
Abstract
Background
Indonesia implemented one of the world’s largest single-payer national health insurance schemes (the Jaminan Kesehatan Nasional or JKN) in 2014. This study aims to assess the incidence of catastrophic health spending (CHS) and its determinants and trends between 2018 and 2019 by which time JKN enrolment coverage exceeded 80%.
Methods
This study analysed data collected from a two-round cross-sectional household survey conducted in ten provinces of Indonesia in February–April 2018 and August–October 2019. The incidence of CHS was defined as the proportion of households with out-of-pocket (OOP) health spending exceeding 10% of household consumption expenditure. Chi-squared tests were used to compare the incidences of CHS across subgroups for each household characteristic. Logistic regression models were used to investigate factors associated with incurring CHS and the trend over time. Sensitivity analyses assessing the incidence of CHS based on a higher threshold of 25% of total household expenditure were conducted.
Results
The overall incidence of CHS at the 10% threshold fell from 7.9% to 2018 to 4.4% in 2019. The logistic regression models showed that households with JKN membership experienced significantly lower incidence of CHS compared to households without insurance coverage in both years. The poorest households were more likely to incur CHS compared to households in other wealth quintiles. Other predictors of incurring CHS included living in rural areas and visiting private health facilities.
Conclusions
This study demonstrated that the overall incidence of CHS decreased in Indonesia between 2018 and 2019. OOP payments for health care and the risk of CHS still loom high among JKN members and among the lowest income households. More needs to be done to further contain OOP payments and further research is needed to investigate whether CHS pushes households below the poverty line.
Similar content being viewed by others

Background
Achieving universal health coverage (UHC) is one of the overarching targets of the 2030 sustainable development goals (SDGs) [1]. In addition to improved access to health services, financial risk protection is another UHC goal, which is defined as access to all needed quality health services without financial hardship [2]. In September 2019, the United Nations (UN) General Assembly held a high-level meeting, where all UN Member States reaffirmed their commitment to UHC [3]. Despite this commitment, the burden imposed by out-of-pocket (OOP) health payments still results in financial hardship for millions of people who seek health care globally [4]. It is estimated that globally approximately 70 million people were pushed into extreme poverty and a further 435 million people were pushed deeper into extreme poverty in 2017 by OOP health payments [5]. While OOP payments have been steadily declining in Indonesia over the past 10 years, National Health Accounts (NHA) data show that in 2020, OOP payments accounted for around one-third of total current health expenditure [6]. This rate was higher than that of Singapore (29%), Thailand (10%) and Brunei Darussalam (5%) [7].
The level of financial protection is measured by catastrophic health spending (CHS) which is defined under SDG indicator 3.8.2 as OOP health payments greater than 10% or 25% of total household expenditure [1]. Studies have found that CHS reduces the consumption of essential commodities such as food, housing, and education of children [8], pushing many families into poverty [9]. In 2017, Wagstaff et al. demonstrated that the global incidence of CHS at the 10% threshold (the most commonly used threshold for global monitoring of CHS) had increased from 9.7% to 2000, to 11.4% in 2005, and to 11.7% in 2010 [10]. Wagstaff et al. also reported that the expansion of health insurance coverage in Indonesia did not coincide with a reduction in the incidence of CHS between 2000 and 2010 [10]. A more recent study by the World Health Organization (WHO) and the World Bank showed that the incidence of CHS in Indonesia had worsened over time, rising from 3.6% to 2015 to 4.5% in 2017 at the 10% threshold [5, 11].
In 2014, the Government of Indonesia introduced its national health insurance program Jaminan Kesehatan Nasional (JKN) managed by the Social Security Organizing Agency for Health (Badan Penyelenggara Jaminan Kesehatan-BPJS Kesehatan) in order to provide universal access to health services with a focus on targeting and subsidizing care for the poor. The JKN mandates all wage earners (formal sector employees) to contribute 1% of their payroll to the JKN with employers required to provide matching funding of an additional 4% of their employees’ wages. The poorest 40% of the population (who are deemed incapable of contributing) are fully subsidized by the central, provincial, city or district governments. Non-wage earners pay a fixed contribution, at three different levels, Indonesian Rupiah (IDR) 42,000, 100,000 and 150,000 per person per month, based on the choice of ward class selected by the person [12]. The JKN covers comprehensive medical care defined as medically necessary health care. Public and private primary health care providers are paid under a capitation model, while public and private hospitals are paid using the Indonesian Case Base Groups (INA-CBG) for all outpatient and inpatient care [13]. In theory, when a JKN member attends a facility within the JKN network, no co-payment or cost-sharing is required. By December 2022, the JKN Administrator reported covering 90% of the Indonesian population [14].
Although the WHO and the World Bank regularly publish data on the incidence of CHS globally, including for Indonesia [5, 15], they have used national socioeconomic survey data that were not originally designed for measuring CHS and consequently do not capture all major aspects of OOP spending on health care in Indonesia. Moreover, the incidence of CHS from 2018 onward has not been published. This study is a retrospective data analysis of a two-round household survey that collected comprehensive information on OOP health spending in Indonesia between 2018 and 2019. The aim of this study was to assess the incidence, determinants, and trend of CHS in the JKN era between 2018 and 2019 by which time JKN enrolment coverage exceeded 80%. This updated evidence will help the Indonesian government design policy reforms to address current gaps in financial protection.
Methods
Study setting
Indonesia is the largest economy in Southeast Asia, and a member of the Group of Twenty (G20), a group of finance ministers and central bank governors from 19 of the world’s largest economies and the European Union. Due to the economic impact of the pandemic, Indonesia went from upper-middle income to lower-middle income status in July 2021, but regained upper middle-income country status in 2023. It is the world’s largest archipelago and the fourth most populous country in the world with approximately 270 million inhabitants. In recent decades, Indonesia has made significant progress in health outcomes, but several challenges remain, particularly in maternal health, nutrition, communicable diseases such as tuberculosis, and an increasing health burden from non-communicable diseases [16]. Indonesia spends relatively little on health (3% of GDP, 2020), compared to the average of upper middle-income countries (7% of GDP, 2020) [7]. Approximately 57% of all health expenditure is from the government, with one-third from household OOP payments [6, 17].
Data collection
This research was part of the “Equity and Health Care Financing in Indonesia” (ENHANCE) Study [18]. The over-arching goal of ENHANCE is to assess the progress being made by Indonesia towards UHC and the impact of major reforms such as the JKN on financial protection. A detailed description of the study aims and methods can be found in the published protocol [18]. The ENHANCE study administrated two-round household survey in 10 of the 34 provinces in Indonesia. These 10 provinces accounted for about 74% of the Indonesian population and allowed a comprehensive assessment of the impact of the JKN on households’ health spending. The first wave of data collection occurred in February – April 2018, and the second wave was carried out in August – October 2019. The selection of provinces was done purposively to capture Indonesia’s different socioeconomic conditions and demographic characteristics. The key considerations for selecting provinces were population size and location. The selection of districts within provinces was based on the geographic location (rural/urban) and fiscal capacity index (FCI) as defined by the Indonesian Ministry of Finance, [19].
This index is published every year and compares regional governments in terms of their capacity to finance a minimum standard of services. The index is used for the distribution of the national budget to regional (both Provincial and District) governments to promote equity (i.e. providing a greater central budget allocation to provinces with lower fiscal capacity ) [19]. In the study provinces, households were selected using a systematic random sampling procedure without any exclusion criteria. First, three districts were selected from each of the ten sample provinces and then classified as having either high, moderate, or low fiscal capacity based on the Regional Fiscal Capacity Map [19]. In each selected district, two sub-districts and four villages (two villages per sub-district) were randomly sampled using a list of sub-districts and villages as the sampling frame. Finally, in each village, we selected neighbourhoods from which households were proportionally selected. Overall, 7,554 households were surveyed in the first wave (2018), but not all could be traced in the second wave, leading to 6,445 households (85% of the first wave) being re-interviewed in 2019. Full details of the sampling procedure and data collection techniques are published elsewhere [18]. In this study, we analysed data from the 6,445 households that completed both rounds of survey (85% of the total number of households interviewed in the first wave).
Data variables
We collected information on socioeconomic status, health insurance coverage, health care utilization and OOP health expenditures for each health service used. There were two types of health insurance coverage: public (JKN) and private health insurance. The health care utilization data included outpatient and inpatient care. Outpatient care represented the utilization of outpatient services in the last month from primary and secondary providers for each member of the household and all associated OOP expenditure. Inpatient care represented the utilization of inpatient services over the last year and all related OOP expenditure. OOP expenditure included fees for medical consultation, laboratory tests, radiology, drugs, medical supplies, transportation, food, and unofficial payments (e.g. tips to health workers). Unofficial payments can be initiated either by patients who believe that they will receive more attention and better treatment or by employees of public health care services [20]. In the 2019 survey, a question on hospital room charges was added to the calculation of OOP payments for inpatient care. In the survey, we also collected data on household consumption expenditure in the past month such as spending on education, utilities and transportation.
Analysis
The WHO and the World Bank define CHS as household expenditure on health care greater than 10% or greater than 25% of total household consumption expenditure. In the baseline analysis, the incidence of CHS was calculated as the proportion of households with OOP spending exceeding 10% of total household consumption expenditure, which is applied by SDG indicator 3.8.2 [1]. In the sensitivity analysis, we assessed the incidence of CHS based on the higher threshold of 25% of total household expenditure. We first aggregated individual health care utilization at the household level by adding up the number of outpatient visits and inpatient days for each household member. Similarly, we summed the OOP payments of each member to derive the total OOP payments within the household. OOP payments for outpatient care in the last month were multiplied by twelve to derive annual OOP payments. Total household consumption expenditure included eight common items: food and non-food expenditure (schooling, electricity, water, transportation, fuel, health care, social events). Annual household consumption expenditure was calculated by multiplying monthly expenditure by twelve. Sensitivity analysis excluding data on hospital room charges from OOP payments collected only in 2019 was conducted. Chi-squared tests were used to compare the incidences of CHS across subgroups for each household characteristic.
We then used logistic regression models to assess factors associated with incurring CHS in each wave. The dependent variable was whether the household experienced CHS (yes or no). The independent variables included: residence type (urban vs. rural as reference), occupation of household head (civil servant, private employee, self-employed, vs. unemployed as reference), household expenditure quintile (the poorest as the reference vs. poorer, middle, richer, and richest), health insurance coverage (JKN, private health insurance, vs. no health insurance coverage as reference), number of children under five years of age (one or more vs. none as reference), number of adults aged 60 + years (one or more vs. none as reference), and type of health care providers for outpatient or inpatient care (private, not using care, vs. public as reference). We also conducted a pooled data analysis using data from all households in both survey rounds of survey (7,554 households in the first wave, plus 6,445 households in the second wave). Again, a logistic regression model was used to predict the likelihood of incurring CHS and study round was included as an independent variable to assess the change over time in CHS. An interaction term between survey round and health insurance coverage was included. Variability between villages was first examined but not included in the final model as the variability was not statistically significant. All analyses were performed using STATA (version 15).
Results
Baseline analysis
The descriptive statistics of the matched 6,445 households in 2018 and in 2019 are shown in Table 1. The proportion of households with JKN membership increased from 64% to 2018 to 73% in 2019 and was highest among households where the head was a civil servant (88% in 2018, 95% in 2019, Appendix Table A1). The average household expenditure was higher in all five wealth quintiles in 2019 compared to 2018. Twenty-eight percent of households had one or more children under five years of age in 2018, drop** to 25% in 2019. The proportion of households with one or more adults aged over 60 years of age increased from 31% to 2018 to 34% in 2019. More than half of all households sought outpatient care in private health facilities in both 2018 and 2019. However, the high use of public hospitals for inpatient care in 2018 changed in 2019 with utilization evenly split between public and private hospitals. Among the 6,445 households that completed both rounds of the survey, 24 individuals in the first wave and 20 individuals in the second wave reported not seeking care when they were sick because they could not afford to pay medical fees.
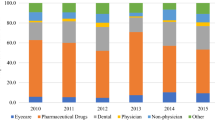
Table 2 shows the OOP payments for outpatient and inpatient care by household characteristics. The average OOP payment by households with JKN coverage decreased from IDR 268,000 in 2018 to IDR 128,000 in 2019 for outpatient care. OOP payments for inpatient care decreased from IDR 1,596,000 in 2018 to IDR 1,347,000 in 2019. Private health insurance holders, by contrast, experienced an increase in OOP payments for both outpatient and inpatient care in 2019 compared to 2018. Uninsured households incurred relatively small OOP payments for outpatient care while experiencing an increase in inpatient OOP payments. Households with higher consumption expenditure incurred much higher OOP payments compared to lower expenditure groups. As expected, households utilising private health care providers, on average, incurred more OOP costs compared to those using public health care providers. For outpatient care, most OOP costs were incurred on drugs and diagnostics (laboratory and radiology examinations). The bulk of OOP spending for inpatient care was on drugs and diagnostics.
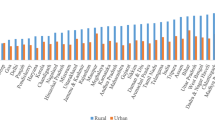
Table 3 presents the incidence of CHS at the 10% expenditure threshold in 2018 and 2019. The overall incidence of CHS is shown to have dropped from 7.9% to 2018 to 4.4% in 2019. The incidence of CHS among JKN members dropped from 7.0% to 2018 to 4.0% in 2019 and was significantly lower compared to households with private health insurance and households without insurance coverage. Households in rural areas experienced a significantly higher incidence of CHS than those in urban areas in 2018 (9.7% vs. 6.8%, P < 0.001), while the gap narrowed in 2019 (4.9% vs. 4.1%). Households where the household head was unemployed incurred an incidence of CHS at 13% in 2018, which was significantly higher than other households. In 2019, the difference was not significantly different among households with different employment statuses. The incidence of CHS was significantly higher among lowest expenditure quintiles in both years (9.7% and 5.6%). Households with one or more children under five had a significantly higher incidence of CHS compared to households with no children in both waves. The incidence of CHS was also significantly higher among households with elderly members in both years. As expected, using private health care providers was associated with a much higher incidence of CHS than seeking care from public health care providers, for both outpatient and inpatient services in both waves.
Factors associated with incurring CHS at the 10% threshold are summarised in Table 4. JKN membership was associated with a significantly lower likelihood of incurring CHS in both 2018 and 2019 compared to households without any health insurance. Households in urban areas were less likely to incur CHS than those living in rural areas in 2018. The odds of incurring CHS were significantly lower among households where the head was either a private employee or self-employed compared to households where the head was unemployed in 2018. In both years, households with lowest consumption expenditure demonstrated a significantly higher odds of experiencing CHS compared with richer households. The number of children and elderly members within households did not significantly impact the probability of incurring CHS in both years. On the other hand, households seeking health care from private providers were more likely to experience CHS in both 2018 and 2019.
Pooled data analysis
The pooled data analyses with and without an interaction term between insurance type and survey rounds are summarized in Table 5. The interaction term was not statistically significant. JKN membership, residing in an urban area, being a private employee and self-employment became protective factors for incurring CHS. Households with lowest household expenditure had a higher likelihood of incurring CHS compared with richer households. Households visiting private facilities were more likely to experience CHS than households visiting public facilities only. The overall trend of CHS occurrence fell significantly over the two time points (OR = 0.66, P < 0.001).
Sensitivity analysis
When hospital room charges were excluded from the calculation of OOP payments in 2019, the incidence of CHS in 2019 remained similar to the baseline analysis (Appendix Table A2). When the incidence of CHS was defined as the proportion of households spending over 25% of their household consumption expenditure on OOP health care payments, the incidence of CHS fell from 2.7% to 2018 to 1.5% in 2019 (Appendix Table A3). Self-employment was associated with significantly lower likelihood of incurring CHS at the 25% threshold in both years (Appendix Table A4). Being insured under the JKN, living in an urban area, and being a private employee were protective factors in 2018, but not in 2019. On the other hand, the richer households (Q4 and Q5) had significantly lower odds of incurring CHS than the poorest households (Q1) at the 25% threshold in both years. Households with children under five and households with elderly members were more likely to experience CHS in 2019. Results from the pooled data analysis showed that at the 25% threshold, JKN membership, living in an urban area, being a private employee/self-employed, living in richer households, and not using health care, were associated with a significantly lower likelihood of experiencing CHS (Appendix Table A5). Overall, households in the second wave had a significantly lower odds of incurring CHS at the 25% threshold compared to households in the first wave (OR = 0.67, P = 0.005).
Discussion
This study investigated the incidence, determinants and trend of CHS under the JKN in Indonesia. A major finding of this study was that the overall incidence of CHS fell from 7.9% to 2018 to 4.4% in 2019. Among households covered by the JKN, the incidence of CHS was 7.0% in 2018 and 4.0% in 2019, which was lower than estimates among households without insurance and households covered by private insurance. Overall, the incidence of CHS displayed a declining trend over the study period and the change was statistically significant.
Our estimate of the incidence of CHS in 2018 is higher than the number published by the WHO and World Bank in 2021 [5]. Using the 2017 National Socioeconomic Survey (Survei Sosial Ekonomi Nasional, SUSENAS), the WHO and World Bank reported that the incidence of CHS at the 10% threshold was 4.5% in 2017 in Indonesia. But it should be noted that the SUSENAS survey did not collect OOP payments on diagnostic procedures, transportation, food and informal payments (Appendix Table A6). Moreover, the recall period was defined as the past month for all OOP expenditure in the SUSENAS, which might have underestimated the total OOP payments, especially the inpatient OOP costs.
Our study found that membership of the JKN was associated with a lower incidence of CHS during the study period. This finding is consistent with previous Indonesian studies evaluating financial protection under the JKN Program [21,22,23]. However, the level of protection in Indonesia was shown to be inadequate to eliminate OOP payments and in turn CHS for some JKN members. In theory, JKN members should not incur OOP payments when they visit health facilities within the JKN network. But there is evidence that the cost of medical procedures is often higher than the capitation payment and INA-CBG tariffs [24, 25]. As a result, households may still face the burden of OOP health payments even if they are insured under the JKN. Moreover, a new government health financing regulation (Presidential Regulation No. 82) implemented in 2018 enables JKN members to pay OOP for up to 75% of INA-CBG tariffs for an upgrade to an executive clinic or VIP room [12]. This may also explain why some households incurred OOP payments and CHS despite being members of the JKN. However, due to the endogeneity of the JKN program - that arises from the choice to be insured, eligibility for insurance, and differences in the health status of individuals - the causal effect of the JKN on CHS could not be determined using the data collected by this study.
Our study found that the poorest households experienced the highest incidence of CHS and had higher odds of experiencing CHS. This finding is consistent with findings reported in several other countries, including Kenya [26, 27] and China [28]. Despite lower OOP payments among the poorest households, these households still incurred a higher incidence of CHS due to relatively low income. Our data also showed that OOP expenditure was the highest among the richest households. It is likely that richer households are more willing to pay upgrade fees under the JKN scheme. In Indonesia, more than half of the roughly 3,000 hospitals are private hospitals [29] and it is likely that richer households make more use of private health facilities which are more expensive. Richer households may also be willing to pay more for care that is perceived to be of better quality. Improved routine measurement of the quality of care is critical to understanding whether the rich may be spending more to access better quality of care in Indonesia and in other low- and middle-income countries [30,31,32].
The pooled data analysis showed that households in urban areas had lower odds of incurring CHS. This finding is consistent with studies in Peru [33], Bangladesh [34] and Senegal [35]. It also aligns with other studies from Indonesia reporting lower household expenditure (usually used as a proxy of income) in rural areas [36]. Moreover, data published by the Statistics Indonesia (Badan Pusat Statistik - BPS) revealed that between 2014 and 2021, the average monthly household expenditure of urban households increased from IDR 979,000 in 2014 to IDR 1,487,000 in 2021, or by 70%. However, the average monthly household expenditure in rural areas increased by only 52%, from IDR 573,000 in 2014 to IDR 971,000 in 2021 [37]. With the same level of health care costs, the incidence of CHS would be lower for households in urban areas due to the higher average income. In the pooled data analysis, households with a head employed in the private sector or self-employed were less likely to incur CHS compared to households with an unemployed head. Other studies have reported similar findings that having a household head who was unemployed significantly increased the odds of incurring CHS [27, 33]. Households with an employed head will most likely have a higher income than those whose head is unemployed and thus with the same level of OOP spending, these households would have lower levels of CHS.
In the 6,445 households that participated in both surveys, altogether 44 respondents reported not seeking care when they were sick with the main reason being that care was unaffordable. Though forgone health care (or unmet health care needs) due to financial barriers did not appear to be a major issue in the surveyed households, this may be due to the one month recall period used in this study compared to studies in OECD countries which typically ask about spending over the last 12 months [38]. For future studies, we recommend that household surveys include unmet health care needs and also collect information on the reasons for not seeking care.
A number of policy recommendations can be made based on the findings of this study. Firstly, to further reduce OOP spending, we recommend that the government reviews its capitation payments and INA-CBG tariffs to ensure these match the real costs of delivering health care services. Strategic purchasing of health services from providers based on capitation payments and INA-CBG tariffs may also help reduce OOP spending, as health providers who charge patients beyond the maximum cost-sharing threshold face the risk of non-renewal of their contract with government. Secondly, claims submitted to the JKN Administrator by health care providers currently do not include OOP payments for services that are not covered under the JKN or any top-up payments for service upgrades. Inclusion of this information can provide a much better understanding of the financial impact of health spending by households. Thus, we recommend that the JKN Administrator collaborates with BPS to include questions on these types of OOP payments in its annual SUSENAS survey. Collecting this information will also facilitate international comparison with other UN member states for monitoring progress towards the SDGs (specifically the indicators for SDG3.8.2). Finally, a more in-depth analysis is needed to identify those areas of health spending that are placing greatest financial burden on households. For example, it is likely that OOP payments for drugs are more burdensome compared to OOP payments for medical fees, since the prices of drugs tend to increase in line with the exchange rate. In this situation the government could consider implementing a safety net scheme for low-income members of the JKN.
Our study has some limitations. The study coincided with the issuance of a new government health financing regulation allowing JKN members to pay up to 75% of the CBG tariff to upgrade inpatient care to a higher class of hospitalization or change to a “VIP room” or executive clinic. This regulation is believed to have contributed to the high OOP spending by high income groups including some JKN members. In this case, the incidence of CHS may not be the most appropriate measure, as it does not take into account voluntary OOP payments towards such health services. Secondly, this study cannot capture the potential effects of seasonality on service utilization rate and household health spending, as the two survey rounds were conducted in different months of the year. Therefore, cautious interpretation is needed on the changes of CHS incidence between 2018 and 2019. Moreover, outpatient OOP spending during the survey month was multiplied by 12 in order to derive an estimate of annual spending on outpatient services. Again, seasonal variations in monthly OOP payments for outpatient visits were unable to be captured under this approach. Total household consumption expenditure may have also been underestimated as our survey covered only eight common items and excluded other potentially relevant items such as clothing, rent and home appliances. Therefore, interpretation of CHS incidence needs to take into account these complexities. Although the survey covered 74% of the Indonesian population, the findings of our study may not be nationally representative, as we use purposive sampling in order to capture different socioeconomic conditions and demographic characteristics. Finally, this study may be limited by sample selectivity due to attrition. In the analyses, we only included households that could be followed up in the second wave. The proportion of households with non-PBI members and private insurance was significantly higher among those lost to follow-up. Households lost to follow-up were also wealthier. Thus, our estimates of incidence of CHS may be biased due to attrition. Despite these limitations, this study has provided insights into the incidence of CHS and its determinants for the same households at two time points, which has never been done before in the context of Indonesia.
Conclusions
In this study, we aimed to assess the incidence of CHS, factors associated with incurring CHS and trends in CHS under the JKN in Indonesia. This study demonstrated that the overall incidence of CHS decreased in Indonesia between 2018 and 2019. However, a higher incidence of CHS was observed among households in rural areas, non-JKN members, households where household heads were unemployed, and the poorest households. The inequality among those experiencing a high incidence of CHS could be potentially addressed by ensuring health policies such as providing a safety net covering health care expense to low-income households and expanding JKN coverage. While households with JKN membership were found to have a lower incidence of CHS compared to households with private insurance and households without health insurance, the national health insurance scheme has not provided adequate protection to all its members. OOP payments for health care and the risk of CHS still loom high among JKN members. While the higher OOP payments among wealthier households may not appear to be of major concern from an equity perspective, it does require further investigation to assess if these OOP payments are caused by unnecessary prescription of tests and treatment through supplier induced demand. We also need further research to investigate whether CHS pushes households below the poverty line.
Data Availability
Post-processing source data and supplementary data are presented within this study. Proposal to access to the ENHANCE survey datasets should be directed to the corresponding author to gain access. Data requestors will need to sign a data access agreement.
Abbreviations
- UHC:
-
Universal health coverage
- SDGs:
-
Sustainable development goals
- UN:
-
United Nations
- OOP:
-
Out-of-pocket
- NHA:
-
National Health Accounts
- CHS:
-
Catastrophic health spending
- WHO:
-
World Health Organization
- JKN:
-
Jaminan Kesehatan Nasional
- BPJS:
-
Badan Penyelenggara Jaminan Sosial
- INA-CBG:
-
Indonesian Case Base Groups
- IDR:
-
Indonesian Rupiah
- SUSENAS:
-
Survei Sosial Ekonomi Nasional
References
United Nations. Global indicator framework for the Sustainable Development Goals and targets of the 2030 Agenda for Sustainable Development New York: United Nations. ; 2023 [Available from: https://unstats.un.org/sdgs/indicators/indicators-list/.
World Health Organization. The world health report: health systems financing: the path to universal coverage Geneva: World Health Organization; 2010 [updated 2010. Available from: https://apps.who.int/iris/handle/10665/44371.
United Nations. UN High-Level Meeting on Universal Health Coverage 2019 2019 [Available from: https://www.un.org/pga/73/event/universal-health-coverage/.
Wagstaff A, Eozenou P, Smitz M. Out-of-Pocket Expenditures on Health: A Global Stocktake. World Bank Res Obs. 2020;35(2):123–57.
World Health Organization, the International Bank for Reconstruction and Development/the World Bank. Tracking universal health coverage: 2021 Global Monitoring Report 2021 [Conference Edition:[Available from: https://www.who.int/publications/i/item/9789240040618.
Kementerian Kesehatan [Ministry of Health]. National Health Accounts Indonesia 2020 Jakarta: Ministry of Health; 2022 [Available from: https://ejournal2.litbang.kemkes.go.id/index.php/lpb/article/view/6406.
World Health Organization. Global spending on health: Rising to the pandemic’s challenges Geneva: World Health Organization. ; 2022 [Available from: https://apps.who.int/iris/bitstream/handle/10665/365133/9789240064911-eng.pdf.
Xu K, Evans DB, Carrin G, Aguilar-Rivera AM, Musgrove P, Evans T. Protecting households from catastrophic health spending. Health Aff (Millwood). 2007;26(4):972–83.
McHenga M, Chirwa GC, Chiwaula LS. Impoverishing effects of catastrophic health expenditures in Malawi. Int J Equity Health. 2017;16(1):25.
Wagstaff A, Flores G, Hsu J, Smitz MF, Chepynoga K, Buisman LR, et al. Progress on catastrophic health spending in 133 countries: a retrospective observational study. Lancet Glob Health. 2018;6(2):e169–e79.
World Health Organization, the International Bank for Reconstruction and Development/the World Bank. Tracking universal health coverage: 2017 global monitoring report: executive summary Geneva: World Health Organization; 2017 [updated 2017. Available from: https://apps.who.int/iris/handle/10665/260522.
Peraturan Presiden [Presidential decree]. Perubahan Kedua atas Peraturan Presiden Nomor 82 Tahun 2018 tentang Jaminan Kesehatan [Second Amendment to Presidential Regulation Number 82 of. 2018 concerning Health Insurance] Jakarta The Supreme Audit Agency of the Republic of Indonesia; 2020 [Available from: https://peraturan.bpk.go.id/Home/Details/136650/perpres-no-64-tahun-2020.
Kementerian Kesehatan [Ministry of Health]. Peraturan Menteri Kesehatan tentang Pedoman Indonesian Case Base Groups (INA-CBG) dalam Pelaksanaan Jaminan Kesehatan Nasional [Minister of Health Regulation on Indonesian Case Base Groups (INA-CBG) Guidelines in the Implementation of National Health Insurance] Jakarta: Ministry of Health. ; 2016 [Available from: https://peraturan.bpk.go.id/Home/Details/114633/permenkes-no-76-tahun-2016.
Dewan Jaminan Sosial Nasional [National Social Security Council]. Sistem Monitoring dan Evaluasi Program JKN [JKN Program Monitoring and Evaluation System]. 2021 [Available from: http://sismonev.djsn.go.id/kepesertaan/?jumpto=map_canvas.
The World Bank. Universal Health Coverage Global Monitoring Data – 2021 2022 [Available from: https://datacatalog.worldbank.org/search/dataset/0060802/Universal-Health-Coverage-Global-Monitoring-Data2021.
World Bank. Indonesia public expenditure review 2020: spending for better results: World Bank Washington, DC. ; 2020 [Available from: https://openknowledge.worldbank.org/handle/10986/33954.
Cheng Q, Asante A, Susilo D, Satrya A, Man N, Fattah RA, et al. Equity of health financing in Indonesia: a 5-year financing incidence analysis (2015–2019). Lancet Reg Health - Western Pac. 2022;21:100400.
Wiseman V, Thabrany H, Asante A, Haemmerli M, Kosen S, Gilson L, et al. An evaluation of health systems equity in Indonesia: study protocol. Int J Equity Health. 2018;17(1):138.
Kementerian Keuangan [Ministry of Finance]. Peraturan Menteri Keuangan Republik Indonesia Nomor 116/PMK.07/2021 tentang Peta Kapasitas Fiskal Daerah [Ministry of Finance Regulation No. 116/PMK/07/2021 on Maps of Local Fiscal Capacity] Jakarta Ministry of Finance; 2021 [Available from: https://jdih.kemenkeu.go.id/in/dokumen/peraturan/e76f2c86-4b60-40b8-c92c-08d971d072b7.
Horodnic AV, Williams CC, Ciobanu CI, Druguș D. Informal payments by patients, institutional trust and institutional asymmetry. Front Psychol. 2022;13:1015208.
Agustina R, Dartanto T, Sitompul R, Susiloretni KA, Suparmi, Achadi EL, et al. Universal health coverage in Indonesia: concept, progress, and challenges. The Lancet. 2019;393(10166):75–102.
Wahyu Pudji N, Risky Kusuma H. Determinan Pengeluaran Kesehatan Katastropik Rumah Tangga Indonesia Pada Tahun Pertama Implementasi Program JKN. Indonesian Bull Health Res. 2017;45(1):27–36.
National Institute for Health Research and Development (Badan Litbangkes). The role of National Health Insurance (JKN) in reducing the financial burden of childbirth Jakarta: Badan Litbangkes Kementerian Kesehatan. ; 2019 [Available from: http://www.healthpolicyplus.com/pubs.cfm?get=17359-17651.
Ekawati FM, Claramita M. Indonesian General Practitioners’ experience of practicing in primary care under the implementation of Universal Health Coverage Scheme (JKN). J Prim Care Community Health. 2021;12:21501327211023707.
Satibi S, Andayani TM, Endarti D, Suwantara IPT, Agustini NPD. Comparison of real cost Versus the Indonesian Case Base Groups (INA-CBGs) Tariff Rates among patients of high- incidence cancers under the National Health Insurance Scheme. Asian Pac J Cancer Prev. 2019;20(1):117–22.
Chuma J, Maina T. Catastrophic health care spending and impoverishment in Kenya. BMC Health Serv Res. 2012;12(1):413.
Barasa EW, Maina T, Ravishankar N. Assessing the impoverishing effects, and factors associated with the incidence of catastrophic health care payments in Kenya. Int J Equity Health. 2017;16(1):31.
Liu H, Zhu H, Wang J, Qi X, Zhao M, Shan L, et al. Catastrophic health expenditure incidence and its equity in China: a study on the initial implementation of the medical insurance integration system. BMC Public Health. 2019;19(1):1761.
Direktorat Jenderal Pelayanan Kesehatan Kementerian Kesehatan RI. Informasi Rumah Sakit Indonesia (Information of Indonesian Hospital) [Available from: http://sirs.yankes.kemkes.go.id/fo/.
Pratiwi AB, Setiyaningsih H, Kok MO, Hoekstra T, Mukti AG, Pisani E. Is Indonesia achieving universal health coverage? Secondary analysis of national data on insurance coverage, health spending and service availability. BMJ Open. 2021;11(10):e050565.
Selvaraj S, Farooqui HH, Karan A. Quantifying the financial burden of households’ out-of-pocket payments on medicines in India: a repeated cross-sectional analysis of National Sample Survey data, 1994–2014. BMJ Open. 2018;8(5):e018020.
Tangcharoensathien V, Patcharanarumol W, Ir P, Aljunid SM, Mukti AG, Akkhavong K, et al. Health-financing reforms in southeast Asia: challenges in achieving universal coverage. Lancet. 2011;377(9768):863–73.
Proaño Falconi D, Bernabé E. Determinants of catastrophic healthcare expenditure in Peru. Int J Health Econ Manage. 2018;18(4):425–36.
Khan JAM, Ahmed S, Evans TG. Catastrophic healthcare expenditure and poverty related to out-of-pocket payments for healthcare in Bangladesh-an estimation of financial risk protection of universal health coverage. Health Policy Plan. 2017;32(8):1102–10.
Séne LM, Cissé M. Catastrophic out-of-pocket payments for health and poverty nexus: evidence from Senegal. Int J Health Econ Manag. 2015;15(3):307–28.
Direktorat Statistik Kesejahteraan Rakyat [Directorate of Social Welfare Statistic]. Pengeluaran untuk Konsumsi Penduduk Indonesia, September 2021 [Consumption Expenditure of Population of Indonesia, September 2021] Jakarta: BPS-Statistics Indonesia; 2022 [Available from: https://www.bps.go.id/publication/2022/06/23/2ab66056b248b86057743ba4/pengeluaran-untuk-konsumsi-penduduk-indonesia-september-2021.html.
Maulana A, Purwaningrum F, Thabrany H, Fitrianti Y, Hartini F. Mengukur Kemampuan Mengiur untuk Jaminan Kesehatan Nasional (JKN) tahun 2021 di Indonesia. Jurnal Jaminan Kesehatan Nasional. 2022;2(1):39–52.
OECD. Focus on unmet needs for health care. : Comparing approached and results from international surveys 2020 [Available from: https://www.oecd.org/health/health-systems/Unmet-Needs-for-Health-Care-Brief-2020.pdf.
Acknowledgements
The ENHANCE Study (Equity and Health Care Financing in Indonesia) was supported through the Health Systems Research Initiative in the UK, and is jointly funded by the Department of International Development, the Economic and Social Research Council, the Medical Research Council and the Wellcome Trust. The funders of this research were not involved in the study. The research would not have been possible without the time and support of all the families and field workers that took part in our household surveys, to them we are very grateful.
Funding
This study is supported by a grant from the Health Systems Research Initiative in the UK, jointly funded by the Department of International Development, the Economic and Social Research Council, the Medical Research Council and the Wellcome Trust (MR/P013996/1).
Author information
Authors and Affiliations
Contributions
HT, VW, AA, SK, LG, AM, AH, VT and SJ conceived and designed the study. VW and AA co-supervised the study. DS, RAF, DN, GC, EA contributed to data curation. RAF and QC conducted the data analysis and have directly accessed and verified the underlying data reported in the manuscript. All authors contributed to the interpretation of the results. RAF and QC drafted the manuscript which all authors commented on. All authors critically reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Informed written consent was obtained from all subjects and ethical support has been granted by all relevant bodies including: the University of Indonesia (Reference: 503/H2.F10/PPM.00.02/2017); London School of Hygiene & Tropical Medicine (Reference: 13773); and the University of New South Wales (Reference: HC17709).
Consent for publication
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Fattah, R.A., Cheng, Q., Thabrany, H. et al. Incidence of catastrophic health spending in Indonesia: insights from a Household Panel Study 2018–2019. Int J Equity Health 22, 185 (2023). https://doi.org/10.1186/s12939-023-01980-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12939-023-01980-w