
Abstract
Background
The main types of PD-L1 in the blood include soluble PD-L1 (sPD-L1), exosomal PD-L1 (exoPD-L1), and PD-L1 in circulating tumor cells (CTCs). However, the predictive and prognostic values of these three indicators in patients with non-small cell lung cancer (NSCLC) undergoing immune checkpoint inhibitor (ICI) therapy are unclear, warranting a systematic meta-analysis.
Methods
A systematic literature search was performed in the PubMed, Cochrane Library, and Embase databases. The pooled hazard ratio (HR) and 95% confidence interval (CI) values were extracted from the included studies to investigate the correlation between the three PD-L1 indicators and overall survival (OS) or progression-free survival (PFS). The Newcastle–Ottawa Scale (NOS) was used to examine the quality of the included studies. Subgroup analyses were employed to investigate the heterogeneity. The publication bias of the included studies was assessed using Begg's and Egger's tests. P < 0.05 was regarded as significantly different.
Results
The pooled results revealed that high pre-treatment sPD-L1 levels were significantly associated with inferior OS (HR = 2.32, 95% CI = 1.68–3.18, P < 0.001) and PFS (HR = 2.52, 95% CI = 1.72–3.68, P < 0.001). However, dynamic changes in sPD-L1 after immunotherapy were not statistically significant for OS (HR = 1.46, 95% CI = 0.65–3.26, P > 0.05) or PFS (HR = 1.62, 95% CI = 0.92–2.86, P > 0.05). Meanwhile, the upregulated pre-treatment exoPD-L1 levels were significantly associated with poor PFS (HR = 4.44, 95% CI = 2.87–6.89, P < 0.001), whereas the post-treatment dynamic upregulation of exoPD-L1 was significantly correlated with superior PFS (HR = 0.36, 95% CI = 0.24–0.54, P < 0.001) and OS (HR = 0.20, 95% CI = 0.07–0.53, P < 0.001). For PD-L1 in CTCs, the pooled results indicated that PD-L1 expression in CTCs was not significantly correlated with OS (HR = 0.75, 95% CI = 0.49–1.13, P = 0.170) and PFS (HR = 0.79, 95% CI = 0.59–1.06, P = 0.12).
Conclusions
Blood-based PD-L1 analysis is a potential strategy for predicting treatment efficacy and prognosis in patients with cancer.
Similar content being viewed by others

Background
Among the malignant tumors, lung cancer, a global public health issue, is the most frequent cause of tumor-related deaths globally [1]. Small cell lung cancer and non-small cell lung cancer (NSCLC) are the two types of lung cancer based on their histology, with NSCLC accounting for about 85% of all lung cancer cases [1]. Although there have been recent breakthroughs in the diagnosis and treatment of cancer, the overall 5-year survival rate for all NSCLC patients remains at 24.6%. Patients with stage I and stage IV have 5-year survival rates of 65% and 5%, respectively [2].
Immune checkpoint inhibitors (ICIs) have improved the survival outcomes of patients with cancer [3]. The US Food and Drug Administration recently approved ICIs to manage NSCLC [4]. Currently, ICIs serve as the first-line and second-line treatments for NSCLC [5, 6]. ICIs have been developed to target immune checkpoint molecules, such as programmed cell death protein 1 (PD-1) and programmed cell death ligand 1 (PD-L1), which are critical for regulating anti-tumor immune responses [7]. The interaction of PD-L1 with PD-1 suppresses T-cell activity and proliferation, resulting in immunological tolerance. Pembrolizumab, an anti-PD-1 antibody, is used to treat patients with NSCLC exhibiting high PD-L1 expression in tumor tissue [8]. However, clinical studies have reported that only 15%–30% of patients achieve favorable outcomes with ICIs [9]. Some patients experience immune-related adverse reactions [10]. Therefore, it is essential to identify biomarkers to assess treatment efficacy and disease prognosis, as well as to screen patients who will benefit from ICI therapy. Tissue PD-L1 (tPD-L1) expression is the most common biomarker for assessing the efficacy and prognosis of ICIs in NSCLC [11]. Previous studies have suggested that highly expressed tPD-L1 improves the clinical prognosis of patients with tumors undergoing ICI therapy [12, 13]. However, recent studies have reported that several individuals with high tPD-L1 expression do not respond to immunotherapy. In contrast, some patients with low tPD-L1 expression had long-term efficacy [14]. A recent meta-analysis revealed that tPD-L1 alone is not an appropriate molecular biomarker for identifying eligible patients for immunotherapy in routine clinical practice [15]. Furthermore, the detection of PD-L1 involves tissue sampling from patients with cancer. Repeated tissue biopsy analysis is challenging for patients with advanced lung cancer. Cancer develops over time due to dynamic molecular changes and harbors escape mutations and epigenetic modifications [16, 17]. This can result in therapy resistance and disease progression, which cannot be evaluated using a single biopsy.
The use of blood-based biopsies to analyze PD-L1 expression in patients with cancer can overcome the challenges associated with the use of solid tumor biopsies. Compared with tissue biopsies, blood-based biopsy techniques have several advantages, including ease of sampling and reproducible monitoring of the dynamic biological changes in vivo [18]. Some studies have reported that tumor cells and immune cells can both release PD-L1 into the bloodstream [19]. Recent studies have revealed that three blood-based PD-L1 indicators, namely soluble PD-L1 (sPD-L1), exosomal PD-L1 (exoPD-L1), and PD-L1 in circulating tumor cells (CTCs), are linked to prognosis in patients with cancer [20,21,22]. Several studies have shown that the elevated pre-treatment sPD-L, PD-L1 in CTCs, and exoPD-L1 levels are negatively correlated with the prognosis of patients with NSCLC undergoing immunotherapy [23,24,25]. The dynamic upregulation of exoPD-L1 and positive PD-L1 expression in CTCs (PD-L1+ CTCs) after immunotherapy were significantly and positively correlated with progression-free survival (PFS) [26, 27]. However, Tiako Meyo et al. reported that upregulated post-treatment levels of sPD-L were not significantly correlated with overall survival (OS) [28]. The roles of these three blood-based PD-L1 indicators in determining the prognosis of patients with NSCLC before and after immunotherapy are unclear. Thus, this study performed a meta-analysis to investigate if the three blood-based PD-L1 indicators are correlated with the prognosis of patients with NSCLC undergoing ICI therapy.
Methods
Protocol and registration
The recommended reporting criteria for the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines were followed to perform the meta-analysis. The study protocol was prospectively registered at PROSPERO (CRD42023402077) and is available at https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42023402077.
Search strategy
Relevant literature in the English language published up to February 23, 2023, was retrieved from the PubMed, Embase, and Cochrane Library databases. The following keywords were used: "non-small cell lung cancer," "lung cancer," "lung tumor," "lung neoplasm," "immune checkpoint inhibitor," "PD-1," "PD-L1," "anti-PD-1," "PD-L1," "programmed death 1 receptor," "programmed death ligand 1," "cytotoxic T lymphocyte antigen 4," "CTLA-4," "blood," "circulating tumor cell," "PD-L1," "soluble PD-L1," "exosomal PD-L1," "circulating PD-L1," "PD-L1 in CTCs," "sPD-L1," and "exoPD-L1." The references in the reviews were manually searched to identify additional related articles.
Inclusion criteria
Studies on patients with pathologically diagnosed primary or metastatic NSCLC; studies on patients undergoing ICI mono-therapy or ICI com-therapy (chemotherapy or targeted therapy); studies evaluating the correlation between PD-L1-based blood markers (PD-L1 in CTCs, sPD-L1, and exoPD-L1) and OS/PFS of patients with NSCLC; studies reporting the hazard ratio (HR) and 95% confidence interval (CI). If the HR was not directly available from studies, it was extracted from the Kaplan–Meier curve. When the univariate and multivariate analysis results were provided simultaneously, only the multivariate analysis results were extracted.
Exclusion criteria
Case reports, reviews, meta-analyses, conference abstracts, and letters; studies in which the full text was not available for download; studies that included animal experiments; studies in non-English language.
Quality assessment
Based on selection, comparability, and outcomes, the quality of the included studies was evaluated using the Newcastle–Ottawa scale (NOS). The NOS quality score ranged from 0 to 9. Studies with NOS scores of ≥ 7 and < 7 were categorized as high-quality and low-quality studies, respectively [29].
Data extraction
Information, such as the name of the first author, the publication year, the region, the sample size, the age, the gender, the cancer stage, the cut-off value, the time point, the study design, and the outcome, was retrieved from each included study. Two authors (Qian Cui and Dong Wang) independently extracted data from univariate and multivariate analyses with HR and 95% CI for OS or PFS. Any controversy was addressed via discussion.
Statistical analysis
The HR and 95% CIs were extracted to assess the association between these three blood-based PD-L1 indicators and survival outcomes of patients with NSCLC undergoing ICI therapy. Additionally, the association between clinicopathologic features and survival outcomes was evaluated by the HR and 95% CI. The HR values of > 1 and < 1 were considered adverse and favorable prognoses, respectively. Cochran's q-test and I2 combined values were applied to analyze the heterogeneity of the results [30]. P > 0.10 and I2 < 50% indicated low-level heterogeneity [29]. Subgroup analysis was utilized to investigate the heterogeneity of the studies. Furthermore, Begg's and Egger's tests were employed to assess publication bias. Differences were considered significant at P < 0.05. All statistical analyses were performed using Stata 15.1 software.
The HR and 95% CIs were extracted to assess the association between these three blood-based PD-L1 indicators and survival outcomes of patients with NSCLC undergoing ICI therapy. Additionally, the association between clinicopathologic features and survival outcomes were evaluated by the HR and 95% CI.
Results
Literature screening
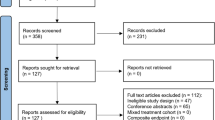
Literature searched in the PubMed, Embase, and Cochrane Library databases yielded 521 studies. Of these, 490 studies were excluded as they were duplications, animal studies, commentaries, and incomplete full texts. The complete texts of the remaining 36 articles were comprehensively evaluated. Of these, 22 studies were excluded, and 14 studies were included in this meta-analysis [23,24,25,26,27,28, 31,32,33,34,35,36,37,38]. The flow chart is illustrated in Fig. 1.

PRISMA flowchart for screening the literature
Study characteristics and quality evaluation
As shown in Table 1, the analysis included 14 trials performed between 2018 and 2022 involving 928 patients with NSCLC. Of these, seven, six, and one studies were performed in Asia, Europe, and America, respectively. Most of the published studies were prospective studies, while only one was a retrospective study. Among the studies included in the meta-analysis, seven, six, and two studies evaluated sPD-L1, PD-L1 in CTCs, and exoPD-L1, respectively. Regarding treatment duration, the pre-treatment sPD-L1 levels were evaluated in six studies, while the dynamic changes in the post-treatment sPD-L1 levels were evaluated in only two studies. Meanwhile, the pre-treatment and post-treatment PD-L1 levels in CTCs were evaluated in four and two studies, respectively. Furthermore, two studies evaluated the pre-treatment exoPD-L1 levels, while one study evaluated dynamic changes in the post-treatment exoPD-L1 levels. The NOS quality score was ≥ 7 and < 7 for 12 and 2 studies, respectively.
Correlation between sPD-L1 and prognosis of patients with NSCLC undergoing ICI therapy
As shown in Fig. 2a, seven studies involving 554 patients with NSCLC undergoing ICI therapy examined the correlation between sPD-L1 and OS. The pooled results revealed that high levels of sPD-L1 were significantly correlated with worse OS (HR = 2.11, 95% CI 1.59–2.80, P < 0.001), and a significant heterogeneity was not observed among studies (I2 = 0%, P = 0.677). As shown in Fig. 2b, five studies involving 493 patients with NSCLC undergoing ICI therapy revealed the correlation between sPD-L1 and PFS. The pooled results demonstrated that high blood levels of sPD-L1 were negatively correlated with PFS (HR = 2.14, 95% CI 1.59–2.88, P < 0.001), and these studies had low-level heterogeneity (I2 = 0%, p = 0.443).

Forest plots of sPD-L1 versus OS/PFS in NSCLC patients undergoing ICI therapy. a–b, sPD-L1 expression versus OS/PFS; Costantini (2018a) and Tiako Meyo (2020a) examined the pre-treatment levels of sPD-L1; Costantini (2018b) and Tiako Meyo (2020b) examined the dynamic changes in the post-treatment sPD-L1 levels
Subgroup analysis was performed based on the correlation of sPD-L1 with OS and PFS according to the time point, sample size, and region. No significant heterogeneity was observed in most subgroups (Table 2). Stratified analysis revealed that high pre-treatment levels of sPD-L1 were remarkably correlated with poorer OS (HR = 2.32, 95% CI 1.68–3.18, P < 0.001; Table 2, Fig. 3a) and PFS (HR = 2.52, 95% CI 1.72–3.68, P < 0.001; Table 2, Fig. 3b). However, after immunotherapy, the dynamic upregulation of sPD-L1 levels was not significantly linked to OS (HR = 1.46, 95% CI = 0.65–3.26, P > 0.05; Table 2, Fig. 3a) and PFS (HR = 1.62, 95% CI = 0.92–2.86, P > 0.05; Table 2, Fig. 3b). Furthermore, moderate heterogeneity was observed in the subgroups of post-treatment sPD-L1 and OS (I2 = 43.3%, p = 0.171).

Subgroup analysis of sPD-L1 levels versus OS/PFS after different treatment durations
Correlation between CTC-PD-L1 and prognosis in patients with NSCLC undergoing ICI therapy
As shown in Fig. 4a, four studies involving 209 patients with NSCLC treated with ICI therapy examined the correlation between PD-L1 expression in CTCs and OS. Pooled analysis of these studies indicated no significant association between PD-L1 expression in CTCs and OS (HR = 0.75, 95% CI 0.49–1.13, P = 0.170). A moderate level of heterogeneity was observed among studies (I2 = 33.5%, P = 0.185). As shown in Fig. 4b, six studies involving 247 patients examined the correlation between PD-L1 expression in CTCs and PFS. The pooled results found that NSCLC patients with PD-L1+ CTCs appeared to have a longer PFS than those with negative PD-L1 expression in CTCs, but this difference did not achieve statistical significance (HR = 0.79; 95% CI 0.59–1.06, P = 0.12). A low level of heterogeneity was observed between studies (I2 = 20.6%, P = 0.266).

Forest plots of PD-L1 expression on CTCs and OS/PFS in patients undergoing ICI therapy. a–b: PD-L1 expression in CTCs versus OS/PFS; Guibert (2018a) represented the data with a cut-off value of 1%; Guibert (2018b) represented the data with a cut-off value of 5%; Guibert (2018c) represented the data with a cut-off value of 10%
Subgroup analysis of OS and PFS according to time point revealed that PD-L1 expression in CTCs before treatment was linked to a lower HR than PD-L1 expression in CTCs after treatment. Additionally, the pre-treatment or post-treatment PD-L1 expression in CTCs was not significantly correlated with OS (pre-treatment: HR = 0.73, 95% CI 0.44–1.21, P > 0.05; post-treatment: HR = 0.83, 95% CI 0.35–1.98, P > 0.05; Table 2, Fig. 5a–b) or PFS (pre-treatment: HR = 0.75, 95% CI 0.52–1.08, P > 0.05; post-treatment: HR = 0.95, 95% CI 0.50–1.80, P > 0.05; Table 2, Fig. 5a–b). Stratified analysis of sample size and region revealed that PD-L1+CTCs were associated with superior OS when the sample size was ≤ 30 (HR = 0.43, 95% CI 0.19–0.97, P < 0.05; Table 2).

Subgroup analysis of PD-L1 expression in CTCs versus OS/ PFS after different treatment durations
Correlation between exoPD-L1 and prognosis in patients with NSCLC undergoing ICI therapy
Two studies demonstrated the relationship between exoPD-L1 and prognosis in patients with NSCLC undergoing ICI therapy. Of these, one reported the correlation of exoPD-L1 with both OS and PFS, while another involved the correlation with only PFS. As shown in Fig. 6a, two studies involving 170 patients with NSCLC receiving ICI therapy investigated the association between exoPD-L1 and PFS. The overall pooled results showed that exoPD-L1 was not significantly correlated with PFS (HR = 0.97, 95% CI 0.28–3.37, P = 0.96), and there was a high level of heterogeneity (I2 = 94.2%, P = 0.000). The relationship between the post-treatment dynamic upregulation of exoPD-L1 and OS in patients with NSCLC undergoing ICI therapy was reported only by Yang et al. In particular, the fold-increasing changes of exoPD-L1 were significantly associated with longer OS (HR = 0.20, 95% CI 0.07–0.53, P < 0.001).

Forest plots of the correlation between exoPD-L1 and PFS in patients undergoing ICI therapy. a: exoPD-L1 expression versus PFS; Wang (2022a) represented the pre-treatment data with mono-immunotherapy; Wang (2022b) represented the pre-treatment data with combination immunotherapy; Wang (2022c) represented the upregulation in the post-treatment data with mono-immunotherapy; Wang (2022d) represented the upregulation in the post-treatment data with combination immunotherapy. b: Subgroup analysis of exoPD-L1 (pre-treatment and post-treatment dynamic changes) and PFS after different treatment durations
As studies on the correlation of pre-treatment exoPD-L1 with OS were not retrieved, subgroup analysis was performed with data on exoPD-L1 and PFS after different treatment durations. The results of the subgroup analysis revealed that the difference in treatment duration was the source of heterogeneity. The heterogeneity decreased to 0% in both the pre-treatment and post-treatment subgroups (Fig. 6b). High pre-treatment exoPD-L1 levels were significantly associated with unfavorable PFS (HR = 4.44, 95% CI 2.87–6.89, P < 0.001; Fig. 6b). However, post-treatment dynamic exoPD-L1 upregulation was significantly correlated with favorable PFS (HR = 0.36, 95% CI 0.24–0.54, P < 0.001; Fig. 6b).
Correlation between clinicopathological parameters and prognosis in patients with NSCLC undergoing ICI therapy
Five studies [23, 27, 28, 31, 33] involving 511 patients with NSCLC undergoing ICI therapy investigated the association between PFS or OS and clinicopathologic features. In this meta-analysis, six indicators of gender, age, Eastern Cooperative Oncology Group Performance Status (ECOG PS), smoking status, metastatic status, and the expression of tPD-L1 were analyzed in association with PFS or OS. The pooled results indicated that these six indicators do not significantly correlate with PFS and OS in patients with NSCLC (the results are listed in Table S1).
Publication bias
The Begg's and Egger's tests were performed to examine publication bias. Publication bias was not observed in the three markers (P > 0.05) (the P values are listed in Table S2). The plots of Begg's and Egger's test results are shown in Fig. S1.
Discussion
Cancers hide from the immune system through PD-L1 upregulation, which is associated with a poor prognosis [39]. Additionally, the activation of the PD-1/PD-L1 pathway can lead to a series of alterations in the T-cell response, including an enhanced threshold of activated T-cells, reducing their proliferation and promoting their exhaustion and apoptosis [40]. This weakens the anti-cancer immune response, allowing tumors to acquire immune escape capacity. PD-1/PD-L1 pathway inhibitors block the communication between PD-1 and PD-L1, improving the survival of patients with cancer by restoring the immune response against tumor cells [41, 42]. However, the clinical efficacy of ICIs is unsatisfactory, with some patients exhibiting hyper-progression, leading to fatality. Recently, PD-L1 has been widely studied as a promising tumor marker. The tPD-L1 expression level is considered a predictive biomarker for the efficacy of ICIs [43]. However, in patients with advanced NSCLC, performing reproducible detection is challenging as the tumor tissues are difficult to obtain. The emergence of precision medicine has enabled the analysis of molecular biomarkers based on liquid biopsies owing to their portability and reproducibility, which can overcome the spatial and temporal heterogeneity of malignancies. However, the predictive and prognostic values of blood-based PD-L1 indicators in patients with NSCLC undergoing ICI therapy are unclear, warranting a systematic meta-analysis. This is the first systematic and comprehensive analysis of the pre-treatment and post-treatment dynamic changes in the three blood-based PD-L1 biomarkers in patients with NSCLC undergoing ICI therapy. Although some studies have performed meta-analyses of sPD-L1 and PD-L1 in CTCs, they collectively analyzed various tumors [44, 45]. These studies did not individually analyze patients with NSCLC, especially the dynamic changes before and after the application of ICIs. In terms of exoPD-L1, an analogous meta-analysis of exoPD-L1 has not been previously performed. The evaluation of dynamic PD-L1 levels before and after treatment is essential for patients with cancer undergoing ICI therapy. Therefore, it is particularly vital that the levels of blood-based PD-L1 are evaluated at different time points. The strength of this study is that subgroup analyses of the included studies were performed before and after immunotherapy. Meanwhile, the correlation between each marker and prognosis at different treatment times was elucidated.
A review of the literature identified 14 trials with 928 NSCLC cases. In this meta-analysis, seven studies on sPD-L1 involving 554 patients with NSCLC, six studies on PD-L1 in CTCs involving 247 patients with NSCLC, and two studies on exoPD-L1 involving 171 patients with NSCLC were included to investigate the prognostic effect of these blood markers in patients with NSCLC undergoing ICI therapy.
The analysis revealed that high levels of sPD-L1 were significantly correlated with worse OS (HR = 2.11, 95% CI 1.59–2.80, P < 0.001) and PFS (HR = 2.14, 95% CI 1.59–2.88, P < 0.001). The subgroup analysis results revealed that high pre-treatment levels of sPD-L1 were significantly associated with poorer OS (HR = 2.32, 95% CI 1.68–3.18, P < 0.001) and PFS (HR = 2.52, 95% CI 1.72–3.68, P < 0.001). However, after immunotherapy, the upregulation of sPD-L1 was not significantly correlated with OS (HR = 1.46, 95% CI = 0.65–3.26, P > 0.05) or PFS (HR = 1.62, 95% CI = 0.92–2.86, P > 0.05). This result suggests that high pre-treatment levels of sPD-L1 can be considered a biomarker to predict the prognosis of NSCLC patients receiving ICIs. These findings are consistent with those of Han et al., who reported that lower pre-treatment sPD-L1 levels predicted improved PFS and OS [46]. Additionally, another study demonstrated that high baseline levels of sPD-L1 were associated with poor OS in patients who initially received immunotherapy [47]. sPD-L1, a predictor of tumor proliferation, migration, and survival, is reported to be a potential predictive and prognostic biomarker for immunotherapy [48]. However, the dynamic changes in post-treatment sPD-L1 were not associated with prognosis. This meta-analysis included three studies related to post-treatment. Costantini et al. demonstrated that high sPD-L1 levels in NSCLC patients receiving nivolumab were associated with adverse effects and a poorer prognosis [31]. However, Tiako Meyo et al. demonstrated that the upregulated sPD-L1 levels were not significantly associated with PFS and OS in patients treated with nivolumab. Interesting, the authors proposed a composite biomarker, namely the combination of sPD-1 and sPD-L1, to predict the efficacy and prognosis of nivolumab in patients with NSCLC [28]. This provides new insights for future studies. Yang et al. suggested that the dynamic changes of sPD-L1 were not correlated with treatment efficacy and OS but were significantly linked to PD-L1 mRNA and exoPD-L1 levels [26].
Recently, several studies have proposed that high expression of PD-L1 in CTCs is associated with a poorer prognosis in patients with various cancers treated with other therapies, such as chemotherapy or surgery [22, 49, 50]. In contrast, PD-L1 upregulation in CTCs predicts a favorable prognosis in patients with cancer undergoing ICIs [51, 52]. However, the pooled results of this analysis indicated no significant correlation between PD-L1+ CTCs and OS (HR = 0.75, 95% CI 0.49–1.13, P = 0.170) or PFS (HR = 0.79, 95% CI 0.59–1.06, P = 0.12). Furthermore, pre-treatment and post-treatment subgroup analyses did not reveal significant differences. These results suggest that PD-L1+ CTCs may not be correlated with the prognosis of patients with NSCLC undergoing ICI therapy. Of the six included studies, three were pre-immunotherapy studies. Guibert et al. demonstrated that the PD-L1+ CTCs before immunotherapy were not significantly correlated with prognosis, but this correlation was significant in patients with treatment failure and disease progression [25]. Dhar et al. reported no significant correlation between PD-L1+ CTCs before immunotherapy and PFS [35]. This can be attributed to the decreased number of patients included in the study (n = 17). However, Zhang et al. demonstrated that pre-treatment PD-L1+ CTCs were positively correlated with PFS and OS in patients with NSCLC treated with immunotherapy plus chemotherapy [38]. The results of these two studies were contrasting. We consider that the heterogeneity may be attributable to two factors. First, the treatment protocols were different in the two studies. Guibert et al. utilized nivolumab, whereas Zhang et al. used sintilimab plus docetaxel. Second, the cut-off values of the two studies were markedly different (Table 1). Three studies examined dynamic changes after immunotherapy. Dall'Olio et al. and Ikeda et al. revealed that, compared to patients with negative PD-L1 expression in CTCs, PD-L1+ CTCs have significantly longer PFS after immunotherapy [27, 37]. However, Zhang et al. demonstrated that PD-L1 expression in CTCs was not associated with PFS [36].
In this meta-analysis, only two studies related to exoPD-L1 were included. The pooled results showed that elevated pre-treatment exoPD-L1 levels were significantly linked to poorer PFS (HR = 4.44, 95% CI 2.87–6.89, P < 0.001; Fig. 4b). However, the dynamic increases in post-treatment exoPD-L1 were associated with superior PFS (HR = 0.36, 95% CI 0.24–0.54, P < 0.001) and OS (HR = 0.20, 95% CI 0.07–0.53, P < 0.001). In conclusion, the role of exoPD-L1 in determining the prognosis was reversed with the increase in treatment duration. Similarly, one study on solid tumors treated with anti-PD-1 therapy reported that the high pre-treatment exoPD-L1 levels predicted a short PFS [53]. Exosomes belong to one of the subgroups of extracellular vesicles (EVs). EVs, which are lipid-bound vesicles secreted by cells into the extracellular space, comprise the following three primary subtypes: microvesicles (MVs), exosomes, and apoptotic bodies. These subtypes can be differentiated based on their release pathways, dimensions, contents, and functions [54,55,56]. Tumor cells can utilize EVs to evade immune responses and promote cancer progression and metastasis [57]. Additionally, tumor cells can secrete a large amount of PD-L1 through EVs. ExoPD-L1 binds to PD-1 through its extracellular domain, and the removal of exoPD-L1 can inhibit tumor growth [58]. Chen et al. found that exoPD-L1 can interact with activated T-cells [59]. Circulating exoPD-L1 was closely associated with cancer progression and immune suppression in patients with cancer. This is consistent with the findings of some reviews [60]. However, elevated exoPD-L1 levels after several treatment cycles predicted a good prognosis in patients with NSCLC. Similarly, some studies found that the higher the level of exoPD-L1 increased after applying PD-1 antibodies, the longer the prognosis of cancer patients [24, 26, 59]. Several studies have also confirmed an increase in tPD-L1 expression in the early stages of treatment in patients who respond to ICIs [61]. During the early stages of immunotherapy, PD-L1 expression in tissues and exoPD-L1 in circulation may be upregulated. This is because immunotherapy blocks the interaction between PD-1 and PD-L1, leading to the release of most PD-L1 through exosomes. Therefore, increased PD-L1 expression after immunotherapy may exert a positive immune regulatory effect. However, de Miguel-Perez et al. found that the dynamic increase of EV PD-L1 in the blood of patients with NSCLC was strongly associated with treatment failure and decreased survival [62]. This finding is in contrast to that of this study. The reason for the heterogeneity can be attributed to two factors. First, Yang et al. and Wang et al. detected exoPD-L1 using the Simoa platform and enzyme-linked immunosorbent assay, respectively. However, de Miguel-Perez et al. used the immunoblotting method for the detection of EV PD-L1. Second, two studies included in this meta-analysis analyzed PD-L1 in the exosomes, whereas de Miguel-Perez et al. analyzed PD-L1 in EV. Recent studies have confirmed that PD-L1 can be detected in both exosomes and MVs [59, 63]. Exosomes are only one subtype of EVs, and the effect of MVs on the prognosis has not been previously reported. In addition, Del Re et al. evaluated the relationship between PD-L1 mRNA in plasma-derived exosomes and the efficacy of ICIs in patients with NSCLC. The results showed that the upregulation of exosomal PD-L1 mRNA was significantly and negatively associated with treatment efficacy [63]. Notably, recent studies have suggested that the PD-L1 mRNA level is distinct from the protein level, owing to post-translational regulatory mechanisms [58, 64].
Limitations
This meta-analysis has several limitations. First, the number of included studies and the sample size were small. Small-sample studies may overestimate the results of efficacy and prognostic evaluations. Second, the pooled results revealed that post-treatment sPD-L1 levels and PD-L1 expression in CTCs were not correlated with the prognosis of patients with NSCLC undergoing ICI therapy. This can be attributed to the high heterogeneity among the studies. Most studies have no definite consensus on the cut-off values of biomarkers and utilize various assay platforms, which may have contributed to the high heterogeneity of these studies and biased outcomes. Therefore, a criterion threshold must be established through a uniform and standardized protocol. In the future, the correlation of PD-L1 expression in CTCs and post-treatment sPD-L1 levels with the prognosis of NSCLC patients receiving ICI therapy needs to be validated using large-sample and multi-center clinical trials. Third, only three indicators were included in the analysis. EVs and some immune cells in the blood also contain PD-L1, such as dendritic cells and myeloid-derived suppressor cells [65], which were not included in this meta-analysis. In the following work, we plan to systematically analyze all blood-based PD-L1 markers and apply more analytical tools such as bioinformatic analysis and Mendelian randomized trials to screen valuable signature genes. Fourth, most of the included studies analyzed only individual markers but not multi-target or multi-gene combinations. Furthermore, these three markers were not validated in clinical trials. In the future, clinical studies combining multiple markers will be performed to validate the characteristic markers.
Conclusions
The comprehensive meta-analysis of three blood-based PD-L1 indicators suggested that pre-treatment sPD-L1 and exoPD-L1 serve as unfavorable prognostic factors in patients with NSCLC undergoing ICI therapy. In contrast, the dynamic upregulation of post-treatment exoPD-L1 levels indicates a favorable prognosis. However, post-treatment sPD-L1 levels and PD-L1 expression in CTCs were not correlated with the prognosis of patients with NSCLC undergoing ICI therapy. The blood-based PD-L1 analysis can provide clinicians with a convenient biomarker and complement tPD-L1 analysis to improve the clinical application of ICIs. It is also a potential strategy for predicting treatment efficacy and prognosis in patients with cancer.
Availability of data and materials
The data analyzed during the current study are available from the corresponding author.
Abbreviations
- NSCLC:
-
Non-small cell lung cancer
- SCLC:
-
Small cell lung cancer
- sPD-L1:
-
Soluble PD-L1
- exoPD-L1:
-
Exosomal PD-L1
- HR:
-
Hazard ratio
- CI:
-
Confidence interval
- OS:
-
Overall survival
- PFS:
-
Progression-free survival
- ICIs:
-
Immune checkpoint inhibitors
- PD-1:
-
Programmed cell death protein 1
- PD-L1:
-
Programmed cell death ligand 1
- CTLA-4:
-
Cytotoxic T lymphocyte antigen 4
- NOS:
-
Newcastle-Ottawa Scale
- ECOG PS:
-
Eastern Cooperative Oncology Group Performance Status
- EVs:
-
Extracellular vesicles
- MVs:
-
Microvesicles
References
Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2021. CA Cancer J Clin. 2021;71:7–33.
Miller KD, Nogueira L, Devasia T, Mariotto AB, Yabroff KR, Jemal A, et al. Cancer treatment and survivorship statistics, 2022. CA Cancer J Clin. 2022;72:409–36.
Hamid O, Robert C, Daud A, Hodi FS, Hwu WJ, Kefford R, et al. Five-year survival outcomes for patients with advanced melanoma treated with pembrolizumab in KEYNOTE-001. Ann Oncol. 2019;30:582–8.
Marhelava K, Pilch Z, Bajor M, Graczyk-Jarzynka A, Zagozdzon R. Targeting negative and positive immune checkpoints with monoclonal antibodies in therapy of cancer. Cancers. 2019;11:1756.
Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csőszi T, Fülöp A, et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med. 2016;375:1823–33.
Paz-Ares L, Ciuleanu TE, Cobo M, Schenker M, Zurawski B, Menezes J, et al. First-line nivolumab plus ipilimumab combined with two cycles of chemotherapy in patients with non-small-cell lung cancer (CheckMate 9LA): an international, randomised, open-label, phase 3 trial. Lancet Oncol. 2021;22:198–211.
Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer. 2012;12:252–64.
Garon EB, Rizvi NA, Hui R, Leighl N, Balmanoukian AS, Eder JP, et al. Pembrolizumab for the treatment of non-small-cell lung cancer. N Engl J Med. 2015;372:2018–28.
Wei SC, Duffy CR, Allison JP. Fundamental Mechanisms of Immune Checkpoint Blockade Therapy. Cancer Discov. 2018;8:1069–86.
Liu W, Zhang Q, Zhang T, Li L, Xu C. Quality of life in patients with non-small cell lung cancer treated with PD-1/PD-L1 inhibitors: a systematic review and meta-analysis. World J Surg Oncol. 2022;20:333.
Chen Y, Wen S, **a J, Du X, Wu Y, Pan B, et al. Association of Dynamic Changes in Peripheral Blood Indexes with Response to PD-1 Inhibitor-Based Combination Therapy and Survival Among Patients with Advanced Non-Small Cell Lung Cancer. Front Immunol. 2021;12:672271.
Sunshine J, Taube JM. PD-1/PD-L1 inhibitors. Curr Opin Pharmacol. 2015;23:32–8.
Sunshine JC, Nguyen PL, Kaunitz GJ, Cottrell TR, Berry S, Esandrio J, et al. PD-L1 Expression in melanoma: a quantitative immunohistochemical antibody comparison. Clin Cancer Res. 2017;23:4938–44.
Rittmeyer A, Barlesi F, Waterkamp D, Park K, Ciardiello F, von Pawel J, et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a phase 3, open-label, multicentre randomised controlled trial. Lancet. 2017;389:255–65.
Wang C, Qiao W, Jiang Y, Zhu M, Shao J, Wang T, et al. The landscape of immune checkpoint inhibitor plus chemotherapy versus immunotherapy for advanced non-small-cell lung cancer: a systematic review and meta-analysis. J Cell Physiol. 2020;235:4913–27.
Zaretsky JM, Garcia-Diaz A, Shin DS, Escuin-Ordinas H, Hugo W, Hu-Lieskovan S, et al. Mutations associated with acquired resistance to PD-1 blockade in melanoma. N Engl J Med. 2016;375:819–29.
Micevic G, Theodosakis N, Bosenberg M. Aberrant DNA methylation in melanoma: biomarker and therapeutic opportunities. Clin Epigenet. 2017;9:34.
Woo D, Yu M. Circulating tumor cells as “liquid biopsies” to understand cancer metastasis. Transl Res. 2018;201:128–35.
Chen X, Du Z, Huang M, Wang D, Fong WP, Liang J, et al. Circulating PD-L1 is associated with T cell infiltration and predicts prognosis in patients with CRLM following hepatic resection. Cancer Immunol Immunother. 2022;71:661–74.
Vecchiarelli S, Passiglia F, D’Incecco A, Gallo M, De Luca A, Rossi E, et al. Circulating programmed death ligand-1 (cPD-L1) in non-small-cell lung cancer (NSCLC). Oncotarget. 2018;9:17554–63.
Li JW, Wei P, Guo Y, Shi D, Yu BH, Su YF, et al. Clinical significance of circulating exosomal PD-L1 and soluble PD-L1 in extranodal NK/T-cell lymphoma, nasal-type. Am J Cancer Res. 2020;10:4498–512.
Bergmann S, Coym A, Ott L, Soave A, Rink M, Janning M, et al. Evaluation of PD-L1 expression on circulating tumor cells (CTCs) in patients with advanced urothelial carcinoma (UC). Oncoimmunology. 2020;9:1738798.
Mazzaschi G, Minari R, Zecca A, Cavazzoni A, Ferri V, Mori C, et al. Soluble PD-L1 and circulating CD8+PD-1+ and NK cells enclose a prognostic and predictive immune effector score in immunotherapy treated NSCLC patients. Lung Cancer. 2020;148:1–11.
Wang Y, Niu X, Cheng Y, Zhang Y, **a L, **a W, et al. Exosomal PD-L1 predicts response with immunotherapy in NSCLC patients. Clin Exp Immunol. 2022;208:316–22.
Guibert N, Delaunay M, Lusque A, Boubekeur N, Rouquette I, Clermont E, et al. PD-L1 expression in circulating tumor cells of advanced non-small cell lung cancer patients treated with nivolumab. Lung Cancer. 2018;120:108–12.
Yang Q, Chen M, Gu J, Niu K, Zhao X, Zheng L, et al. Novel biomarkers of dynamic blood PD-L1 expression for immune checkpoint inhibitors in advanced non-small-cell lung cancer patients. Front Immunol. 2021;12:665133.
Dall’Olio FG, Gelsomino F, Conci N, Marcolin L, De Giglio A, Grilli G, et al. PD-L1 expression in circulating tumor cells as a promising prognostic biomarker in advanced non–small-cell lung cancer treated with immune checkpoint inhibitors. Clin Lung Cancer. 2021;22:423–31.
Tiako Meyo M, Jouinot A, Giroux-Leprieur E, Fabre E, Wislez M, Alifano M, et al. Predictive value of soluble PD-1, PD-L1, VEGFA, CD40 ligand and CD44 for nivolumab therapy in advanced non-small cell lung cancer: a case-control study. Cancers. 2020;12:473.
Jiang T, Bai Y, Zhou F, Li W, Gao G, Su C, et al. Clinical value of neutrophil-to-lymphocyte ratio in patients with non-small-cell lung cancer treated with PD-1/PD-L1 inhibitors. Lung Cancer. 2019;130:76–83.
Al-Showbaki L, Wilson B, Tamimi F, Molto C, Mittal A, Cescon DW, et al. Changes in circulating tumor DNA and outcomes in solid tumors treated with immune checkpoint inhibitors: a systematic review. J Immunother Cancer. 2023;11:e005854.
Costantini A, Julie C, Dumenil C, Hélias-Rodzewicz Z, Tisserand J, Dumoulin J, et al. Predictive role of plasmatic biomarkers in advanced non-small cell lung cancer treated by nivolumab. Oncoimmunology. 2018;7:e1452581.
Okuma Y, Wakui H, Utsumi H, Sagawa Y, Hosomi Y, Kuwano K, et al. Soluble programmed cell death ligand-1 (sPD-L1) as a novel biomarker for nivolumab therapy for non-small cell lung cancer. Clin Lung Cancer. 2018;19:410–7.
Murakami S, Shibaki R, Matsumoto Y, Yoshida T, Goto Y, Kanda S, et al. Association between serum level soluble programmed cell death ligand 1 and prognosis in patients with non-small cell lung cancer treated with anti-PD-1 antibody. Thorac Cancer. 2020;11:3585–95.
Zizzari IG, Di Filippo A, Scirocchi F, Di Pietro FR, Rahimi H, Ugolini A, et al. Soluble immune checkpoints, gut metabolites and performance status as parameters of response to nivolumab treatment in NSCLC patients. J Pers Med. 2020;10:208.
Dhar M, Wong J, Che J, Matsumoto M, Grogan T, Elashoff D, et al. Evaluation of PD-L1 expression on vortex-isolated circulating tumor cells in metastatic lung cancer. Sci Rep. 2018;8:2592.
Zhang L, Zhang X, Liu Y, Zhang T, Wang Z, Gu M, et al. PD-L1+ aneuploid circulating tumor endothelial cells exhibit resistance to the checkpoint blockade immunotherapy in advanced NSCLC patients. Cancer Lett. 2020;469:355–66.
Ikeda M, Koh Y, Teraoka S, Sato K, Oyanagi J, Hayata A, et al. Longitudinal evaluation of PD-L1 expression on circulating tumor cells in non-small cell lung cancer patients treated with nivolumab. Cancers. 2021;13:2290.
Zhang Y, Song L, Zeng L, **ong Y, Liu L, Zhou C, et al. Sintilimab plus docetaxel as second-line therapy of advanced non-small cell lung cancer without targetable mutations: a phase II efcacy and biomarker study. BMC Cancer. 2022;22:952.
Kythreotou A, Siddique A, Mauri FA, Bower M, Pinato DJ. PD-L1. J Clin Pathol. 2018;71:189–94.
Frydenlund N, Mahalingam M. PD-L1 and immune escape: insights from melanoma and other lineage-unrelated malignancies. Hum Pathol. 2017;66:13–33.
Brahmer J, Reckamp KL, Baas P, Crinò L, Eberhardt WE, Poddubskaya E, et al. Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N Engl J Med. 2015;373:123–35.
Gandhi L, Rodríguez-Abreu D, Gadgeel S, Esteban E, Felip E, De Angelis F, et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N Engl J Med. 2018;378:2078–92.
Hirsch FR, McElhinny A, Stanforth D, Ranger-Moore J, Jansson M, Kulangara K, et al. PD-L1 Immunohistochemistry assays for lung cancer: results from phase 1 of the blueprint PD-L1 IHC assay comparison project. J Thorac Oncol. 2017;12:208–22.
Li X, Zheng Y, Yue F. Prognostic value of Soluble Programmed Cell Death Ligand-1 (sPD-L1) in various cancers: a meta-analysis. Target Oncol. 2021;16:13–26.
Kong D, Zhang W, Yang Z, Li G, Cheng S, Zhang K, et al. Correlation between PD-L1 expression on CTCs and prognosis of patients with cancer: a systematic review and meta-analysis. Oncoimmunology. 2021;10:1938476.
Han X, Gu YK, Li SL, Chen H, Chen MS, Cai QQ, et al. Pre-treatment serum levels of soluble programmed cell death-ligand 1 predict prognosis in patients with hepatitis B-related hepatocellular carcinoma. J Cancer Res Clin Oncol. 2019;145:303–12.
Genova C, Tasso R, Rosa A, Rossi G, Reverberi D, Fontana V, et al. Prognostic role of soluble and extracellular vesicle-associated PD-L1, B7–H3 and B7–H4 in non-small cell lung cancer patients treated with immune checkpoint inhibitors. Cells. 2023;12:832.
Mildner F, Sopper S, Amann A, Pircher A, Pall G, Köck S, et al. Systematic review: Soluble immunological biomarkers in advanced nonsmall-cell lung cancer (NSCLC). Crit Rev Oncol Hematol. 2020;153:102948.
Pinato DJ, Vallipuram A, Evans JS, Wong C, Zhang H, Brown M, et al. Programmed cell death ligand expression drives immune tolerogenesis across the diverse subtypes of neuroendocrine tumours. Neuroendocrinology. 2021;111:465–74.
Satelli A, Mitra A, Brownlee Z, **a X, Bellister S, Overman MJ, et al. Epithelial-mesenchymal transitioned circulating tumor cells capture for detecting tumor progression. Clin Cancer Res. 2015;21:899–906.
Yue C, Jiang Y, Li P, Wang Y, Xue J, Li N, et al. Dynamic change of PD-L1 expression on circulating tumor cells in advanced solid tumor patients undergoing PD-1 blockade therapy. Oncoimmunology. 2018;7:e1438111.
Tan Z, Yue C, Ji S, Zhao C, Jia R, Zhang Y, et al. Assessment of PD-L1 expression on circulating tumor cells for predicting clinical outcomes in patients with cancer receiving PD-1/PD-L1 blockade therapies. Oncologist. 2021;26:e2227–38.
Zhang C, Fan Y, Che X, Zhang M, Li Z, Li C, et al. Anti-PD-1 Therapy response predicted by the combination of exosomal PD-L1 and CD28. Front Oncol. 2020;10:760.
Zaborowski MP, Balaj L, Breakefield XO, Lai CP. Extracellular vesicles: composition, biological relevance, and methods of study. Bioscience. 2015;65:783–97.
Yáñez-Mó M, Siljander PR, Andreu Z, Zavec AB, Borràs FE, Buzas EI, et al. Biological properties of extracellular vesicles and their physiological functions. J Extracell Vesicles. 2015;4:27066.
Borges FT, Reis LA, Schor N. Extracellular vesicles: Structure, function, and potential clinical uses in renal diseases. Braz J Med Biol Res. 2013;46:824–30.
Chen DS, Mellman I. Elements of cancer immunity and the cancer–immune set point. Nature. 2017;541:321–30.
Poggio M, Hu T, Pai CC, Chu B, Belair CD, Chang A, et al. Suppression of exosomal PD-L1 induces systemic anti-tumor immunity and memory. Cell. 2019;177:414–27.
Chen G, Huang AC, Zhang W, Zhang G, Wu M, Xu W, et al. Exosomal PD-L1 contributes to Immunosuppression and is associated with anti-PD-1 Response. Nature. 2018;560:382–6.
**e F, Xu M, Lu J, Mao L, Wang S. The role of exosomal PD-L1 in tumor progression and immunotherapy. Mol Cancer. 2019;18:146.
Vilain RE, Menzies AM, Wilmott JS, Kakavand H, Madore J, Guminski A, et al. Dynamic changes in PD-L1 expression and immune infiltrates early during treatment predict response to PD-1 blockade in melanoma. Clin Cancer Res. 2017;23:5024–33.
de Miguel-Perez D, Russo A, Arrieta O, Ak M, Barron F, Gunasekaran M, et al. Extracellular vesicle PD-L1 dynamics predict durable response to immune-checkpoint inhibitors and survival in patients with non-small cell lung cancer. J Exp Clin Cancer Res. 2022;41:186.
Del Re M, Marconcini R, Pasquini G, Rofi E, Vivaldi C, Bloise F, et al. PD-L1 mRNA expression in plasma-derived exosomes is associated with response to anti-PD-1 antibodies in melanoma and NSCLC. Br J Cancer. 2018;118:820–4.
Zerdes I, Matikas A, Bergh J, Rassidakis GZ, Foukakis T. Genetic, transcriptional and post-translational regulation of the programmed death protein ligand 1 in cancer: biology and clinical correlations. Oncogene. 2018;37:4639–61.
Wang T, Denman D, Bacot SM, Feldman GM. Challenges and the evolving landscape of assessing blood-based PD-L1 expression as a biomarker for anti-PD-(L)1 immunotherapy. Biomedicines. 2022;10:1181.
Acknowledgements
Thanks very much to AQing Liu, Ying **a, Guan Zhang and Yanjie Yang for providing some suggestions in revising the paper.
Funding
This work was supported by the Scientific Research Plan Project of Tian** Education Commission (No. 2018KJ034).
Author information
Authors and Affiliations
Contributions
Q.C. designed and drafted the manuscript; WT.L, D.W. and SC.W. searched articles and checked grammar; JC.Y. designed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
PRISMA Checklist.
Additional file 2.
Full search strategies.
Additional file 3:
Table S1. Correlation of OS/PFS and clinicopathological characteristic of NSCLC patients. Table S2. Results of Begg's and Egger's tests of 3 indicators related to PFS/OS. Fig.S1. Results of Begg's and Egger's tests of 3 indicators related to PFS/OS a, Beeg’s and Egger’s between sPD-L1 and OS; b, Beeg’s and Egger’s between sPD-L1 and PFS; c, Beeg’s and Egger’s between PD-L1 in CTCs and OS; d, Beeg’s and Egger’s between PD-L1 in CTCs and PFS; e, Beeg’s and Egger’s between exoPD-L1 score and PFS.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Cui, Q., Li, W., Wang, D. et al. Prognostic significance of blood-based PD-L1 analysis in patients with non-small cell lung cancer undergoing immune checkpoint inhibitor therapy: a systematic review and meta-analysis. World J Surg Onc 21, 318 (2023). https://doi.org/10.1186/s12957-023-03215-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12957-023-03215-2