
Abstract
Background
To analyse the causal associations of different physical measures with osteoarthritis knee (KOA).
Methods
Exposure factors (weight, body mass index (BMI), body fat percentage, waist circumference, hip circumference, waist–hip ratio (WHR), and basal metabolic rate (BMR)), and outcome factor KOA were analyzed by inverse-variance weighted (IVW) method, along with heterogeneity test, sensitivity and pleiotropy analyses. Meta-analysis was used to combine the effect values of IVW methods in different data sources.
Results
Weight, BMI, body fat percentage, waist circumference, hip circumference and BMR analyses showed causal association with increased KOA risk, while WHR analysis indicated a reduction of the incidence of KOA. P-value for all the results was less than 0.05 and F-value large than 20. All results were negative for heterogeneity tests and sensitivity analyses, and there was pleiotropy in weight and BMR. Meta-analysis results showed that the results of Odds Ratios (95% Confidence Intervals) for Weight (1.43(1.35–1.51)), BMI (1.40(1.10–1.78)), body fat percentage (1.56(1.44–1.68)), waist circumference (1.40(1.10–1.78)), hip circumference (1.37(1.30–1.44)), WHR (0.86(0.71–1.04)) and BMR (1.36(1.27–1.46) were consistent with the ones by Mendelian randomization analyses.
Conclusions
Body fat percentage may be a better indicator of KOA than BMI. In addition, weight and BMR may have a causal effect in KOA, but WHR does not have a causal relationship. BMI, body fat percentage, waist circumference, and hip circumference has a causal effect on KOA.
Similar content being viewed by others

Background
Osteoarthritis knee (KOA) is a chronic arthritic disease characterized by degenerative lesions and osteophytes in the knee cartilage [1, 2]. Clinical manifestations include pain, restricted motion, joint deformity, and bone friction sounds [3, 4]. With the population aging, the incidence of KOA is anticipated to rise from 13.8 to 15.7% by 2032, placing a huge burden on families and society [5, 6].
Several risk factors have been established to be caused with KOA, including age, gender, previous knee injury, occupational performance, and overweight or obesity. Overweight or obesity has been found to have a temporal causal association with the development and progression of KOA in early cohort studies [7,8,9]. Overweight or obesity is measured in various ways, such as body mass index (BMI), body fat percentage, waist circumference, hip circumference, waist–hip ratio (WHR), and basal metabolic rate (BMR). Although previous studies have found that all these indicators are risk factors for KOA, their causal relationship is not yet clear [10,11,12].
Mendelian randomization (MR) is a causal inference approach that uses genetic variation as an instrumental variable (IV); it is based on the principle of using the random division and combination of gametes during sexual reproduction to simulate the random assignment process to the subject of the study [13, 14]. Katan was the first to formulate a MR method for exploring the direct increase in cancer risk cause with low serum cholesterol levels [15]. In recent years, it has been widely used in the study of causal associations in a variety of diseases [16,17,18]. MR uses IVs, usually single nucleotide polymorphisms (SNPs), which are reliably caused with exposure and do not vary with caused lifestyle or socio-economic factors, and have the potential to confound traditional observational associations [19, 20]. Therefore, our study used MR to explore the causal relationship between weight, BMI, body fat percentage, waist circumference, hip circumference, WHR, and BMR in KOA. Data from multiple datasets for the same indicator were combined using meta-analysis. Through exploring the causal association between body composition measurements and KOA, it can help to make relevant interventions in the clinic to effectively prevent the development of KOA, and to make the patients with KOA have better regression.
Methods
Study design
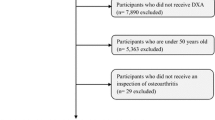
This study used MR to explore the causal relationship between weight, BMI, body fat percentage, body fat percentage, waist circumference, hip circumference, WHR, and BMR in KOA. Three assumptions need to be met in order to minimise bias due to unobserved confounding, measurement error, and reverse causality. They are (1) relevance, where the IV is strongly correlated with the exposure factor; (2) independence, whereby the IV is not correlated with the confounding factor; and (3) exclusion restriction, there is no causal association between the instrument variable and outcome independent of the exposure [21]. An overview of the study design is shown in Fig. 1. This study is reported following the STROBE-MR guidelines.

Overview of the design of this Mendelian randomization (MR) study on body composition measurements and osteoarthritis knee
Data sources
All analysed data are available in the IEU OpenGWAS project for this study (https://gwas.mrcieu.ac.uk/). Exposure factors were body composition measurements, including weight, BMI, body fat percentage, waist circumference, hip circumference, WHR, and BMR. The principle of selection was that the same exposure factor was selected, systematic and comprehensive search for datasets on body composition measurements, with a screening process that: (1) has a clear data source (e.g., GIANT, MRC-IEU, Neale Lab, Within family GWAS, etc.); and (2) uses the most recent year of data for the same data source. SNPs were from individuals of European origin, including both males and females. The KOA outcome factor was derived from 29 999 696 SNPs obtained from 403 124 European populations, which were sequenced by Tachmazidou et al. and published in the UK Biobank consortium [22]. Detailed information is shown in Table 1.
Genetic instrument selection
To avoid strong linkage disequilibrium between SNPs, then genome-wide significant SNPs with independent and highly correlated exposure factors, as well as outcome variables were selected as IVs. The genome-wide information from the Thousand Genomes Project was used as a reference to screen for IVs without linkage effects [23]: (1) the parameters of weight, BMI, body fat percentage, waist circumference, hip circumference, WHR, and BMR datasets with genome-wide significance were set to P < 5 × 10− 8; (2) the linkage disequilibrium parameter (r2) was set to 0.001; and (3) the genetic distance was set to 10 MB, to screen for IVs without linkage effects. Then, IVs that were apparently caused with KOA were excluded from the screened IVs (P < 0.05). At the same time, the data were pre-processed so as to ensure consistency in effects equivalence and effect sizes. Finally, the strength of causal association of the genetic instruments for each putative risk factor was quantified by the F statistic (F = β2/se2) for all SNPs, to assess the power of the SNPs, If the F-statistic is much greater than 10, the likelihood of weak IV bias is small [30, 35]. Our study further demonstrated a causal relationship between waist circumference, hip circumference, and KOA in different datasets. However, the results of WHR in both datasets suggested that there was no causal relationship with KOA. In the previous studies, the findings on WHR were inconsistent. Holliday et al. found that WHR was not caused with KOA [35], but Lohmander et al. found an RR (risk ratio) of 2.2 for WHR [36]. On the other hand, Gandhi et al. found the RR of being obese [10], as determined by WHR if classified as obese by the BMI criteria, was 1.04 for men and 1.23 for women, suggesting that the causal relationship between WHR and KOA might be influenced by gender factors and requires further study.
In the two datasets for BMR analysis, the Neale Lab consortium’s dataset was found to have a statistically significant pleiotropic analysis, and the MRC-IEU consortium’s dataset suggested a causal relationship between BMR and KOA, with a combined OR of 1.36 (1.27–1.46). Therefore, BMR might have a causal effect in KOA. However, BMR was influenced by a number of factors, such as body surface area, growth stage, gender, nutrition, and functional status, thus was expected further analysis.
There were some limitations should be mentioned in this study. The sources of datasets for different physical measures were inconsistent, with four datasets present for some indicators and two datasets for others, which might have impacted the results. The discrepancy in findings due to gender differences evident in previous studies of the WHR, and failing to analyse gender separately, might also be insufficient in other measures. The datasets were all from European populations, so the findings may be applicable only in European populations and be of limited use for other populations. MR assumed a linear relationship between exposure factors and outcome factors, and did not apply if there was no linear relationship between the two.
Conclusion
In summary, our study used MR to explore the causal relationships between weight, BMI, body fat percentage, waist circumference, hip circumference, WHR, and BMR in KOA. Additionally, we used meta-analysis to combine the results of different datasets and to enhance the strength of their causal associations. We found that weight and BMR might have a causal effect on KOA, but WHR did not. BMI, body fat percentage, waist circumference, and hip circumference had a causal relationship with KOA. Additionally, body fat percentage might be a better indicator of KOA than BMI.
Data availability
The data used in this study were publicly available. Weight: (dataset: ukb-b-11842, MRC-IEU, https://gwas.mrcieu.ac.uk/datasets/ukb-b-11842/; dataset: ukb-a-249, Neale Lab, https://gwas.mrcieu.ac.uk/datasets/ukb-a-249/); Body Mass Index: (dataset: ieu-b-40, GIANT, https://gwas.mrcieu.ac.uk/datasets/ieu-b-40/; dataset: ukb-b-19953, MRC-IEU, https://gwas.mrcieu.ac.uk/datasets/ukb-b-19953/; dataset: ukb-a-248, Neale Lab, https://gwas.mrcieu.ac.uk/datasets/ukb-a-248/; dataset: ieu-b-4816, Within family GWAS, https://gwas.mrcieu.ac.uk/datasets/ieu-b-4816/); Body Fat Percentage: (dataset: ukb-b-8909, MRC-IEU, https://gwas.mrcieu.ac.uk/datasets/ukb-b-8909/; dataset: ukb-a-264, Neale Lab, https://gwas.mrcieu.ac.uk/datasets/ukb-a-264/); Waist Circumference: (dataset: ukb-b-9405, MRC-IEU, https://gwas.mrcieu.ac.uk/datasets/ukb-b-9405/; dataset: ukb-a-382, Neale Lab, https://gwas.mrcieu.ac.uk/datasets/ukb-a-382/; dataset: ieu-a-61, GIANT, https://gwas.mrcieu.ac.uk/datasets/ieu-a-61/); Hip Circumference: (dataset: ukb-b-15590, MRC-IEU, https://gwas.mrcieu.ac.uk/datasets/ukb-b-15590/; dataset: ukb-a-388, Neale Lab, https://gwas.mrcieu.ac.uk/datasets/ukb-a-388/; dataset: ieu-a-49, GIANT, https://gwas.mrcieu.ac.uk/datasets/ieu-a-49/); Waist-Hip Ratio: (dataset: ieu-a-73, GIANT, https://gwas.mrcieu.ac.uk/datasets/ieu-a-73/; dataset: ieu-b-4830, Within family GWAS, https://gwas.mrcieu.ac.uk/datasets/ieu-b-4830/); Basal Metabolic Rate: (dataset: ukb-b-16446, MRC-IEU, https://gwas.mrcieu.ac.uk/datasets/ukb-b-16446/; dataset: ukb-a-268, Neale Lab, https://gwas.mrcieu.ac.uk/datasets/ukb-a-268/); Knee Osteoarthritis: (dataset: ebi-a-GCST007090 UK, Biobank, https://gwas.mrcieu.ac.uk/datasets/ebi-a-GCST007090/)
Abbreviations
- KOA:
-
Osteoarthritis Knee
- BMI:
-
Body Mass Index
- WHR:
-
Waist Hip Ratio
- BMR:
-
Basal Metabolic Rate
- IVW:
-
Inverse Variance Weighted
- MR:
-
Mendelian Randomization
- IV:
-
Instrumental Variable
- SNPs:
-
Single Nucleotide Polymorphisms
- OR:
-
Odds Ratio
- CI:
-
Confidence Interval
References
Brophy RH, Fillingham YA, AAOS Clinical Practice Guideline Summary. Management of Osteoarthritis of the knee (nonarthroplasty), Third Edition. J Am Acad Orthop Surg. 2022;30(9):e721–9.
Giorgino R, Albano D, Fusco S, Peretti GM, Mangiavini L, Messina C. Knee osteoarthritis: Epidemiology, Pathogenesis, and mesenchymal stem cells: what else is New? An update. Int J Mol Sci 2023; 24(7).
Georgiev T, Angelov AK. Modifiable risk factors in knee osteoarthritis: treatment implications. Rheumatol Int. 2019;39(7):1145–57.
Ma XL, Hu YC, Wang KZ. Chinese clinical practice guidelines in treating knee osteoarthritis by Periarticular Knee Osteotomy. Orthop Surg. 2022;14(5):789–806.
Safiri S, Kolahi AA, Smith E, Hill C, Bettampadi D, Mansournia MA, Hoy D, Ashrafi-Asgarabad A, Sepidarkish M, Almasi-Hashiani A, et al. Global, regional and national burden of osteoarthritis 1990–2017: a systematic analysis of the global burden of Disease Study 2017. Ann Rheum Dis. 2020;79(6):819–28.
Turkiewicz A, Petersson IF, Björk J, Hawker G, Dahlberg LE, Lohmander LS, Englund M. Current and future impact of osteoarthritis on health care: a population-based study with projections to year 2032. Osteoarthritis Cartilage. 2014;22(11):1826–32.
Kulkarni K, Karssiens T, Kumar V, Pandit H. Obesity and osteoarthritis. Maturitas. 2016;89:22–8.
Reyes C, Leyland KM, Peat G, Cooper C, Arden NK, Prieto-Alhambra D. Association between Overweight and Obesity and risk of clinically diagnosed knee, hip, and Hand Osteoarthritis: a Population-based Cohort Study. Arthritis Rheumatol. 2016;68(8):1869–75.
Wills AK, Black S, Cooper R, Coppack RJ, Hardy R, Martin KR, Cooper C, Kuh D. Life course body mass index and risk of knee osteoarthritis at the age of 53 years: evidence from the 1946 British birth cohort study. Ann Rheum Dis. 2012;71(5):655–60.
Gandhi R, Dhotar H, Tsvetkov D, Mahomed NN. The relation between body mass index and waist-hip ratio in knee osteoarthritis. Can J Surg. 2010;53(3):151–4.
Gill SV, Hicks GE, Zhang Y, Niu J, Apovian CM, White DK. The association of waist circumference with walking difficulty among adults with or at risk of knee osteoarthritis: the Osteoarthritis Initiative. Osteoarthritis Cartilage. 2017;25(1):60–6.
Zhang W, Doherty M, Peat G, Bierma-Zeinstra MA, Arden NK, Bresnihan B, Herrero-Beaumont G, Kirschner S, Leeb BF, Lohmander LS, et al. EULAR evidence-based recommendations for the diagnosis of knee osteoarthritis. Ann Rheum Dis. 2010;69(3):483–9.
Sekula P, Del GMF, Pattaro C, Köttgen A. Mendelian randomization as an Approach to assess causality using Observational Data. J Am Soc Nephrol. 2016;27(11):3253–65.
Skrivankova VW, Richmond RC, Woolf B, Yarmolinsky J, Davies NM, Swanson SA, Vanderweele TJ, Higgins J, Timpson NJ, Dimou N, et al. Strengthening the reporting of Observational studies in Epidemiology using mendelian randomization: the STROBE-MR Statement. JAMA. 2021;326(16):1614–21.
Katan MB. Apolipoprotein E isoforms, serum cholesterol, and cancer. Lancet. 1986;1(8479):507–8.
van Oort S, Beulens J, van Ballegooijen AJ, Grobbee DE, Larsson SC. Association of Cardiovascular Risk factors and lifestyle behaviors with hypertension: a mendelian randomization study. Hypertension. 2020;76(6):1971–9.
Yuan S, Larsson SC. Assessing causal associations of obesity and diabetes with kidney stones using mendelian randomization analysis. Mol Genet Metab. 2021;134(1–2):212–5.
Zhang Z, Wang M, Yuan S, Liu X. Alcohol, Coffee, and milk intake in relation to Epilepsy Risk. Nutrients. 2022; 14(6).
Davies NM, Holmes MV, Davey SG. Reading mendelian randomisation studies: a guide, glossary, and checklist for clinicians. BMJ. 2018;362:k601.
Gupta V, Walia GK, Sachdeva MP. Mendelian randomization’: an approach for exploring causal relations in epidemiology. Public Health. 2017;145:113–9.
Boef AG, Dekkers OM, le Cessie S. Mendelian randomization studies: a review of the approaches used and the quality of reporting. Int J Epidemiol. 2015;44(2):496–511.
Tachmazidou I, Hatzikotoulas K, Southam L, Esparza-Gordillo J, Haberland V, Zheng J, Johnson T, Koprulu M, Zengini E, Steinberg J, et al. Identification of new therapeutic targets for osteoarthritis through genome-wide analyses of UK Biobank data. Nat Genet. 2019;51(2):230–6.
Funck-Brentano T, Nethander M, Movérare-Skrtic S, Richette P, Ohlsson C. Causal factors for knee, hip, and Hand Osteoarthritis: a mendelian randomization study in the UK Biobank. Arthritis Rheumatol. 2019;71(10):1634–41.
**e J, Huang H, Liu Z, Li Y, Yu C, Xu L, Xu C. The associations between modifiable risk factors and nonalcoholic fatty liver disease: a comprehensive mendelian randomization study. Hepatology. 2023;77(3):949–64.
Neogi T, Zhang Y. Epidemiology of osteoarthritis. Rheum Dis Clin North Am. 2013;39(1):1–19.
Pradelli L, Sinigaglia T, Migliore A, Checchia GA, Franceschi F, Frediani B, Iannone F, Romanini E. Non-surgical treatment of knee osteoarthritis: Multidisciplinary Italian Consensus on best practice. Ther Clin Risk Manag. 2021;17:507–30.
Sun X, Zhen X, Hu X, Li Y, Gu S, Gu Y, Dong H. Osteoarthritis in the Middle-aged and Elderly in China: prevalence and influencing factors. Int J Environ Res Public Health. 2019; 16(23).
Zheng H, Chen C. Body mass index and risk of knee osteoarthritis: systematic review and meta-analysis of prospective studies. Bmj Open. 2015;5(12):e7568.
Holmberg S, Thelin A, Thelin N. Knee osteoarthritis and body mass index: a population-based case-control study. Scand J Rheumatol. 2005;34(1):59–64.
Vasilic-Brasnjevic S, Marinkovic J, Vla**ac H, Vasiljevic N, Jakovljevic B, Nikic M, Maksimovic M. Association of body mass index and waist circumference with severity of knee osteoarthritis. Acta Reumatol Port. 2016;41(3):226–31.
Katz JN, Arant KR, Loeser RF. Diagnosis and treatment of hip and knee osteoarthritis: a review. JAMA. 2021;325(6):568–78.
Panunzi S, Maltese S, De Gaetano A, Capristo E, Bornstein SR, Mingrone G. Comparative efficacy of different weight loss treatments on knee osteoarthritis: a network meta-analysis. Obes Rev. 2021;22(8):e13230.
Long H, **e D, Zeng C, Wei J, Wang Y, Yang T, Xu B, Qian Y, Li J, Wu Z, et al. Association between body composition and osteoarthritis: a systematic review and meta-analysis. Int J Rheum Dis. 2019;22(12):2108–18.
Karlsson MK, Magnusson H, Cöster M, Karlsson C, Rosengren BE. Patients with knee osteoarthritis have a phenotype with higher bone mass, higher fat mass, and lower lean body mass. Clin Orthop Relat Res. 2015;473(1):258–64.
Holliday KL, Mcwilliams DF, Maciewicz RA, Muir KR, Zhang W, Doherty M. Lifetime body mass index, other anthropometric measures of obesity and risk of knee or hip osteoarthritis in the GOAL case-control study. Osteoarthritis Cartilage. 2011;19(1):37–43.
Lohmander LS, Gerhardsson DVM, Rollof J, Nilsson PM, Engström G. Incidence of severe knee and hip osteoarthritis in relation to different measures of body mass: a population-based prospective cohort study. Ann Rheum Dis. 2009;68(4):490–6.
Acknowledgements
We thank the MRC-IEU, Neale Lab, GIANT, within family GWAS, and UK Biobank consortiums for providing summary statistics data for the analyses.
Funding
This study was funded by Key Disciplines of Changshu (CSZDXK202303).
Author information
Authors and Affiliations
Contributions
B.P. and G.H. designed the study. D.Q., W.H. and K.W. analysed and interpreted the data. K.W., B.C. and M.X. revised the manuscript. The manuscript was drafted by G.H and W.H. with contributions from B.P. B.P. is the guarantor of this work. All authors revised the paper critically for intellectual content and approved the final version. All authors agree to be accountable for the work and to ensure that any questions relating to the accuracy and integrity of the paper are investigated and properly resolved.
Corresponding authors
Ethics declarations
Consent for publication
Not applicable.
Ethics approval and consent to participate
The source of the data was a publicly available database, and no human participants were involved; hence, ethical parameters are not applicable.
Competing interests
Guoxin Huang, Weimin Hong, Ke Wang, Ming Xu, Bingqian Chen, Da Qian, Bin Pei declared that they had no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Huang, G., Hong, W., Wang, K. et al. Causal analysis of body composition measurements in osteoarthritis knee: a two-sample mendelian randomization study. BMC Musculoskelet Disord 25, 341 (2024). https://doi.org/10.1186/s12891-024-07465-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-024-07465-3