analysis for between group analysis for absolute force sense accuracy (ta** vs. no comparator). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improvement in force sense accuracy for the no-ta** group, negative effect size: improvement in force sense accuracy for the ta** group. Figure S20. Leave-one-out sensitivity analysis for between group analysis for absolute force sense accuracy (repeated measures design, ta** vs. no comparator). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improvement in force sense accuracy for the no-ta** group, negative effect size: improvement in force sense accuracy for the ta** group. Figure S21. Leave-one-out sensitivity analysis for between group analysis for absolute force sense accuracy (elastic tape, elastic ta** vs. no comparator). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improvement in force sense accuracy for the no-ta** group, negative effect size: improvement in force sense accuracy for the elastic ta** group. Figure S22. Leave-one-out sensitivity analysis for between group analysis for absolute force sense accuracy (rigid tape, rigid ta** vs. no comparator). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improvement in force sense accuracy for the no-ta** group, negative effect size: improvement in force sense accuracy for the rigid ta** group. Figure S23. Leave-one-out sensitivity analysis for between group analysis for absolute force sense accuracy (healthy individuals, ta** vs. no comparator). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improvement in force sense accuracy for the no-ta** group, negative effect size: improvement in force sense accuracy for the ta** group. Figure S24. Leave-one-out sensitivity analysis for between group analysis for absolute force sense accuracy (individuals with medial epicondylitis, ta** vs. no comparator). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improvement in force sense accuracy for the no-ta** group, negative effect size: improvement in force sense accuracy for the ta** group. Figure S25. Leave-one-out sensitivity analysis for between group analysis for absolute force sense accuracy (healthy individuals, elastic ta** vs. no comparator). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improvement in force sense accuracy for the no-ta** group, negative effect size: improvement in force sense accuracy for the elastic ta** group. Figure S26. Leave-one-out sensitivity analysis for between group analysis for absolute force sense accuracy (healthy individuals, rigid ta** vs. no comparator). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improvement in force sense accuracy for the no-ta** group, negative effect size: improvement in force sense accuracy for the rigid ta** group. Figure S27. Leave-one-out sensitivity analysis for between group analysis for relative force sense accuracy (ta** vs. no comparator). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improvement in force sense accuracy for the no-ta** group, negative effect size: improvement in force sense accuracy for the ta** group. Figure S28. Leave-one-out sensitivity analysis for between group analysis for relative force sense accuracy (repeated measures design, ta** vs. no comparator). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improvement in force sense accuracy for the no-ta** group, negative effect size: improvement in force sense accuracy for the ta** group. Figure S29. Leave-one-out sensitivity analysis for between group analysis for relative force sense accuracy (healthy individuals, ta** vs. no comparator). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improvement in force sense accuracy for the no-ta** group, negative effect size: improvement in force sense accuracy for the ta** group. Figure S30. Leave-one-out sensitivity analysis for between group analysis for relative force sense accuracy (individuals with medial epicondylitis, ta** vs. no comparator). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improvement in force sense accuracy for the no-ta** group, negative effect size: improvement in force sense accuracy for the ta** group. Figure S31. Leave-one-out sensitivity analysis for between group analysis for absolute force sense accuracy (ta** vs. placebo ta** comparator). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improvement in force sense accuracy for the placebo ta** group, negative effect size: improvement in force sense accuracy for the ta** group. Figure S32. Leave-one-out sensitivity analysis for between group analysis for absolute force sense accuracy (healthy individuals, ta** vs. placebo ta** comparator). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improvement in force sense accuracy for the placebo ta** group, negative effect size: improvement in force sense accuracy for the ta** group. Figure S33. Leave-one-out sensitivity analysis for between group analysis for absolute force sense accuracy (individuals with medial epicondylitis, ta** vs. placebo ta** comparator). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improvement in force sense accuracy for the placebo ta** group, negative effect size: improvement in force sense accuracy for the ta** group. Figure S34. Leave-one-out sensitivity analysis for between group analysis for relative force sense accuracy (ta** vs. placebo ta** comparator). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improvement in force sense accuracy for the placebo ta** group, negative effect size: improvement in force sense accuracy for the ta** group. Figure S35. Leave-one-out sensitivity analysis for between group analysis for relative force sense accuracy (healthy individuals, ta** vs. placebo ta** comparator). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improvement in force sense accuracy for the placebo ta** group, negative effect size: improvement in force sense accuracy for the ta** group. Figure S36. Leave-one-out sensitivity analysis for between group analysis for relative force sense accuracy (individuals with medial epicondylitis, ta** vs. placebo ta** comparator). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: improvement in force sense accuracy for the placebo ta** group, negative effect size: improvement in force sense accuracy for the ta** group. Figure S37. Leave-one-out sensitivity analysis for within group analysis for absolute force sense accuracy. Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: deterioration in force sense accuracy, negative effect size: improvement in force sense accuracy. Figure S38. Leave-one-out sensitivity analysis for within group analysis for absolute force sense accuracy (repeated measures design). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: deterioration in force sense accuracy, negative effect size: improvement in force sense accuracy. Figure S39. Leave-one-out sensitivity analysis for within group analysis for absolute force sense accuracy (elastic tape). Black boxes: individual weighted effect sizes, whiskers: 95% confidence intervals, red diamond: pooled weighted effect size and 95% confidence interval, positive effect size: deterioration in force sense accuracy, negative effect size: improvement in force sense accuracy. Search strategy for individual databases.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ghai, S., Ghai, I. & Narciss, S. Influence of ta** on force sense accuracy: a systematic review with between and within group meta-analysis. BMC Sports Sci Med Rehabil 15, 138 (2023). https://doi.org/10.1186/s13102-023-00740-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13102-023-00740-1