
Abstract
Background
Current evidence suggests that the magnetic resonance imaging (MRI)-based vertebral bone quality (VBQ) score is a good parameter for evaluating bone quality. We aimed to assess whether the VBQ score can predict the occurrence of postoperative cage subsidence after oblique lumbar interbody fusion (OLIF) surgery.
Methods
Patients (n = 102) who had undergone single-level OLIF with a minimal follow-up for 1 year were reviewed in this study. Demographic and radiographic data of these patients were collected. Cage subsidence was defined as ≥ 2 mm of cage migration into the inferior endplate, superior endplate, or both. Further, the MRI-based VBQ score was measured on T1-weighted images. Moreover, univariable and multivariable binary logistic regression analyses were performed. Meanwhile, Pearson analysis was used to evaluate the correlation among the VBQ score, average lumbar dual-energy X-ray absorptiometry (DEXA) T-score, and degree of cage subsidence. Furthermore, ad-hoc analysis was used along with receiver operating characteristic curve analysis to assess the predictive ability of the VBQ score and average lumbar DEXA T-score.
Results
Of 102 participants, cage subsidence was observed in 39 (38.24%) patients. According to the univariable analysis, patients with subsidence had older age, higher antiosteoporotic drug use, larger disk height change, a more concave morphology of inferior and superior endplates, higher VBQ score, and lower average lumbar DEXA T-score compared to patients without subsidence. In the multivariable logistic regression analysis, a higher VBQ score was significantly associated with an increased risk of subsidence (OR = 23.158 ± 0.849, 95% CI 4.381–122.399, p < 0.001), and it was the only significant and independent predictor of subsidence after OLIF. Moreover, the VBQ score was moderately correlated with the average lumbar DEXA T-score (r = − 0.576, p < 0.001) and the amount of cage subsidence (r = 0.649, p < 0.001). Furthermore, this score significantly predicted cage subsidence with an accuracy of 83.9%.
Conclusions
The VBQ score can independently predict postoperative cage subsidence in patients undergoing OLIF surgery.
Similar content being viewed by others


Background
In the literature, many studies have reported favorable clinical outcomes of mini-open oblique lateral interbody fusion (OLIF) in patients with lumbar degenerative disk disease [1, 2]. Moreover, it is possible to perform OLIF through the physiological gap between the aorta and psoas major by making a small anterior–lateral skin incision [3]. This method avoids the invasion into the paraspinal musculature, is less invasive, and reduces the risk of injury to the lumbar plexus; in addition, it offers various advantages, such as minimal trauma and speedy recovery [4]. Indirect decompression of the neural elements is achieved using an enlarged cage to distract the narrow intervertebral space and the foramen [5]. Therefore, the degree of cage subsidence may have a greater impact on the clinical outcomes of OLIF than those of other posterior approach techniques where decompression is achieved directly.
Cage subsidence is one of the most commonly reported complications in OLIF, which leads to various compromised clinical outcomes, such as disk/foraminal height loss, column lordosis reduction, neuroforaminal stenosis, and recurrence of radiculopathy. In the relevant literature, low bone mineral density (BMD) has been considered as one of the main risk factors of cage subsidence, and it could be used as one of its predictors [6, 7]. The gold standard for BMD assessment and osteopenia or osteoporosis diagnosis is dual-energy X-ray absorptiometry (DEXA). However, previous studies have confirmed that DEXA cannot help in accurate BMD assessment of patients with lumbar degenerative diseases. Quantitative computed tomography (qCT) could be used as an alternative method for a more accurate assessment of bone quality. However, qCT is not routinely performed because it is expensive [8, 9]. Recently, a novel method of determining MRI-based vertebral bone quality (VBQ) score was proposed for evaluating the quality and fat infiltration of trabecular bone [10]. This score was found to significantly correlate with BMD assessed using the DEXA scan, which may help reduce investigation costs and radiation hazards [11, 12]. Moreover, the VBQ score has been recognized as an independent risk factor for fragility fractures, and it predicts the occurrence of cage subsidence and reoperation after transforaminal lumbar interbody fusion surgery [13, 14].
However, to the best of our knowledge, no studies have evaluated the relationship between the VBQ score and the occurrence of cage subsidence after OLIF surgery to date. Thus, this retrospective study aimed to assess whether the VBQ score can be used to predict the occurrence of cage subsidence after OLIF surgery.
Methods
Patients
We retrospectively collected the medical records of patients who underwent OLIF surgery between February 2019 and October 2021 after obtaining approval from our institutional review board. Patients who underwent single-level OLIF surgery with ≥ 1 year of follow-up were included in this study. In contrast, patients with a history of congenital spinal anomalies, those who did not undergo any surgery for degenerative lumbar disease, those with endplate sclerosis on preoperative CT scan, and those with an endplate injury on immediate postoperative CT scan were excluded from the study. All surgical procedures were consecutively performed at our center by one of the two spine fellowship-trained neurosurgeons.
Surgical procedure
All procedures were performed by the same group of spine surgeons in accordance with the standard guidelines. After intubation with general anesthesia, the patient was placed in the right lateral recumbent position. A 4–6 cm skin incision was made from the anterior to the center of the marked disk. Further, the retroperitoneal space was accessed by blunt dissection of the abdominal muscle. Moreover, a series of dilators was placed to create an anatomically oblique lateral corridor. After the removal of the disk and preparation of the intradiscal plate, a cage of appropriate size (Clydesdale Spine System, Medtronic, or Oracle Systems, Synthes) filled with demineralized bone matrix and artificial bone material was placed in the optimal position. Subsequently, two screws (Medtronic Sofamor Danek USA, Inc.) were inserted into the lateral side of the vertebral body near the endplate and locked with a single rod. Finally, the abdominal muscles and the incised skin were closed.
Data collection and radiographic assessment
Basic data of the participants, including age, sex, body mass index (BMI), age-adjusted Charlson Comorbidity Index (CCI) score, hypertension, history of smoking and drinking, chronic steroid use, antiosteoporotic drug use for 1 year perioperatively, diagnosis, surgical level, fusion status, and follow-up time, were retrospectively collected. Lumbar CT scans and X-rays of the participants were obtained pre- and postoperatively, i.e., on day 1 and 3, 6, and 12 months postoperatively. We used the average T-scores of lumbar vertebrae 1–4 obtained by dual-energy X-ray absorptiometry (DEXA) scans. Moreover, data related to cage height, length, and position were collected. The primary outcome of this study was cage subsidence, which was defined as ≥ 2 mm of cage migration into the inferior endplate, superior endplate, or both at the final follow-up (Fig. 1A) [15]. Cage position was defined by the percentage of the distance between the anterior metal marker of the cage and the anterior edge of the vertebral body at the length of the caudal endplate [16] (Fig. 1B). The endplate morphology was classified into flat and concave types (Fig. 1C). Disk height was expressed in terms of the Farfan index [13] (Fig. 1D). The change in disk height was defined by the difference between the midline distance of the superior and inferior endplates, and it was assessed before and after 1 day of operation.

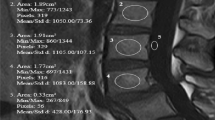
A Cage subsidence is indicated as ≥ 2 mm sinking of the cage into the superior endplate. B The cage position is calculated as \(\frac{a}{b} \times 100\%\) (a, the distance between the anterior metal marker and the leading edge of the caudal endplate; b, he length of caudal endplate). C Classification of the disk space morphology on MRI scan (c, concave; d, fat). D The disk height is calculated as \(\frac{e + f}{g} \times 100\%\) on a lumbar X-ray (lateral view) (e, anterior disk height; f, posterior disk height; g, sagittal disk width). E Representative image of the ROI used to calculate the VBQ score
VBQ score calculation
The VBQ score was calculated using the method described by Ehresman et al. [10]. Moreover, a midsagittal T1-weighted MRI of the lumbar spine was performed without inversion recovery or contrast. Regions of interest (ROIs) were placed in the medullary portions of L1–4 vertebral bodies and in the cerebrospinal fluid (CSF) space at the level of L3 (Fig. 1E). Subsequently, the VBQ score was calculated by dividing the mean signal intensity (SI) value in the vertebral bodies of L1–4 by the signal intensity in the cerebrospinal fluid.
Statistics
Continuous variables were analyzed using the independent t-test, whereas categorical variables were compared using the chi-square test. We included all clinically and radiologically significant risk factors in the multivariable logistic regression model. Moreover, Pearson’s correlation test was performed to assess the relationship among the VBQ score, cage subsidence, and lumbar T-score. A receiver operating characteristic (ROC) curve was used for ad-hoc analysis to identify cutoff values by the Youden index and calculate the area under the curve (AUC) of the significant continuous variables. SPSS statistical software version 20 (IBM Corp.) was used to perform statistical analyses. A p-value of < 0.05 was considered statistically significant.
Results
In total, 102 patients were included in this study based on the inclusion and exclusion criteria. The demographic and clinical data of these patients are shown in Table 1. Overall, 39 (38.24%) patients with cage subsidence were included in the subsidence group, and their average subsidence was 3.59 ± 1.22 mm. The remaining 63 patients (61.76%) were included in the nonsubsidence group, and their average subsidence was 1.13 ± 1.56 mm. Comparison between the subsidence and nonsubsidence groups revealed that patients with subsidence were significantly older (62.10 ± 9.60 vs. 58.09 ± 8.82 years, p = 0.034) and had undergone more number of antiosteoporotic drug treatments [10 (25.64%) vs. 6 (9.52%), p = 0.030] than patients without subsidence. Additionally, patients with subsidence had a larger disk height change (3.51 ± 1.14 vs. 2.99 ± 1.05 mm, p = 0.022), more concave morphology of inferior endplate [1 (1.56%) vs. 14 (22.22%), p = 0.006] and superior endplate [2 (5.13%) vs. 16 (25.40%), p = 0.009] higher VBQ score (3.83 ± 0.82 vs. 2.98 ± 0.39 mm, p < 0.001), and a lower average lumbar DEXA T-score (− 1.76 ± 0.98 vs. − 1.02 ± 1.08 mm, p = 0.001) than patients without subsidence. In contrast, there were no significant differences in terms of other factors, including sex, BMI, age-adjusted CCI score, hypertension, history of smoking and drinking, chronic use of steroid, diagnosis, follow-up time, surgical level, cage height, cage length, cage position, preoperative and immediate postoperative disk height, and fusion status.
All statistically significant factors according to the univariable analysis were included in the multivariable logistic regression model. Detailed results of the effect size of each variable in the multivariable analysis are presented in Table 2. Notably, a higher VBQ score [odds ratio (OR): 23.158 ± 0.849, 95% confidence interval (CI) 4.381–122.399, p < 0.001] was the only variable that significantly predicted subsidence. We also conducted correlation analyses to evaluate the correlation among the VBQ score, average lumbar DEXA T-score, and amount of cage subsidence; the results of these analyses are shown in Table 3. A moderate correlation was found between the VBQ score and the amount of cage subsidence (r = 0.649, p < 0.001). Similarly, the VBQ score was moderately correlated with the average lumbar DEXA T-score (r = − 0.576, p < 0.001). However, a fair correlation was found between the average lumbar DEXA T-score and the amount of cage subsidence (r = − 0.418, p < 0.001).
Further, the ad-hoc analysis was performed to determine the cutoff values of the VBQ score and average lumbar DEXA T-score. Moreover, ROC curves were created for the preoperative VBQ score and average lumbar DEXA T-score as predictors for cage subsidence. Notably, the AUCs of the VBQ score and average lumbar DEXA T-score were 0.839 (95% CI 0.756–0.922) and 0.695 (95% CI 0.591–0.798), respectively. The cutoff value of the VBQ score was 3.435, with a sensitivity of 69.23% and a specificity of 88.89% (Fig. 2A). The cutoff value of the average lumbar DEXA T-score was − 0.75, with a sensitivity of 84.62% and a specificity of 44.44% (Fig. 2B).

ROC curve analysis and AUC of the VBQ score (A) and average lumbar DEXA T-score (B) for predicting cage subsidence. Red dots indicate the cutoff points determined by the Youden index
Discussion
In the present study, we retrospectively examined 102 patients who underwent OLIF surgery and identified 39 cases of cage subsidence. Some risk factors have been identified including old age, large number of antiosteoporotic drug treatments, increased disk height change, concave endplate morphology, low lumbar DEXA T-score, and high VBQ score. Notably, the novelty of this study is that we found that the VBQ score can independently predict postoperative cage subsidence in patients undergoing OLIF surgery. Cage subsidence is a clinical phenomenon that manifests as sinking of the cage into the vertebrae through an adjacent endplate. This phenomenon may lead to progressive disk height narrowing and poor clinical outcomes. Various subsidence rates have been reported in previous studies, and they range from 11 to 46.7% [3, 5, 17, 18]. In the present study, cage subsidence following OLIF was observed in 38.24% of the participants. This relatively higher subsidence rate in our study can be attributed to the use of a low threshold (≥ 2 mm of cage migration into adjacent endplates) to define subsidence. Moreover, the incidence of subsidence in the present study (38.24%) was much lower than that reported by Kotheeranurak et al. (46.7%), probably because we excluded patients with intraoperative endplate violations [18]. According to the reports in the relevant literature, the probability of occurrence of intraoperative endplate violations ranges from 16.8 to 33.1%, and these violations increase the risk of cage subsidence [19,20,21]. Therefore, careful management of the surgical procedure is crucial to ensure that the endplate is completely undamaged.
Apart from the endplate violation, the risk factors that were thought to be associated with cage subsidence have been widely discussed in previous studies, including poor bone quality, over distraction, cage position and design, endplate sclerosis, age, and the presence or absence of the supplemental fixation [20, 22, 23]. In the present study, based on univariable analysis, patients with subsidence had older age, underwent greater number of antiosteoporotic drug treatments, had greater disk height change, and had a more concave endplate morphology compared to those without subsidence. Notably, bone quality and muscle mass tend to reduce with aging. According to a previous study, older patients are more likely to develop cage subsidence owing to the negative effects of age on bone microstructure [24]. Moreover, the use of antiosteoporotic drugs was recommended postoperatively for patients undergoing lumbar fusion surgery in order to reduce the subsidence rate [25]. However, in our study, the number of patients treated with antiosteoporosis therapy was more in the subsidence group, indicating that such patients have worse bone quality and are more prone to cage subsidence. Over the distraction is another important factor contributing to cage subsidence. Notably, it has been reported that disk space distraction may cause cage subsidence in anterior cervical and lumbar fusion cases [26, 27]. A large distraction leads to a large change in disk height, which further causes a significant increase in the compressive force between the cage–endplate interface. The selection of cage height has been suggested to be determined according to the disk height measured preoperatively. Furthermore, previous reports have proven that cage morphology affects cage subsidence [28, 29]. In particular, it has been believed that a flat endplate has better interface contact with an OLIF cage at the surface. A well-matched endplate-cage surface provides more even stress distribution and a larger area for endplate coverage, decreasing the incidence of cage subsidence. In contrast, a concave endplate provides a reduced contact area and leads to stress concentration, increasing the incidence of cage subsidence [30].
Low BMD has been proven to be a critical risk factor for cage subsidence. Proper preoperative assessment of bone quality helps in develo** a reasonable surgical plan and taking relevant preventive measures to improve surgical outcomes and reduce associated complications. Although DEXA is recognized as the gold standard for bone density assessment, it is associated with many issues that can lead to inaccurate evaluations, such as spinal deformities, overlying soft tissue, previous compression fractures, bowel content, osteophytes, and aortic atherosclerosis [31,32,33]. In the present study, the average lumbar DEXA T-score was fairly correlated with the amount of cage subsidence; this finding was similar to the findings of previous studies, which reported that BMD assessed by DEXA scanning had a significantly weak correlation with the amount of cage subsidence. Therefore, this score is not a good predictor for cage subsidence in OLIF surgery and demonstrates low accuracy (0.695). Previous studies have reported that Hounsfield units calculated by qCT may help assess bone quality more accurately than the DEXA T-score [9, 34]. Notably, low Hounsfield units indicate low BMD, which further indicates a higher incidence of develo** cage subsidence [7, 35]. However, qCT is more expensive and associated with a high risk of radiological hazards; hence, it is not suitable for use in routine examinations.
Previous studies have examined the MRI-based VBQ score to assess bone quality [10, 36]. In particular, the use of this score is inexpensive and completely radiation-free. Osteoporotic bone is usually characterized by trabecular atrophy and local adipocyte replacement on histological analysis [37]. The use of the VBQ score is based on the theory that more atrophy and fatty infiltration in osteoporotic trabecular bone causes higher SI on T1-weighted images. Owing to the easy-to-teach methodology and rapid results unaffected by confounding factors, the measurement of this score has shown good reproducibility and reliability, demonstrating that this is a practical tool for clinical use [14, 38]. In previous studies, the use of the VBQ score was verified against the use of DEXA to identify osteoporotic bone and to independently predict the risk of fragility fractures, cage subsidence, and vertebral compression fracture in patients with spine metastases [13, 39, 40]. In the present study, the VBQ score was moderately correlated with the average lumbar DEXA T-score and amount of cage subsidence. This score is known to be an accurate indicator of bone quality; in addition, it is known to facilitate the identification of osteoporotic bone. More importantly, the VBQ score was found to be a significant independent predictor of cage subsidence after OLIF surgery according to the multivariable logistic regression analysis in our study. Patients with VBQ scores higher than the threshold are approximately 23 times more likely to experience subsidence than those with lower scores. Moreover, the VBQ score predicts cage subsidence better than the average lumbar DEXA T-score, with an accuracy of 0.839. This difference may be attributed to the fact that the VBQ score is a site-specific bone density measure that directly reflects vertebral bone quality at the weight-bearing site while excluding factors affecting whole-region standard DEXA measurement, making its assessment more precise than that of the DEXA T-score. Notably, endplate bone quality—a novel site-specific MRI-based bone quality assessment proposed by Jone et al. [41] could predict severe cage subsidence after standalone lateral lumbar interbody fusion even better than the VBQ score. These findings suggest that the VBQ score should be adopted in clinical practice for patients with OLIF surgery in order to improve the efficacy and safety of treatment.
This study has several limitations. First, the retrospective design was subject to certain biases, such as the selection bias in the data collection and the potential observer-expectancy bias. Second, the relatively small cohort from a single health center may explain the lack of statistical significance of some previously identified risk factors for cage subsidence in our multivariable logistic regression analysis. Finally, some important laboratory examination parameters were not assessed in the present study, including calcium, phosphorus, lipids, and cholesterol levels. A previous study reported that patient physiology affects the VBQ score and found a higher VBQ score in patients with hyperlipidemia and healthy bones [42].
Conclusion
The VBQ scoring method can be used to evaluate bone quality with good effectiveness and accuracy and to independently predict postoperative cage subsidence in patients undergoing OLIF surgery. Preoperative measurement of the VBQ score should be considered to identify high-risk patients and take timely precautions to minimize complications.
Availability of data and materials
Data will be available upon request to the corresponding author.
Abbreviations
- VBQ:
-
Vertebral bone quality
- MRI:
-
Magnetic resonance imaging
- OLIF:
-
Oblique lumbar interbody fusion
- BMD:
-
Bone mineral density
- DEXA:
-
Dual-energy X-ray absorptiometry
- CT:
-
Computed tomography
- BMI:
-
Body mass index
- CCI:
-
Charlson Comorbidity Indexs
- ROI:
-
Regions of interest
- CSF:
-
Cerebrospinal fluid
- SI:
-
Signal intensity
- ROC:
-
Receiver operating characteristic
- AUC:
-
Area under the curve
References
Mehren C, Mayer HM, Zandanell C, Siepe CJ, Korge A. The oblique anterolateral approach to the lumbar spine provides access to the lumbar spine with few early complications. Clin Orthop Relat Res. 2016;474(9):2020–7.
Silvestre C, Mac-Thiong JM, Hilmi R, Roussouly P. Complications and morbidities of mini-open anterior retroperitoneal lumbar interbody fusion: oblique lumbar interbody fusion in 179 patients. Asian Spine J. 2012;6(2):89–97.
** C, Jaiswal MS, Jeun SS, Ryu KS, Hur JW, Kim JS. Outcomes of oblique lateral interbody fusion for degenerative lumbar disease in patients under or over 65 years of age. J Orthop Surg Res. 2018;13(1):38.
** J, Ryu KS, Hur JW, Seong JH, Kim JS, Cho HJ. Comparative study of the difference of perioperative complication and radiologic results: MIS-DLIF (minimally invasive direct lateral lumbar interbody fusion) versus MIS-OLIF (minimally invasive oblique lateral lumbar interbody fusion). Clin Spine Surg. 2018;31(1):31–6.
Frisch RF, Luna IY, Brooks DM, Joshua G, O’Brien JR. Clinical and radiographic analysis of expandable versus static lateral lumbar interbody fusion devices with two-year follow-up. J Spine Surg. 2018;4(1):62–71.
Wu H, Cheung JPY, Zhang T, Shan Z, Zhang X, Liu J, et al. The role of hounsfield unit in intraoperative endplate violation and delayed cage subsidence with oblique lateral interbody fusion. Glob Spine J. 2021. https://doi.org/10.1177/21925682211052515.
** Z, Mummaneni PV, Wang M, Ruan H, Burch S, Deviren V, et al. The association between lower Hounsfield units on computed tomography and cage subsidence after lateral lumbar interbody fusion. Neurosurg Focus. 2020;49(2):E8.
Choi MK, Kim SM, Lim JK. Diagnostic efficacy of Hounsfield units in spine CT for the assessment of real bone mineral density of degenerative spine: correlation study between T-scores determined by DEXA scan and Hounsfield units from CT. Acta Neurochir. 2016;158(7):1421–7.
Zou D, Sun Z, Zhou S, Zhong W, Li W. Hounsfield units value is a better predictor of pedicle screw loosening than the T-score of DXA in patients with lumbar degenerative diseases. Eur Spine J. 2020;29(5):1105–11.
Ehresman J, Pennington Z, Schilling A, Lubelski D, Ahmed AK, Cottrill E, et al. Novel MRI-based score for assessment of bone density in operative spine patients. Spine J. 2020;20(4):556–62.
Roch PJ, Celik B, Jackle K, Reinhold M, Meier MP, Hawellek T, et al. Combination of vertebral bone quality scores from different magnetic resonance imaging sequences improves prognostic value for the estimation of osteoporosis. Spine J. 2022;23:305.
Razzouk J, Ramos O, Ouro-Rodrigues E, Samayoa C, Wycliffe N, Cheng W, et al. Comparison of cervical, thoracic, and lumbar vertebral bone quality scores for increased utility of bone mineral density screening. Eur Spine J. 2022. https://doi.org/10.1007/s00586-022-07484-5.
Hu YH, Yeh YC, Niu CC, Hsieh MK, Tsai TT, Chen WJ, et al. Novel MRI-based vertebral bone quality score as a predictor of cage subsidence following transforaminal lumbar interbody fusion. J Neurosurg Spine. 2022;37:654.
Ehresman J, Schilling A, Yang X, Pennington Z, Ahmed AK, Cottrill E, et al. Vertebral bone quality score predicts fragility fractures independently of bone mineral density. Spine J. 2021;21(1):20–7.
Park KH, Chung HW, Lee HD, Jeon CH, Koh JH, Chung NS. Cage obliquity and radiological outcomes in oblique lateral interbody fusion. Spine. 2022. https://doi.org/10.1097/BRS.0000000000004507.
Landham PR, Don AS, Robertson PA. Do position and size matter? An analysis of cage and placement variables for optimum lordosis in PLIF reconstruction. Eur Spine J. 2017;26(11):2843–50.
Tempel ZJ, McDowell MM, Panczykowski DM, Gandhoke GS, Hamilton DK, Okonkwo DO, et al. Graft subsidence as a predictor of revision surgery following stand-alone lateral lumbar interbody fusion. J Neurosurg Spine. 2018;28(1):50–6.
Kotheeranurak V, Jitpakdee K, Lin GX, Mahatthanatrakul A, Singhatanadgige W, Limthongkul W, et al. Subsidence of interbody cage following oblique lateral interbody fusion: an analysis and potential risk factors. Glob Spine J. 2021. https://doi.org/10.1177/21925682211067210.
Satake K, Kanemura T, Nakashima H, Yamaguchi H, Segi N, Ouchida J. Cage subsidence in lateral interbody fusion with transpsoas approach: intraoperative endplate injury or late-onset settling. Spine Surg Relat Res. 2017;1(4):203–10.
Tohmeh AG, Khorsand D, Watson B, Zielinski X. Radiographical and clinical evaluation of extreme lateral interbody fusion: effects of cage size and instrumentation type with a minimum of 1-year follow-up. Spine. 2014;39(26):E1582–91.
Shiga Y, Orita S, Inage K, Sato J, Fujimoto K, Kanamoto H, et al. Evaluation of the location of intervertebral cages during oblique lateral interbody fusion surgery to achieve sagittal correction. Spine Surg Relat Res. 2017;1(4):197–202.
Liu J, Ding W, Yang D, Wu H, Hao L, Hu Z, et al. Modic changes (MCs) associated with endplate sclerosis can prevent cage subsidence in oblique lumbar interbody fusion (OLIF) stand-alone. World Neurosurg. 2020;138:e160–8.
Ohiorhenuan IE, Walker CT, Zhou JJ, Godzik J, Sagar S, Farber SH, et al. Predictors of subsidence after lateral lumbar interbody fusion. J Neurosurg Spine. 2022. https://doi.org/10.3171/2022.1.SPINE201893.
Campbell PG, Cavanaugh DA, Nunley P, Utter PA, Kerr E, Wadhwa R, et al. PEEK versus titanium cages in lateral lumbar interbody fusion: a comparative analysis of subsidence. Neurosurg Focus. 2020;49(3):E10.
Samtani RG, Bernatz JT, Harrison R, Roy S, Gupta S, O’Brien JR. The effect of alendronate on subsidence after lateral transpsoas interbody fusion: a preliminary report. Int J Spine Surg. 2019;13(3):289–95.
Truumees E, Demetropoulos CK, Yang KH, Herkowitz HN. Effects of disc height and distractive forces on graft compression in an anterior cervical discectomy model. Spine. 2002;27(22):2441–5.
Mobbs RJ, Phan K, Malham G, Seex K, Rao PJ. Lumbar interbody fusion: techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP. LLIF ALIF J Spine Surg. 2015;1(1):2–18.
Pappou IP, Cammisa FP Jr, Girardi FP. Correlation of end plate shape on MRI and disc degeneration in surgically treated patients with degenerative disc disease and herniated nucleus pulposus. Spine J. 2007;7(1):32–8.
Park MK, Kim KT, Bang WS, Cho DC, Sung JK, Lee YS, et al. Risk factors for cage migration and cage retropulsion following transforaminal lumbar interbody fusion. Spine J. 2019;19(3):437–47.
Hu Z, He D, Gao J, Zeng Z, Jiang C, Ni W, et al. The influence of endplate morphology on cage subsidence in patients with stand-alone oblique lateral lumbar interbody fusion (OLIF). Glob Spine J. 2021. https://doi.org/10.1177/2192568221992098.
Girardi FP, Parvataneni HK, Sandhu HS, Cammisa FP Jr, Grewal H, Schneider R, et al. Correlation between vertebral body rotation and two-dimensional vertebral bone density measurement. Osteoporos Int. 2001;12(9):738–40.
Muraki S, Yamamoto S, Ishibashi H, Horiuchi T, Hosoi T, Orimo H, et al. Impact of degenerative spinal diseases on bone mineral density of the lumbar spine in elderly women. Osteoporos Int. 2004;15(9):724–8.
Rumancik S, Routh RH, Pathak RD, Burshell AL, Nauman EA. Assessment of bone quantity and distribution in adult lumbar scoliosis: new dual-energy x-ray absorptiometry methodology and analysis. Spine. 2005;30(4):434–9.
Hiyama A, Sakai D, Katoh H, Nomura S, Sato M, Watanabe M. Comparative study of cage subsidence in single-level lateral lumbar interbody fusion. J Clin Med. 2022;11(5):1374.
Ran L, **e T, Zhao L, Huang S, Zeng J. Low Hounsfield units on computed tomography are associated with cage subsidence following oblique lumbar interbody fusion (OLIF). Spine J. 2022;22(6):957–64.
Bandirali M, Di Leo G, Papini GD, Messina C, Sconfienza LM, Ulivieri FM, et al. A new diagnostic score to detect osteoporosis in patients undergoing lumbar spine MRI. Eur Radiol. 2015;25(10):2951–9.
Meunier P, Aaron J, Edouard C, Vignon G. Osteoporosis and the replacement of cell populations of the marrow by adipose tissue: a quantitative study of 84 iliac bone biopsies. Clin Orthop Relat Res. 1971;80:147–54.
Salzmann SN, Okano I, Jones C, Zhu J, Lu S, Onyekwere I, et al. Preoperative MRI-based vertebral bone quality (VBQ) score assessment in patients undergoing lumbar spinal fusion. Spine J. 2022;22(8):1301–8.
Ehresman J, Schilling A, Pennington Z, Gui C, Chen X, Lubelski D, et al. A novel MRI-based score assessing trabecular bone quality to predict vertebral compression fractures in patients with spinal metastasis. J Neurosurg Spine. 2019;32:499.
Haffer H, Muellner M, Chiapparelli E, Moser M, Dodo Y, Zhu J, et al. Bone quality in patients with osteoporosis undergoing lumbar fusion surgery: analysis of the MRI-based vertebral bone quality score and the bone microstructure derived from microcomputed tomography. Spine J. 2022;22(10):1642–50.
Jones C, Okano I, Arzani A, Dodo Y, Moser M, Reisener MJ, et al. The predictive value of a novel site-specific MRI-based bone quality assessment, endplate bone quality (EBQ), for severe cage subsidence among patients undergoing standalone lateral lumbar interbody fusion. Spine J. 2022;22(11):1875–83.
Aynaszyan S, Devia LG, Udoeyo IF, Badve SA, DelSole EM. Patient physiology influences the MRI-based vertebral bone quality score. Spine J. 2022;22(11):1866–74.
Acknowledgements
Not applicable.
Funding
The authors acknowledge the funding support from the National Natural Science Foundation of China (Nos. 82072434, 82272546), the Sichuan Science and Technology Program (2021YFS0218), Research Development Program of North Sichuan Medical College (CBY20-QA-Y24), and Research Development Plan of the Affiliated Hospital of North Sichuan Medical College (2022JC020). These organizations had no involvements in the study design, collection, analysis, or interpretation of data; in the writing of the manuscript; or in the decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
YH and QC conceptualized and designed the study and drafted the initial manuscript. QL, CZ, JW, RW, HD, and ZW carried out the initial analyses and reviewed and revised the manuscript. GF and LL coordinated and supervised data collection and critically reviewed and revised the manuscript for important intellectual content. All authors have approved the final manuscript for submission and agree to be accountable for all aspects of the work.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the ethics committee of West China Hospital of Sichuan University, and informed consent was obtained from the patients.
Consent for publication
The patients provided written consent for the publication of their clinical details and clinical images. A copy of the written consent form is available for review by the editor of this journal.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Huang, Y., Chen, Q., Liu, L. et al. Vertebral bone quality score to predict cage subsidence following oblique lumbar interbody fusion. J Orthop Surg Res 18, 258 (2023). https://doi.org/10.1186/s13018-023-03729-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-023-03729-1