
Abstract
Background
Many surgical options have been described to manage post-tubercular kyphosis, but the standard approach for treating severe post-tubercular angular kyphosis in children has not been established yet. The present study was performed to evaluate the safety and efficacy of deformed complex vertebral osteotomy (DCVO) for the treatment of severe thoracic post-tubercular angular kyphosis (> 70°) in children.
Methods
Deformed complex vertebrae indicated that multiple deformed and fused vertebrae were usually involved with two or more vertebral bodies and the partial or total fusion of many segments' facet joints and intervertebral discs. Thus, DCVO indicated that a wider posterior wedge-shaped and three-column osteotomy was performed within deformed complex vertebrae to correct a more extensive range of angles. From 2010 to 2017, 15 children who suffered from severe thoracic post-tubercular angular kyphosis underwent DCVO. Deformed complex vertebrae involved two vertebral bodies in 9 patients and three vertebral bodies in 6 patients. The Visual Analogue Scale (VAS) and Oswestry Disability Index (ODI) were assessed preoperatively and at the final follow up. This was a retrospective study analysing the outcome after grade 4/5 spinal osteotomies in deformed complex vertebrae.
Results
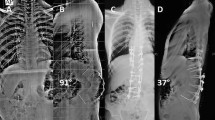
The mean duration of surgery was 239 ± 37.81 min. The average period of follow-up was 31.6 ± 6.98 months. The preoperative mean kyphosis of deformed complex vertebrae was 83.39° ± 9.04°; the mean thoracic kyphosis (TK) and lumbar lordosis (LL) were 81.09° ± 8.51° and 80.51° ± 7.64°, respectively; the mean sagittal vertical axis (SVA) was 3.83 cm ± 1.43 cm. The postoperative mean kyphosis of deformed complex vertebrae was reduced to 19.98° ± 2.47° (P < 0.001) with a mean kyphosis correction of 63.41°; at the final follow up, it was 18.4° ± 2.29° (P < 0.001) without obvious loss of correction. The postoperative mean TK, LL, and SVA were reduced to 24.05° ± 3.84°, 46.9° ± 3.53°, and 0.6 cm ± 0.34 cm, respectively (P < 0.001 for all); and there was no obvious loss of sagittal alignment and balance at the final follow up (p = 0.982, p = 0.604, p = 0.754). Complicated with neural dysfunction preoperatively, 5 Frankel's grade D cases showed complete neurological recovery at final follow up. VAS score reduced from 3.6 ± 1.18 to 0.87 ± 0.64 (P < 0.001); and ODI score reduced from 22.21 ± 6.93 to 5.02 ± 2.6 (P < 0.001) at the final follow up.
Conclusions
DCVO was an individualized osteotomy for treating severe thoracic post-tubercular angular kyphosis in children and could be safe and effective in reducing the incidence of complications and significantly improving kyphosis correction.
Similar content being viewed by others

Background
Spinal tuberculosis accounts for half the cases of osteo-articular tuberculosis. Vertebral inoculation occurs via the haematogenous route, and the process then spreads to the intervertebral disk and, in some cases, to the adjacent vertebra. Para-spinal abscesses may develop by direct spread from the vertebral lesion. The thoracic spine is predominantly involved [1]. The patients with spinal tuberculosis that were treated conservatively presented with kyphosis with an average of 15°, and eventually, 3–5% of them ended up with a kyphotic angle of more than 60° [2,3,4,5]. Furthermore, even if spinal tuberculosis heals during the period of growth and development of children, an imbalance in the spinal growth of the anterior and posterior columns could still aggravate kyphosis [6, 7]. Severe post-tubercular angular kyphosis generally affects children's self-confidence and appearance and could even lead to severe neurological impairment and cardiopulmonary dysfunction. Many surgical options have been described to manage post-tubercular angular kyphosis, but the standard approach has not yet been established.
Until now, surgical osteotomy has been the leading choice for correcting the deformity and realigning the spine. Posterior column osteotomy (PCO) is not indicated as a first-line treatment for post-tubercular angular kyphosis because of the difficulty in decompressing the spine canal anteriorly and the relatively small correction angle [8,9,10]. Conversely, pedicle subtraction osteotomy (PSO) is a wedge-shaped resection in one vertebra which includes the partial vertebral body and posterior column elements and can only acquire correction of 30°-40° [9,10,11]. Vertebral column resection (VCR) requires removing one or several whole vertebrae, concurrently including adjacent discs and a portion of the ribs in the thoracic region, which could significantly correct severe kyphoscoliosis. However, VCR has several disadvantages, such as neurological complications, blood loss, operation time, nonunion or pseudoarthrosis, and a significant increase in the incidence of postoperative complications [12,13,14,15]. Therefore, the present study was performed to evaluate the safety and efficacy of modified posterior wedge osteotomy within deformed complex vertebrae to treat severe thoracic post-tubercular angular kyphosis (> 70°) in children. This was a retrospective study analysing the outcome after grade 4/5 spinal osteotomies.
Materials and methods
Patient data
In this study, we retrospectively evaluate the clinical efficacy of 15 children (8 boys and 7 girls; age, 5–11 years; average age, 7.8 ± 2.0 years) that suffered from severe thoracic post-tubercular angular kyphosis and were treated in our department between 2010 to 2017. In all children, X-ray, CT, and MRI examinations revealed: deformed complex vertebrae involved with two vertebral bodies in 9 patients and three vertebral bodies in 6 patients; the lesions healed completely in all 15 cases without further destruction of the vertebral bodies or abscesses.
All cases presented with apparent kyphotic deformity and persistent back pain, and some of them incurred incomplete paralysis. C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) in all cases were normal. The Frankel scoring system was used to assess neurological function. Frankel's grade D was in 5 patients, and Grade E in 10 patients. The Ethics Committee of ** the growth potentials of the anterior column and to reduce surgical trauma and intraoperative blood loss. The anterior longitudinal ligament served as a hinge for the bone-to-bone closure of the gap. In this group of cases, the nerve roots were not ligated and slightly affected the visibility of the operative field and the freedom of osteotomy. However, there was no direct damage to the nerve roots, and this helped preserve nervous system functional integrity.
After DCVO, the postoperative mean kyphosis was reduced to 19.98° with a kyphosis correction of 63.41°. The correction rate was considerably better than that of PSO and VCR reported by some authors [9, 10, 12, 14, 17, 18]. Patients' body figure, sagittal alignment and balance (TK, LL, and SVA), pain (VAS), daily activities (ODI), and neurological function (Frankel's grade) all showed good improvement. However, the operation time, blood loss, difficulty of operation, incidence of complications, and neurological events were significantly lower than those of VCR reported in previous studies [12, 14, 17, 19, 20].
Although conservative treatment is effective with the use of antituberculosis medication, however, it is well known that progressive collapse of anterior spinal elements may still occur under gravity and compression. Moreover, due to eccentric loads and spinal growth imbalance of anterior and posterior columns in children, the wedge shape of the vertebral body and kyphotic deformity could be aggravated. Neurological deterioration, cardiopulmonary dysfunction, and severe persistent back pain are all possible side effects of post-tubercular kyphosis [2, 21, 22]. As a result, children with severe thoracic post-tubercular angular kyphosis frequently require surgery.
The primary goal of surgery is to treat spinal deformity and prevent further deformity, as well as to restore and reconstruct the physiological sagittal alignment and decompress the nerve to improve its function. To date, numerous techniques have been developed to treat kyphosis secondary to spinal tuberculosis, mainly including Smith-Petersen Osteotomy (SPO), PSO, and VCR [10, 14, 21, 23]. However, none of those mentioned above techniques was considered a golden criterion for attaining minor trauma and significant correction.
SPO could only achieve approximately 10.7° per segment of kyphosis correction. However, after opening the anterior column, it was determined that there was a risk of permanent neurological impairment and aortic rupture [10, 24]. In recent years, three-column osteotomy has been the primary technique for the treatment of severe angular kyphosis. Hu et al. [9] compared SPO and PSO in the treatment of rigid thoracolumbar kyphotic deformity, finding that PSO's kyphosis correction ranged from 31.7° to 48° with an average of 36.7°, while SPO's was 8.74° less. Furthermore, the incidence of biomechanical complications, including instrument breakage, anterior cortex fracture, pedicle screw loosening, pedicle fraction, vertebral body translation, and nonunion, in PSO was lower than in SPO [10, In conclusion, DCVO was an individualized osteotomy for treating severe thoracic post-tubercular angular kyphosis in children. It could be safe and effective in reducing the incidence of complications and significantly improving kyphosis correction.Conclusions
Availability of data and materials
The datasets analyzed during the current study are not publicly available because a further study about severe angular kyphosis is in progress in our institution, but are available from the corresponding author on reasonable request.
Abbreviations
- DCVO:
-
Deformed complex vertebral osteotomy
- SVA:
-
Sagittal vertical axis
- VAS:
-
Visual Analogue Scale
- ODI:
-
Oswestry Disability Index
- CT:
-
Computed tomography
- MRI:
-
Magnetic resonance imaging
- TK:
-
Thoracic kyphosis
- LL:
-
Lumbar lordosis
- MEP:
-
Motor evoked potential
- SEP:
-
Somatosensory evoked potential
- PCO:
-
Posterior column osteotomy
- SPO:
-
Smith-Petersen Osteotomy
- PSO:
-
Pedicle subtraction osteotomy
- VCR:
-
Vertebral column resection
- CRP:
-
C-reactive protein
- ESR:
-
Erythrocyte sedimentation rate
References
Ferrer MF, Torres LG, Ramírez OA, Zarzuelo MR, González NDP, Tuberculosis of the spine. A systematic review of case series. Int Orthop. 2012;36(2):221–31.
Rajasekaran S. Kyphotic deformity in spinal tuberculosis and its management. Int Orthop. 2012;36(2):359–65.
Wang YX, Zhang HQ, Tang MX, Guo CF, Deng A, Wu JH, Liu JY, Deng Z, Chen J. One-stage posterior focus debridement, interbody grafts, and posterior instrumentation and fusion in the surgical treatment of thoracolumbar spinal tuberculosis with kyphosis in children: a preliminary report. Childs Nerv Syst. 2016;32(8):1495–502.
Deng A, Zhang HQ, Tang MX, Liu SH, Gao QL, Wang YX, Guo CF, Wang XY. One-stage combined posterior and anterior approaches for active tuberculosis of the subaxial cervical spine complicated with kyphosis in children: a preliminary study. Int J Clin Exp Med. 2016;9(2):3953–9.
Zhang HQ, Li JS, Guo CF, Liu SH, Tang MX, Wang YX, Deng A, Le Gao Q, Lin MZ. Two-stage surgical management using posterior instrumentation, anterior debridement and allografting for tuberculosis of the lower lumbar spine in children of elementary school age: minimum 3-year follow-up of 14 patients. Arch Orthop Trauma Surg. 2012;132(9):1273–9.
Rajasekaran S, Prasad Shetty A, Dheenadhayalan J, Shashidhar Reddy J, Naresh-Babu J, Kishen T. Morphological changes during growth in healed childhood spinal tuberculosis: a 15-year prospective study of 61 children treated with ambulatory chemotherapy. J Pediatr Orthop. 2006;26(6):716–24.
Moon MS, Kim SS, Lee BJ, Moon JL. Spinal tuberculosis in children: retrospective analysis of 124 patients. Indian J Orthop. 2012;46(2):150–8.
Rathod TN, Shah KA. Vertebral column resection for post tuberculosis severe kyphotic deformity: results of 5 year follow-up. J Orthop. 2019;19:122–7.
Hu XM, Thapa AJ, Cai ZP, Wang P, Huang L, Tang Y, Ye JC, Cheng K, Shen HY. Comparison of smith-petersen osteotomy, pedicular subtraction osteotomy, and poly-segmental wedge osteotomy in treating rigid thoracolumbar kyphotic deformity in ankylosing spondylitis a systematic review and meta-analysis. BMC Surg. 2016;16:4.
Cho KJ, Bridwell KH, Lenke LG, Berra A, Baldus C. Comparison of Smith-Petersen versus pedicle subtraction osteotomy for the correction of fixed sagittal imbalance. Spine. 2005;30(18):2030–7.
Park JS, Kim J, Joo IH, Sim KD, Park YS. Analysis of risk factors for sagittal translation after pedicle subtraction osteotomy in patients with ankylosing spondylitis. Spine J. 2018;18(8):1356–62.
Yang C, Zheng Z, Liu H, Wang J, Kim YJ, Cho S. Posterior vertebral column resection in spinal deformity: a systematic review. Eur Spine J. 2016;25(8):2368–75.
Schwab F, Blondel B, Chay E, Demakakos J, Lenke L, Tropiano P, Ames C, Smith JS, Shaffrey CI, Glassman S, Farcy JP, Lafage V. The comprehensive anatomical spinal osteotomy classification. Neurosurgery. 2014;74(1):112–20.
Lenke LG, Newton PO, Sucato DJ, Shufflebarger HL, Emans JB, Sponseller PD, Shah SA, Sides BA, Blanke KM. Complications after 147 consecutive vertebral column resections for severe pediatric spinal deformity: a multicenter analysis. Spine. 2013;38(2):119–32.
Riley MS, Lenke LG, Chapman TM Jr, Sides BA, Blanke KM, Kelly MP. Clinical and radiographic outcomes after posterior vertebral column resection for severe spinal deformity with five-year follow-up. J Bone Joint Surg Am. 2018;100(5):396–405.
Zhang HQ, **ao LG, Guo CF, Wang YX, Wu JH, Liu JY. Deformed complex vertebral osteotomy technique for management of severe congenital spinal angular kyphotic deformity. Orthop Surg. 2021;13(3):1016–25.
Suk SI, Kim JH, Kim WJ, Lee SM, Chung ER, Nah KH. Posterior vertebral column resection for severe spinal deformities. Spine. 2002;27(21):2374–82.
Kalra KP, Dhar SB, Shetty G, Dhariwal Q. Pedicle subtraction osteotomy for rigid post-tuberculous kyphosis. J Bone Joint Surg Br. 2006;88(7):925–7.
Zhang HQ, Li JS, Liu SH, Guo CF, Tang MX, Gao QL, Lin MZ, Yin XH, Wang YX, Deng A. The use of posterior vertebral column resection in the management of severe posttuberculous kyphosis: a retrospective study and literature review. Arch Orthop Trauma Surg. 2013;133(9):1211–8.
Hua W, Wu X, Zhang Y, Gao Y, Li S, Wang K, Liu X, Yang S, Yang C. Incidence and risk factors of neurological complications during posterior vertebral column resection to correct severe post-tubercular kyphosis with late-onset neurological deficits: case series and review of the literature. J Orthop Surg Res. 2018;13:269.
Bezer M, Kucukdurmaz F, Guven O. Transpedicular decancellation osteotomy in the treatment of posttuberculous kyphosis. J Spinal Disord Tech. 2007;20(3):209–15.
Pappou IP1, Papadopoulos EC, Swanson AN, Mermer MJ, Fantini GA, Urban MK, Russell L, Cammisa FP Jr, Girardi FP. Pott disease in the thoracolumbar spine with marked kyphosis and progressive paraplegia necessitating posterior vertebral column resection and anterior reconstruction with a cage. Spine. 2006;31(4):E123-127.
Issack PS, Boachie-Adjei O. Surgical correction of kyphotic deformity in spinal tuberculosis. Int Orthop. 2012;36(2):353–7.
Liu H, Yang C, Zheng Z, Ding W, Wang J, Wang H, Li S. Comparison of Smith-Petersen osteotomy and pedicle subtraction osteotomy for the correction of thoracolumbar kyphotic deformity in ankylosing spondylitis: a systematic review and meta-analysis. Spine. 2015;40(8):570–9.
Hong-Qi Z, Yong C, Jia H, Chaofeng G, **ongke H. Modified pedicle subtraction osteotomies (mPSO) for thoracolumbar post-tubercular kyphosis in pediatric patients: retrospective clinical cases and review of the literature. Childs Nerv Syst. 2015;31(8):1347–54.
Yang BP, Ondra SL, Chen LA, Jung HS, Koski TR, Salehi SA. Clinical and radiographic outcomes of thoracic and lumbar pedicle subtraction osteotomy for fixed sagittal imbalance. J Neurosurg Spine. 2006;5(1):9–17.
Acknowledgements
Not applicable.
Funding
The study was supported by the Natural Science Foundation of Hunan Province, China (NO. 2020JJ4873). The funding bodies had no role in the design of the study or in collection, analysis, interpretation or presentation of data.
Author information
Authors and Affiliations
Contributions
HQZ was involved in critical revision of the manuscript, statistical expertise and performing most of the analyses presented in the paper. AD was involved in study design, data analysis and interpretation, writing the manuscript and critical revision of the manuscript. CFG was involved in data collection, preliminary data analysis and interpretation, critical revision of the manuscript and statistical expertise. QLG was involved in study conception and design, data analysis and interpretation, writing the manuscript, critical revision of the manuscript, supervision and administrative support. EA was involved in study conception and design, data collection, development of data collection instruments and critical revision of the manuscript. All authors approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Ethics Committee in **angya Hospital of Central South University approved the study. All methods were performed in accordance with the relevant guidelines and regulations. Written informed consent was acquired from each of the patients (or their parents and legal guardians) to authorize treatment, imageology findings, and photographic documentation. The patients (or their parents and legal guardians) consented to the publication of their pictures as well as their anonymous and clustered data.
Consent for publication
Written informed consent was acquired from each of the patients (or their parents and legal guardians) to authorize treatment, imageology findings, and photographic documentation. The patients (or their parents and legal guardians) consented to the publication of their pictures as well as their anonymous and clustered data.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, HQ., Deng, A., Guo, CF. et al. Retrospective analysis of deformed complex vertebral osteotomy in children with severe thoracic post-tubercular angular kyphosis. BMC Musculoskelet Disord 23, 805 (2022). https://doi.org/10.1186/s12891-022-05756-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-022-05756-1