
Abstract
Background
Insulin resistance (IR) is linked to both the complexity of coronary artery lesions and the prognosis of acute coronary syndrome (ACS). However, the precise extent of this correlation and its impact on adverse cardiovascular outcomes in ACS patients remain unclear. Therefore, this study aims to investigate the intricate relationship between IR, coronary artery lesion complexity, and the prognosis of ACS through a cohort design analysis.
Method
A total of 986 patients with ACS who underwent percutaneous coronary intervention (PCI) were included in this analysis. IR was assessed using the triglyceride-glucose (TyG) index, while coronary artery lesion complexity was evaluated using the SYNTAX score. Pearson’s correlation coefficients were utilized to analyze the correlations between variables. The association of the TyG index and SYNTAX score with major adverse cardiovascular events (MACEs) in ACS was investigated using the Kaplan-Meier method, restricted cubic splines (RCS), and adjusted Cox regression. Additionally, a novel 2-stage regression method for survival data was employed in mediation analysis to explore the mediating impact of the SYNTAX score on the association between the TyG index and adverse cardiovascular outcomes, including MACEs and unplanned revascularization.
Results
During a median follow-up of 30.72 months, 167 cases of MACEs were documented, including 66 all-cause deaths (6.69%), 26 nonfatal myocardial infarctions (MIs) (2.64%), and 99 unplanned revascularizations (10.04%). The incidence of MACEs, all-cause death, and unplanned revascularization increased with elevated TyG index and SYNTAX score. Both the TyG index (non-linear, P = 0.119) and SYNTAX score (non-linear, P = 0.004) displayed a positive dose-response relationship with MACEs, as illustrated by the RCS curve. Following adjustment for multiple factors, both the TyG index and SYNTAX score emerged as significant predictors of MACEs across the total population and various subgroups. Mediation analysis indicated that the SYNTAX score mediated 25.03%, 18.00%, 14.93%, and 11.53% of the correlation between the TyG index and MACEs in different adjusted models, respectively. Similar mediating effects were observed when endpoint was defined as unplanned revascularization.
Conclusion
Elevated baseline TyG index and SYNTAX score were associated with a higher risk of MACEs in ACS. Furthermore, the SYNTAX score partially mediated the relationship between the TyG index and adverse cardiovascular outcomes.
Similar content being viewed by others

Introduction
The implementation of reperfusion strategies and the improvement of regional coordinated treatment systems have notably decreased acute-phase mortality among patients with acute coronary syndrome (ACS) [1, 2]. However, despite these advancements, the incidence of long-term adverse events following percutaneous coronary intervention (PCI) continues to rise due to population accumulation [3]. Early identification of high-risk patients and the management of relevant risk factors are beneficial for improving the long-term prognosis of ACS patients [4].
Elevated levels of insulin resistance (IR) have been consistently shown to not only correlate with the development and progression of atherosclerotic cardiovascular disease [5,6,7] but also be connected to a heightened susceptibility to adverse cardiovascular events [8]. The triglyceride-glucose (TyG) index is widely recognized as a non-invasive, cost-effective, and reliable indicator of IR, comparable to the homeostasis model assessment of insulin resistance (HOMA-IR) [9]. Recent studies have shown that an elevated TyG index is independently associated with the development and progression of a range of cardiovascular diseases, such as myocardial infarction [10], coronary artery calcification [11, 12], peripheral artery disease [13], and stroke [14]. Furthermore, it has been noted to be significantly linked to the complexity of coronary artery disease and adverse cardiovascular events following coronary artery revascularization, regardless of the presence of diabetes [15, 16].
Additionally, multiple previous studies have consistently demonstrated a significant correlation between the complexity of coronary artery lesions and the long-term adverse outcomes subsequent to PCI in ACS, encompassing mortality rates and the necessity for repeat revascularization procedures [17, 18]. The SYNTAX (Synergy Between Percutaneous Coronary Intervention) score is a well-established scoring system utilized to assess the complexity of coronary artery disease (CAD) based on various anatomic risk factors evaluated by angiography [19]. Based on our initial research, we have observed that IR, as measured by the TyG index, is independently linked to a greater likelihood of increased coronary anatomical complexity (SYNTAX score > 22) in patients with ACS [15]. Nonetheless, further evidence is required to better comprehend the intricate relationship between IR, coronary artery lesion complexity, and adverse cardiovascular outcomes, contributing to a more thorough insight into IR as a critical prognostic factor for coronary artery disease.
Therefore, this study aimed to investigate the relationship between IR assessed by the TyG index and the complexity of coronary artery lesions evaluated by the SYNTAX score with long-term adverse outcomes following PCI in patients with ACS. Moreover, we examined whether the link between IR and adverse cardiovascular outcomes is partly mediated by the complexity of coronary artery lesions.
Methods
Study population
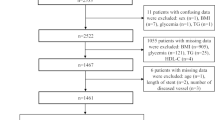
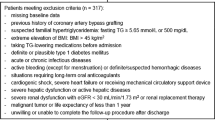
We consecutively enrolled 986 patients hospitalized at the Third People’s Hospital of Chengdu (Sichuan, China) undergoing coronary angiography and diagnosed with ACS from July 2018 to December 2020. Exclusion criteria were as follows: (1) a history of coronary artery bypass grafting (CABG); (2) critical structural heart disease requiring intervention; (3) severe hepatic, respiratory, or renal insufficiency (creatinine clearance < 15 ml/min); (4) advanced hematological or solid tumors with a limited life expectancy; (5) death during hospitalization; (6) incomplete critical medical data exceeding 10%. This study was approved by the ethics committee of the Third People’s Hospital of Chengdu and strictly complied with the Declaration of Helsinki. All participants provided informed consent either in written or oral form.
Data collection and definitions
Demographic information, medical history, smoking status, and specific medical details were systematically extracted from patients’ electronic health records. The collection included historical health events like prior percutaneous coronary intervention (PCI), chronic obstructive pulmonary disease (COPD), hypertension, diabetes mellitus, stroke, and atrial fibrillation (AF). These historical details were corroborated by medical records following initial self-reports. ACS encompassed conditions such as unstable angina, ST-segment elevation myocardial infarction (STEMI), and non-ST-segment elevation myocardial infarction (NSTEMI), with diagnoses made in accordance with respective guidelines [20]. The identification of diabetes mellitus [21] was based on either the self-reported use of antidiabetic medications or elevated blood glucose readings, characterized by casual blood glucose levels of 11.1mmol/L or higher, fasting blood glucose levels of 7.0mmol/L or higher, or 2-hour postprandial levels exceeding 11.1mmol/L following a 75 g oral glucose tolerance test. Hypertension was identified through a consistent record of blood pressure readings of 140/90mmHg or above, or the ongoing use of antihypertensive medication [22].
Fasting venous blood samples were collected to measure the plasma levels of total cholesterol (TC), triglycerides (TG), LDL-C, HDL-C, fasting blood glucose (FBG), serum creatinine, brain natriuretic peptide (BNP), and cardiac troponin T (cTnT), fibrinogen (Fib), Homocysteine (Hcy), employing standard laboratory methods. The left ventricular ejection fraction (LVEF) was measured using the two-dimensional modified Simpson’s method, providing essential data for evaluating cardiac function.
The TyG index was determined using the formula: ln [TG (mg/dL) ×FBG (mg/dL)/2]. To compute the baseline SYNTAX score (bSS), a web-accessible calculator (http://syntaxscore.com/) was utilized, with two independent evaluators analyzing the preprocedural angiograms without knowledge of initial clinical features and outcomes. In instances of disagreement, a third evaluator’s input was sought to reach a consensus. All data were entered into a dedicated computer database and assessed for quality.
Follow-up and endpoints
Follow-up assessments were conducted at 1, 3, 6, and12 months post-discharge, and subsequently every 12 months, either through phone calls or in-person clinic visits. Trained professionals documented any clinical events that occurred during follow-up duration. The primary endpoint was major adverse cardiovascular events (MACEs), which encompassed all-cause death, nonfatal myocardial infarction (MI) and unplanned revascularization. Secondary endpoint included cardiac death, unplanned revascularization, and nonfatal stroke. Verification of all clinical endpoints was achieved through review of medical records as needed. Death from any cause was categorized under all-cause death. Unplanned revascularization was defined as ischemia-driven revascularization due to lesion progression or in-stent restenosis during follow-up after the index procedures. The diagnosis of MI and stroke is established in accordance with internationally recognized guidelines.
Statistical analysis
Continuous variables were characterized by the mean ± SD or the median with interquartile range (IQR), based on the data’s distribution normality. Group differences were analyzed using t-tests or Mann–Whitney U tests accordingly. Categorical variables were summarized as frequencies and percentages, and comparisons between groups were performed using the chi-square (χ2) test or Fisher’s exact test. Correlations among variables, such as the TyG index and baseline SYNTAX score, were evaluated using Pearson’s correlation coefficients. Additionally, a heatmap was created to visually represent each correlation coefficient. The incidence of adverse cardiovascular events in different groups was assessed by the Kaplan–Meier method based on the TyG index and SYNTAX score groups, respectively. Discrepancies between groups were evaluated by log-rank tests.
The dose-response association between the TyG index, baseline SYNTAX score, and adverse cardiovascular outcomes in patients with ACS was illustrated through the use of restricted cubic splines (RCS) curve. Cox regression models were employed to assess the relationship between the TyG index, baseline SYNTAX score, and the incidence of adverse cardiovascular outcomes. Hazard ratio (HR) with 95% confidence interval (CI) were calculated within a time-to-event framework. Additionally, several subgroup analyses were conducted to explore whether the predictive utility of the TyG index and baseline SYNTAX score remained consistent across patients with diverse demographic characteristics or comorbidities. To assess the impact of the TyG index (exposure) on MACEs (outcome) via SYNTAX score (mediator), we employed VanderWeele’s two-stage regression approach for survival data [23]. This method involves fitting two distinct regression models: one for the mediator and another for the outcome. By integrating the parameter estimates and standard errors from both models as per VanderWeele’s specified formulas, we derived the mediation effect size. Specifically, we utilized Cox proportional hazards regression to analyze the outcome (MACEs) and linear regression for the mediator (SYNTAX score). The significance of the mediating effect was assessed through the examination of 1000 bootstrap samples. The same approach was used to assess the effect of the TyG index (exposure) mediated by the SYNTAX score (Mediator) on unplanned revascularization (outcome).
In mediation analysis, subgroup analysis, and COX regression analysis, we employed multiple adjusted models, adjusting various covariates independently, to thoroughly evaluate the robustness and reliability of the findings. In all adjusted models, Model I was adjusted for age, sex, BMI, hypertension, diabetes mellitus, smoking, Previous PCI, serum creatinine. Model II was adjusted for age, BMI, serum creatinine, Diuretics, Fib, acute myocardial infarction (AMI), LVEF. Model III was adjusted for age, sex, BMI, hypertension, diabetes mellitus, smoking, Previous PCI, serum creatinine, Diuretics, Fib, AMI, LVEF. All statistical analyses in the present study were performed with SPSS 24.0 (IBM, Armonk, New York), R Programming Language 4.0.2, Stata/MP 16.0 software and MedCalc19.1 (MedCalc software, Belgium). All tests were 2-sided, and P < 0.05 was considered statistically significant.
Results
Baseline characteristics
The final cohort consisted of 986 participants who were eligible for the final analysis. The mean age of the population was 66.61 ± 11.42 years. Over a median follow-up period of 30.72 months (interquartile range: 26.13 to 35.07 months), There were 167 (16.94%) cases of MACEs observed, including 66 (6.69%) all-cause deaths, 26 (2.64%) nonfatal MIs, and 99 (10.04%) unplanned revascularizations. Baseline characteristics of the study population are presented in Table 1. Individuals who experienced MACEs were generally older and exhibited higher levels of cTnT, BNP, serum creatinine, uric acid, FBG, TG, Fib, TyG index, and SYNTAX score. They also had lower LVEF, a higher incidence of AMI, and greater usage of insulin and diuretics upon discharge compared to those without MACEs. Furthermore, a heatmap was depicted to visualize the correlations between different variables, revealing a significant positive association between the TyG index and SYNTAX score (r = 0.22, P < 0.001, Fig. 1).

A heatmap illustrating the correlation between different variables. BMI, body mass index; SBP, systolic blood pressure; HR, heart rate; UA, Uric acid; FBG, fasting blood glucose; TG, triglyceride; TC, total cholesterol; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; Fib, fibrinogen; Hcy, Homocysteine; EF, left ventricular ejection fraction; Cr, Serum creatinine; TyG index, the triglyceride–glucose index; bSS, baseline SYNTAX score. The intensity of color reflects the strength of the correlation
Association between the TyG index, SYNTAX score, and the incidence of MACEs
Patients were categorized into low-risk (SYNTAX score ≤ 22) and medium/high-risk (SYNTAX score > 22) groups based on the SYNTAX score. Simultaneously, patients were divided into a lower TyG index group (TyG index < 8.95) and a higher TyG index group (TyG index ≥ 8.95) according to the median value of the TyG index. The incidence of major adverse cardiovascular events (MACEs), all-cause death, and unplanned revascularization increased with elevated TyG index and SYNTAX score (Fig. 2 and Additional File: Table S1, Figure S1).

Cumulative incidence of MACEs during follow-up stratified by the TyG index value (A) and SYNTAX score (B). TyG index, the triglyceride–glucose index; bSS, baseline SYNTAX score; MACEs, major adverse cardiovascular events
Furthermore, both the TyG index (non-linear, P = 0.119) and SYNTAX score (non-linear, P = 0.004) displayed a positive dose-response relationship with MACEs when analyzed as continuous variables, as depicted by the restricted cubic spline (RCS) curve (Fig. 3). Univariate COX regression showed that the TyG index, age, BMI, AMI, serum creatinine, FBG, TG, Fib, SYNTAX score, LVEF, diuretics, and insulin were risk factors for incidence of MACEs (Additional File: Table S2). The TyG index and SYNTAX score were included as continuous variables in multivariate Cox regression analysis. After adjusting for multiple confounding factors, both an elevated TyG index (Model I: HR 1.9024, 95% CI: 1.3803–2.6219, P = 0.0001; Model II: HR 1.6682, 95% CI: 1.2682–2.1944, P = 0.0003; Model III: HR 1.9674, 95% CI: 1.4346–2.6979, P = 0.0001) and SYNTAX score (Model I: HR 1.0342, 95% CI: 1.0174–1.0512, P = 0.0001; Model II: HR 1.0269, 95% CI: 1.0094–1.0447, P = 0.0024; Model III: HR 1.0251, 95% CI: 1.0073–1.0432, P = 0.0055) were associated with an increased risk of MACEs in patients with ACS undergoing PCI (Table 2).

Dose-responsive relationship of the TyG index (A) and SYNTAX score (B) with the risk of with MACEs in ACS undergoing PCI. TyG index, the triglyceride–glucose index; bSS, baseline SYNTAX score; HR, hazard ratio; CI, confidence interval
The predictive value of the TyG index for MACE in various subgroups
Various subgroup analyses were also conducted to assess whether the predictive value of the TyG index and SYNTAX score remained consistent across diverse demographic characteristics or comorbidities. Figure 4 presents the association between the TyG index and SYNTAX score with MACEs, stratified by age, sex, BMI, diabetes, hypertension, smoking status, and type of ACS. We discovered, after adjusting for multiple factors, that both the TyG index and SYNTAX score emerged as significant predictors of MACEs across various subgroups.

Forest plot illustrating the association of the TyG index and baseline SYNTAX score with the risk of MACEs in ACS undergoing PCI stratified by different subgroups. TyG index, the triglyceride–glucose index; bSS, baseline SYNTAX score; BMI, body mass index; ACS, acute coronary syndrome; NSTE-ACS, non-ST-segment elevation acute coronary syndrome; STEMI, ST-segment elevation myocardial infarction; CTO, chronic total occlusion; HR was evaluated by 1-point increase of the TyG index and SYNTAX score. HR, hazard ratio; CI, confidence interval. All models were adjusted for age, sex, BMI, hypertension, diabetes mellitus, smoking, Previous PCI, serum creatinine, Diuretics, Fib, AMI, LVEF.
Mediation analysis
As demonstrated in Table 3; Fig. 5, the mediation analysis revealed that the complexity of coronary artery lesions, as reflected by the SYNTAX score, exerted a significant partial mediating effect on the relationship between IR, as reflected by the TyG index, and the incidence of MACEs across multiple adjusted models. In particular, the mediation proportions of an elevated SYNTAX score were 25.03% (CI: 12.88 − 53.44%, P<0.05), 18.00% (CI: 7.94 − 39.84%, P<0.05), 14.93% (CI: 4.67 − 36.63%, P<0.05), and 11.53% (CI: 2.80 − 28.64%, P<0.05) in the unadjusted, adjusted Model I, adjusted Model II, and adjusted Model III analyses, respectively. Moreover, similar mediating effects were observed when cardiovascular adverse events were defined as unplanned revascularization. The result shows that the mediation proportions of an elevated SYNTAX score were 27.18% (CI: 10.03 − 88.50%, P<0.05), 17.96% (CI: 5.26 − 48.52%, P<0.05), 20.26% (CI: 6.23 − 77.18%, P<0.05), and 13.16% (CI: 3.71 − 36.62%, P<0.05) in the unadjusted, adjusted Model I, adjusted Model II, and adjusted Model III analyses, respectively (Additional File: Table S3, Figure S2).

Decomposition of the total association of the TyG index and the risk of MACEs in ACS undergoing PCI into direct and indirect associations mediated by baseline SYNTAX score in different adjusted models, respectively. TyG index, the triglyceride–glucose index; MACEs, major adverse cardiovascular events; CI, confidence interval; PM, proportion mediated. All effects are presented by β coefficients. A represents the unadjusted Model; B represents the adjusted Model I; C represents the adjusted Model II; D represents the adjusted Model III. Model I was adjusted for age, sex, BMI, hypertension, diabetes mellitus, smoking, Previous PCI, serum creatinine; Model II was adjusted for age, BMI, serum creatinine, Diuretics, Fib, AMI, LVEF; Model III was adjusted for age, sex, BMI, hypertension, diabetes mellitus, smoking, Previous PCI, serum creatinine, Diuretics, Fib, AMI, LVEF.
Discussion
In this retrospective cohort study involving 986 individuals with ACS followed for up to 30.72 months, an significant association was found between elevated baseline TyG index, SYNTAX score, and a higher incidence of MACEs post index PCI. These associations retained their statistical significance even after accounting for established cardiovascular disease risk factors in different models and subgroup analyses. Furthermore, the study indicated that the elevated SYNTAX score partly mediated the connection between the TyG index and adverse cardiovascular outcomes, including MACEs and unplanned revascularization, in ACS patient following PCI.
IR, assessed by the homeostasis model assessment of insulin resistance (HOMA-IR), is a metabolic disorder significantly associated with the initiation and advancement of atherosclerosis and cardiovascular disease [5,6,7]. This condition results in elevated blood glucose levels and excessive insulin secretion, potentially triggering abnormal inflammation and lipid metabolism, thus accelerating atherosclerosis development [24]. In patients with normal glucose tolerance and coronary artery disease, IR, as evaluated by HOMA-IR, is associated not only with the severity of coronary artery disease [25] but also with restenosis and the need for overall new PCI [26]. Numerous studies have validated the TyG index as a direct and cost-effective method for evaluating IR levels, serving as a substitute for HOMA-IR [9]. It is associated with cardiovascular prognosis in various conditions, such as myocardial infarction [16], stroke [14], type 2 diabetes mellitus [27], fatty liver [28], metabolic syndrome [28], and other diseases. Additionally, previous research has elucidated the relationship between the TyG index and long-term adverse cardiovascular events, as well as in-stent restenosis and recurrent revascularization following PCI [29,30,31]. In line with existing studies, our research illustrated an independent association between a higher TyG index and MACEs in different models and subgroup analyses. The analysis of the restricted cubic spline (RCS) curve revealed a positive dose-response relationship between the TyG index and MACEs, indicating that the incidence of MACEs rises with increasing TyG index levels.
Prior research has shown that IR impacts cardiovascular outcomes by enhancing the advancement of atherosclerosis [6], arterial calcification [11], renal dysfunction [32], inflammation [33], and other mechanisms. The complexity of coronary artery lesions is a strong predictor of adverse cardiovascular outcomes and is associated with elevated TyG index levels [15]. Won KB et al. found that the TyG index serves as an independent predictor for the progression of coronary artery calcification, particularly noticeable in individuals initially lacking significant coronary artery calcification [11]. In a study involving 2792 participants, an elevated TyG index was associated with an increased risk of multi-vessel coronary artery disease (CAD) [34]. Our previous research also revealed a significant positive correlation between the TyG index and SYNTAX scores in patients with ACS undergoing coronary angiography [15]. The SYNTAX score is determined through a comprehensive assessment of coronary lesion quantity, severity, and distribution [19]. A high SYNTAX score indicates intricate and severe coronary artery disease, which is linked to a poorer clinical prognosis [17]. Based on these findings, we hypothesize that coronary artery lesion complexity may play a crucial role as a mediator in the relationship between IR and the risk of MACEs following PCI. To our knowledge, this study represents a pioneering analysis examining the mediating role of the SYNTAX score in the association between the TyG index and the long-term risk of adverse cardiovascular events following PCI.
This study elucidates the mediating function of the SYNTAX score in the correlation between the TyG index and adverse cardiovascular outcomes including MACEs and unplanned revascularization following PCI, thereby amalgamating prior evidence into a holistic pathway for informing clinical decision-making. Globally, there has been a consistent rise in the volume of patients receiving coronary intervention. Individuals with coronary heart disease, particularly those with type 2 diabetes mellitus (T2DM) or intricate coronary artery lesions like left main or multi-vessel lesions, maintain a heightened susceptibility to recurring adverse cardiovascular incidents [4, 18]. Hence, prompt recognition of high-risk patients with unfavorable prognoses is imperative. In clinical practice, evaluating IR in patients with coronary artery disease enhances the overall disease assessment and facilitates the development of more effective, personalized treatment and management strategies. Moreover, comprehending the correlation between IR and the severity of coronary artery disease, along with cardiovascular adverse events, enables physicians to better evaluate patient risk and promptly identify and address potential complications.
Besides, even in patients with normal glucose tolerance, IR is still not only associated with the severity of coronary artery disease but also with restenosis and the overall need for new percutaneous coronary interventions. Therefore, proactive interventions targeting IR, including lifestyle interventions [35] and pharmacotherapy (such as metformin [36, 37], GLP-1 receptor agonists [38], SGLT-2 inhibitors [39], and DPP-4 inhibitors [40]), along with comprehensive cardiovascular risk management, are expected to reduce the long-term cardiovascular adverse events in this susceptible population.
Limitations
While this study provides valuable information, it also poses certain limitations that warrant careful consideration. Primarily, the single-center, observational design restricts our ability to establish a causal link between the TyG index, SYNTAX score, and adverse cardiovascular events following PCI. Additionally, despite adjustments for known cardiac risk factors, the inherent nature of the observational design means that not all confounding variables may have been accounted for, leaving room for potential residual confounding effects. Furthermore, this study did not employ the HOMA-IR to evaluate the level of IR, precluding a comparative analysis between the TyG index and HOMA-IR in our research context. Moreover, aside from its impact on the complexity of coronary artery lesions, IR can provoke inflammatory responses [8], leading to reduced left ventricular systolic function [41] and renal impairment [32], thereby increasing the risk of adverse cardiovascular events following ischemic coronary events. Further investigation is necessary to explore the intricate relationships among these factors in the future. Finally, given that the study’s cohort consisted solely of Chinese patients, the applicability of these findings across different ethnic groups necessitates further validation.
Conclusion
This study illustrated the significance of the TyG index and SYNTAX score in identifying patients at a higher risk of MACEs following PCI. It also proposed that the complexity of coronary lesions, evaluated by the SYNTAX score, might partly mediate the connection between IR (as indicated by the TyG index) and the probability of adverse cardiovascular outcomes including MACEs and unplanned revascularization. Targeting IR through specific therapies could provide additional advantages in attenuating cardiovascular risks. The results underscore the importance of integrating metabolic and anatomical evaluations to enhance risk stratification in individuals with ACS.
Data availability
The datasets used and/or analyzed in the study are available from the corresponding author upon reasonable request.
References
Zhang YM, Cheng LC, Zhou MG, Chen YZ, Zhu F, Cui CY, Li SY, Cai L. Effect of regional cooperative rescue systems based on chest pain centers for patients with acute myocardial infarction in a first-tier city in China[. J] Intern Emerg Med. 2021;16:2069–76.
Collet JP, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, Dendale P, Dorobantu M, Edvardsen T, Folliguet T, Gale CP, Gilard M, Jobs A, Jüni P, Lambrinou E, Lewis BS, Mehilli J, Meliga E, Merkely B, Mueller C, Roffi M, Rutten FH, Sibbing D, Siontis GCM. 2020 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation[. J] Eur Heart J. 2021;42:1289–367.
Mensah GA, Fuster V, Murray CJL, Roth GA. Global Burden of Cardiovascular diseases and risks, 1990–2022.[J].J am Coll Cardiol. 2023; 82:2350–473.
Batra G, Lindbäck J, Becker RC, Harrington RA, Held C, James SK, Kempf T, Lopes RD, Mahaffey KW, Steg PG, Storey RF, Swahn E, Wollert KC, Siegbahn A, Wallentin L. Biomarker-based prediction of recurrent ischemic events in patients with Acute Coronary syndromes.[J]. J Am Coll Cardiol. 2022;80:1735–47.
Devesa A, Fuster V, Vazirani R, García-Lunar I, Oliva B, España S, Moreno-Arciniegas A, Sanz J, Perez-Herreras C, Bueno H, Lara-Pezzi E, García-Alvarez A, de Vega VM, Fernández-Friera L, Trivieri MG, Fernández-Ortiz A, Rossello X, Sanchez-Gonzalez J, Ibanez B. Cardiac insulin resistance in subjects with metabolic syndrome traits and early subclinical atherosclerosis.[J].Diabetes Care. 2023; 46:2050–7.
Iglesies-Grau J, Garcia-Alvarez A, Oliva B, Mendieta G, García-Lunar I, Fuster JJ, Devesa A, Pérez-Herreras C, Fernández-Ortiz A, Brugada R, Ibanez B, Fernandez-Jimenez R, Fuster V. Early insulin resistance in normoglycemic low-risk individuals is associated with subclinical atherosclerosis.[J].Cardiovasc Diabetol. 2023; 22:350.
Ormazabal V, Nair S, Elfeky O, Aguayo C, Salomon C, Zuñiga FA. Association between insulin resistance and the development of cardiovascular disease[. J] Cardiovasc Diabetol. 2018;17:122.
Laakso M, Kuusisto J. Insulin resistance and hyperglycaemia in cardiovascular disease development[. J] Nat Rev Endocrinol. 2014;10:293–302.
Guerrero-Romero F, Simental-Mendía LE, González-Ortiz M, Martínez-Abundis E, Ramos-Zavala MG, Hernández-González SO, Jacques-Camarena O, Rodríguez-Morán M. The product of triglycerides and glucose, a simple measure of insulin sensitivity. Comparison with the euglycemic-hyperinsulinemic clamp.[J]. J Clin Endocrinol Metab. 2010;95:3347–51.
Liu X, Tan Z, Huang Y, Zhao H, Liu M, Yu P, Ma J, Zhao Y, Zhu W, Wang J. Relationship between the triglyceride-glucose index and risk of cardiovascular diseases and mortality in the general population: a systematic review and meta-analysis[. J] Cardiovasc Diabetol. 2022;21:124.
Won KB, Park EJ, Han D, Lee JH, Choi SY, Chun EJ, Park SH, Han HW, Sung J, Jung HO, Chang HJ. Triglyceride glucose index is an independent predictor for the progression of coronary artery calcification in the absence of heavy coronary artery calcification at baseline.[J].Cardiovasc Diabetol. 2020; 19:34.
Park K, Ahn CW, Lee SB, Kang S, Nam JS, Lee BK, Kim JH, Park JS. Elevated TyG Index Predicts Progression Coron Artery Calcification [J] Diabetes Care. 2019;42:1569–73.
Gao JW, Hao QY, Gao M, Zhang K, Li XZ, Wang JF, Vuitton DA, Zhang SL, Liu PM. Triglyceride-glucose index in the development of peripheral artery disease: findings from the atherosclerosis risk in communities (ARIC) Study.[J].Cardiovasc Diabetol. 2021; 20:126.
Yang Y, Huang X, Wang Y, Leng L, Xu J, Feng L, Jiang S, Wang J, Yang Y, Pan G, Jiang B, Wang Y, Chen L. The impact of triglyceride-glucose index on ischemic stroke: a systematic review and meta-analysis.[J].Cardiovasc Diabetol. 2023; 22:2.
**ong S, Chen Q, Long Y, Su H, Luo Y, Liu H, Chen Y, Feng Q, Peng X, Jiang M, Yu X, Zhang Z, Cai L. Association of the triglyceride-glucose index with coronary artery disease complexity in patients with acute coronary syndrome.[J].Cardiovasc Diabetol. 2023; 22:56.
Zhang Y, Ding X, Hua B, Liu Q, Gao H, Chen H, Zhao XQ, Li W, Li H. High triglyceride-glucose index is associated with adverse cardiovascular outcomes in patients with acute myocardial infarction.[J]. Nutr Metab Cardiovasc Dis. 2020;30:2351–62.
Ikeno F, Brooks MM, Nakagawa K, Kim MK, Kaneda H, Mitsutake Y, Vlachos HA, Schwartz L, Frye RL, Kelsey SF, Waseda K, Hlatky MA. SYNTAX score and long-term outcomes: the BARI-2D trial.[J]. J Am Coll Cardiol. 2017;69:395–403.
Hara H, Shiomi H, van Klaveren D, Kent DM, Steyerberg EW, Garg S, Onuma Y, Kimura T, Serruys PW. External validation of the SYNTAX score II 2020.[J].J am Coll Cardiol. 2021; 78:1227–38.
Serruys PW, Onuma Y, Garg S, Sarno G, van den Brand M, Kappetein AP, Van Dyck N, Mack M, Holmes D, Feldman T, Morice MC, Colombo A, Bass E, Leadley K, Dawkins KD, van Es GA, Morel MA, Mohr FW. Assessment of the SYNTAX score in the Syntax study.[J].EuroIntervention. 2009; 5:50–6.
Byrne RA, Rossello X, Coughlan JJ, Barbato E, Berry C, Chieffo A, Claeys MJ, Dan GA, Dweck MR, Galbraith M, Gilard M, Hinterbuchner L, Jankowska EA, Jüni P, Kimura T, Kunadian V, Leosdottir M, Lorusso R, Pedretti RFE, Rigopoulos AG, Rubini Gimenez M, Thiele H, Vranckx P, Wassmann S, Wenger NK, Ibanez B. 2023 ESC guidelines for the management of acute coronary syndromes[. J] Eur Heart J. 2023;44:3720–826.
ElSayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D, Collins BS, Hilliard ME, Isaacs D, Johnson EL, Kahan S, Khunti K, Leon J, Lyons SK, Perry ML, Prahalad P, Pratley RE, Seley JJ, Stanton RC, Gabbay RA. on behalf of the American Diabetes A. 2. Classification and Diagnosis of Diabetes: Standards of Care in Diabetes-2023.[J].Diabetes Care. 2023; 46:S19-s40.
Mancia G, Kreutz R, Brunström M, Burnier M, Grassi G, Januszewicz A, Muiesan ML, Tsioufis K, Agabiti-Rosei E, Algharably EAE, Azizi M, Benetos A, Borghi C, Hitij JB, Cifkova R, Coca A, Cornelissen V, Cruickshank JK, Cunha PG, Danser AHJ, Pinho RM, Delles C, Dominiczak AF, Dorobantu M, Doumas M, Fernández-Alfonso MS, Halimi JM, Járai Z, Jelaković B, Jordan J, Kuznetsova T, Laurent S, Lovic D, Lurbe E, Mahfoud F, Manolis A, Miglinas M, Narkiewicz K, Niiranen T, Palatini P, Parati G, Pathak A, Persu A, Polonia J, Redon J, Sarafidis P, Schmieder R, Spronck B, Stabouli S, Stergiou G, Taddei S, Thomopoulos C, Tomaszewski M, Van de Borne P, Wanner C, Weber T, Williams B, Zhang ZY, Kjeldsen SE. 2023 ESH guidelines for the management of arterial hypertension the Task Force for the management of arterial hypertension of the European Society of Hypertension: endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA).[J].J Hypertens. 2023; 41:1874–2071.
VanderWeele TJ. J] Epidemiol. 2011;22:582–5. Causal mediation analysis with survival data.[.
Liang CP, Han S, Senokuchi T, Tall AR. The macrophage at the crossroads of insulin resistance and atherosclerosis[. J] Circ Res. 2007;100:1546–55.
Sasso FC, Carbonara O, Nasti R, Campana B, Marfella R, Torella M, Nappi G, Torella R, Cozzolino D. Glucose metabolism and coronary heart disease in patients with normal glucose tolerance[. J] Jama. 2004;291:1857–63.
Sasso FC, Pafundi PC, Marfella R, Calabrò P, Piscione F, Furbatto F, Esposito G, Galiero R, Gragnano F, Rinaldi L, Salvatore T, D’Amico M, Adinolfi LE, Sardu C. Adiponectin and insulin resistance are related to restenosis and overall new PCI in subjects with normal glucose tolerance: the prospective AIRE Study.[J].Cardiovasc Diabetol. 2019; 18:24.
DeFronzo RA. Pathogenesis of type 2 diabetes mellitus[. J] Med Clin North Am. 2004;88:787–835. ix.
Muzurović E, Mikhailidis DP, Mantzoros C. Non-alcoholic fatty liver disease, insulin resistance, metabolic syndrome and their association with vascular risk.[J].Metabolism. 2021; 119:154770.
Zhu Y, Liu K, Chen M, Liu Y, Gao A, Hu C, Li H, Zhu H, Han H, Zhang J, Zhao Y. Triglyceride-glucose index is associated with in-stent restenosis in patients with acute coronary syndrome after percutaneous coronary intervention with drug-eluting stents. [J] Cardiovasc Diabetol. 2021;20:137.
Chen Q, **ong S, Zhang Z, Yu X, Chen Y, Ye T, Yang S, Qi L, Chen X, Liu H, Zheng J, Cai L. Triglyceride-glucose index is associated with recurrent revascularization in patients with type 2 diabetes mellitus after percutaneous coronary intervention.[J].Cardiovasc Diabetol. 2023; 22:284.
Liang S, Wang C, Zhang J, Liu Z, Bai Y, Chen Z, Huang H, He Y. Triglyceride-glucose index and coronary artery disease: a systematic review and meta-analysis of risk, severity, and prognosis.[J].Cardiovasc Diabetol. 2023; 22:170.
Cui C, Liu L, Zhang T, Fang L, Mo Z, Qi Y, Zheng J, Wang Z, Xu H, Yan H, Yue S, Wang X, Wu Z. Triglyceride-glucose index, renal function and cardiovascular disease: a national cohort study.[J].Cardiovasc Diabetol. 2023; 22:325.
Yang T, Li G, Wang C, Xu G, Li Q, Yang Y, Zhu L, Chen L, Li X, Yang H. Insulin resistance and coronary inflammation in patients with coronary artery disease: a cross-sectional study. [J] Cardiovasc Diabetol. 2024;23:79.
Wang X, Xu W, Song Q, Zhao Z, Meng X, **a C, **e Y, Yang C, ** P, Wang F. Association between the triglyceride-glucose index and severity of coronary artery disease[. J] Cardiovasc Diabetol. 2022;21:168.
Valenzuela PL, Carrera-Bastos P, Gálvez BG, Ruiz-Hurtado G, Ordovas JM, Ruilope LM, Lucia A. Lifestyle interventions for the prevention and treatment of hypertension[. J] Nat Rev Cardiol. 2021;18:251–75.
Campbell JM, Bellman SM, Stephenson MD, Lisy K. Metformin reduces all-cause mortality and diseases of ageing independent of its effect on diabetes control: a systematic review and meta-analysis[. J] Ageing Res Rev. 2017;40:31–44.
Sardu C, D’Onofrio N, Torella M, Portoghese M, Mureddu S, Loreni F, Ferraraccio F, Panarese I, Trotta MC, Gatta G, Galdiero M, Sasso FC, D’Amico M, De Feo M, Balestrieri ML, Paolisso G, Marfella R. Metformin Therapy effects on the expression of sodium-glucose cotransporter 2, leptin, and SIRT6 levels in Pericoronary Fat excised from pre-diabetic patients with Acute myocardial infarction.[J].Biomedicines. 2021; 9.
Sattar N, Lee MMY, Kristensen SL, Branch KRH, Del Prato S, Khurmi NS, Lam CSP, Lopes RD, McMurray JJV, Pratley RE, Rosenstock J, Gerstein HC. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of randomised trials.[J]. Lancet Diabetes Endocrinol. 2021;9:653–62.
Palmer SC, Tendal B, Mustafa RA, Vandvik PO, Li S, Hao Q, Tunnicliffe D, Ruospo M, Natale P, Saglimbene V, Nicolucci A, Johnson DW, Tonelli M, Rossi MC, Badve SV, Cho Y, Nadeau-Fredette AC, Burke M, Faruque LI, Lloyd A, Ahmad N, Liu Y, Tiv S, Millard T, Gagliardi L, Kolanu N, Barmanray RD, McMorrow R, Raygoza Cortez AK, White H, Chen X, Zhou X, Liu J, Rodríguez AF, González-Colmenero AD, Wang Y, Li L, Sutanto S, Solis RC, Díaz González-Colmenero F, Rodriguez-Gutierrez R, Walsh M, Guyatt G, Strippoli GFM. Sodium-glucose cotransporter protein-2 (SGLT-2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists for type 2 diabetes: systematic review and network meta-analysis of randomised controlled trials.[J].Bmj. 2021; 372:m4573.
Scheen AJ. Cardiovascular effects of new oral glucose-lowering agents: DPP-4 and SGLT-2. Inhibitors [J] Circ Res. 2018;122:1439–59.
Sasso FC, Carbonara O, Cozzolino D, Rambaldi P, Mansi L, Torella D, Gentile S, Turco S, Torella R, Salvatore T. Effects of insulin-glucose infusion on left ventricular function at rest and during dynamic exercise in healthy subjects and noninsulin dependent diabetic patients: a radionuclide ventriculographic study[. J] J Am Coll Cardiol. 2000;36:219–26.
Acknowledgements
The authors would like to thank all the participants.
Funding
This work was supported by National High Level Hospital Clinical Research Funding (2022-NHLHCRF-YSPY-01), Chinese Society of Cardiology’s Foundation (No. CSCF2021B02), and Chengdu High-level Key Clinical Specialty Construction Project.
Author information
Authors and Affiliations
Contributions
QC, SX, and TY drafted the manuscript, and were major contributors in the collection, analysis and interpretation of data. YG, JW, XL, YL, CC, HL, and ZZ were major contributors in the acquisition and interpretation of data and contributed to revision of the manuscript. LC and JZ designed the study and provided constructive suggestions for revisions of the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by the ethics committee of the Third People’s Hospital of Chengdu and strictly complied with the Declaration of Helsinki.
Consent for publication
All participants provided written/oral informed consent for publication.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chen, Q., **ong, S., Ye, T. et al. Insulin resistance, coronary artery lesion complexity and adverse cardiovascular outcomes in patients with acute coronary syndrome. Cardiovasc Diabetol 23, 172 (2024). https://doi.org/10.1186/s12933-024-02276-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-024-02276-1