
Abstract
Background
Although the COVID-19 pandemic and its implications have been associated with mental health services utilization and medication consumption, there is no longitudinal study on the long-term impact on ADHD medication use trends.
Methods
This study examines the European ADHD medication consumption in 2020 to 2022 compared to the predicted consumption assuming the persistence of pre-pandemic trends. Predictions are calculated using Seasonal Autoregressive Integrated Moving Average (SARIMA) models.
Results
While European ADHD medication sales recorded a drop in 2020, they returned to the predicted level in 2021, even slightly exceeding it. In 2022, we found a clear exceedance of the predicted level by 16.4% on average at country level. Furthermore, the increase in consumption growth in the post-pandemic period (2021–2022) compared to the pre-pandemic period (2014–2019) was significant in 26 of the 28 European countries under consideration.
Conclusion
There is strong evidence of a trend change in the ADHD medicine consumption growth throughout Europe after the COVID-19 pandemic.
Similar content being viewed by others

Background
A steady growth in the use of attention deficit hyperactivity disorder (ADHD) medications has been reported for the decades prior to the COVID-19 pandemic [5, 16, 23]. This was associated with an increase in the general awareness of ADHD among the public, practitioners, and psychotherapists alike. An important contributing factor was the broadening of the diagnostic criteria, e.g., the elimination of exclusion criteria such as autism spectrum disorder (ASD) in the DSM-5 released in 2013 [1]. Also, DSM-5 reduced the symptoms threshold for adults and the necessity of a childhood onset for an adult-ADHD diagnosis has become a matter of debate [4, 18]. The COVID-19 pandemic is associated with a break in this steady growth: We showed in a previous study that, globally, ADHD medicine consumption in 2020 was on average per country 6% lower than predicted based on pre-pandemic data [12]. However, several studies reported adverse effects of the pandemic on patients with ADHD in form of increased ADHD symptoms [6, 24, 25]. In fact, towards the end of 2021, the actual consumption slightly exceeded the predicted consumption without the occurrence of the pandemic [12]. Recent studies reported that the pandemic led to greater stress in children with ADHD in general [11], as well as medium-term impacts on children with ADHD of pandemic-related stress specifically [26]. Pre-pandemic studies found prolonged effects of stress exposure in form of worsened and persistent ADHD symptoms from childhood into young adulthood [14, 15]. Because no studies to date have investigated ADHD medication consumption in Europe after COVID-19, this study aimed to assess the long-term impact of the pandemic in the European ADHD medication market, particulary answering the question if the post-pandemic surge is only a catch-up effect or if the pandemic has indeed accelerated consumption growth in the long run. We examined changes in ADHD medicine consumption trends from pre-pandemic (2014 to 2019) to post-pandemic (2021 to 2022) in 28 European countries. We also measured the deviation of the actual consumption in 2022 from the prediction under non-pandemic conditions.
Methods
Data sources
We used quarterly data obtained from IQVIA Multinational Integrated Data Analysis System (IQVIA MIDAS®). IQVIA MIDAS data combine country-level data, healthcare expertise and therapeutic knowledge in 90 + countries to deliver data in globally standardized forms to facilitate multi-country analyses.
The database includes the sales of generic and brand products and does not contain individual-level data. Thus, institutional review board approval was not required. This study is based on sales volume data of ADHD medications from Quarter 1, 2014 to Quarter 4, 2022 of 28 European countries including information about the number of sold standard units, the strength, the active substances, and the sales value of each drug. Some of the substances included in the data set are also approved for other indications than ADHD treatment. However, in this study only sales data of medications specifically indicated for the treatment of ADHD (ATC class N06B) were evaluated.
Population estimates of each country were obtained from the UN World Population Prospects 2022 report [28]. Definitions of the defined daily dose (DDD), which is the assumed average maintenance dose per day for a drug used for its main indication in adults [29] were obtained by the World Health Organization (WHO) for each substance.
Data analysis
As we do not observe the quantity of interest, consumption, directly, we use the sales data as proxy. It is plausible to assume that the error margin of medicine that is sold, but not consumed, remains fairly stable across regions and time, and does not distort the spatial and temporal analysis. We chose DDD per 1000 inhabitants per day as the main quantity of interest. Although individual doses vary, this number strongly correlates with the prevalence of diagnosed patients. Using the country-level sales volume data, the measure ‘DDD per 1000 inhabitants per day’ was calculated as following:
where standard.units are the number of sold standard units of each medication, strength is the dose of its active substance, DDD is the defined daily dose depending on the substance, population is the population estimate of the country at the time of sales and #days is the number of days in the time period. This measure is useful for comparison as it is standardized not only by time but also by population size.
We analyzed the European ADHD medicine consumption usage before and after the pandemic (2014 to 2022), per country and in total. Pre- and post-pandemic time trend coefficients were estimated by linear regression models using consumption data in DDD per 1000 inhabitants per day from 2014 to 2019 (pre-pandemic) and from 2021 to 2022 (post-pandemic) including an intercept, time of sales (linear trend) and quarters as regressors. The year 2020 was left out in the regression analyses to avoid distortions. We tested, for Europe in total and for each country, the one-sided hypothesis that the post-pandemic trend coefficient is not larger than the pre-pandemic trend coefficient. Rejection of this one-sided hypothesis provides evidence for a post-pandemic increase of the trend. Details on the test are given in the Supplement.
Additionally, we analyzed the differences in active substances of ADHD medication. They can be divided into stimulants (amfetamine, dexmethylphenidate, lisdexamfetamine, methylphenidate), which are recommended as first-line pharmacological treatment, and non-stimulants (atomoxetine and guanfacine), which are recommended for patients who cannot tolerate stimulants, do not benefit from them or who suffer from substance use disorders [9, 19]. The effects can last 3–5 h (short-acting) or 8–12 h (long-acting).
To further quantify the impact of the COVID-19 pandemic on ADHD medicine consumption, we forecasted the sales volume of the years 2020 to 2022 based on the national consumption trends until 2019. The impact was assessed by fitting a SARIMA model [10] and comparing its predictions to the actual sales volume. We used R [22], version 4.1.3, for data analysis.
Results
Increased growth of European ADHD medicine consumption after the pandemic
Before the pandemic, the annual ADHD medicine consumption growth in Europe was consistently around 5 to 6% (Table 1). However, from 2018 to 2019, we observed a higher increase of 9.7%, which decreased from 2019 to the pandemic affected year 2020 to 4.7%. In the following years, we observed remarkably higher growth rates of 12.7% in 2021 and 15.2% in 2022.
Comparing ADHD medication consumption by active substances (Table 2), we found increasing trends in all substances. Stimulants (methylphenidate, amfetamine, lisdexamfetamine or dexamfetamine) are by far the most frequently prescribed medications, followed by non-stimulants (atomoxetine or guanfacine). Methylphenidate has the highest share of the European consumption, however, due to rapid growth of lisdexamfetamine medications, its share decreases steadily (Fig. 1). We also found that consumption of long-acting medications increased stronger than prescriptions of short-acting medications, which accounted for 21% of total European consumption in 2014, but for only 15% in 2022 (Table 3).

Share of substances on European ADHD medication consumption. DDD = defined daily dose
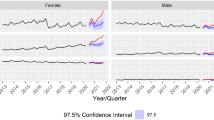
In line with previous studies, we found substantial differences in national ADHD medication use levels in 2019, ranging from 0.009 DDD per 1000 inhabitants per day in Bulgaria to 16.49 in Sweden. In general, the highest levels of medicine consumption were recorded in Scandinavian countries (Sweden, Norway, and Denmark), followed by the Netherlands, Switzerland, and Finland (Figure S2 in the Supplement). Eastern European countries generally showed the lowest consumption levels. However, time trends were comparable across most European countries. In the pre-pandemic years up to 2019, time trend estimates were significant at the 5% level in all countries except Romania and Luxembourg. In the post-pandemic period (2021 to 2022), regression slope estimates were significantly positive in all 28 countries. Moreover, post-pandemic time trend estimates were larger than pre-pandemic in all countries (Table 4; see also Figure S3 in the Supplement). In Luxembourg, and Romania, the consumption trend even switched from declining into increasing during the pandemic. In 26 of the 28 countries, the regression slopes after the pandemic (2021 to 2022) were significantly larger than before the pandemic (2014 to 2019). Non-significant increases were observed in Belgium and Croatia (Table 4). Throughout Europe (Fig. 2), the pre-pandemic regression slope was estimated as 0.03 (p < 0.001), increasing to 0.11 (p < 0.001) in the post-pandemic period. The latter is significantly larger than the former (p < 0.001). The individual-country analogues of Fig. 2 can be found the Supplement (Figure S2).

Quarterly ADHD consumption in Europe. Regression line in pre COVID years (2014–2019) is marked as red line, in post COVID years (2021–2022) as green line. DDD = defined daily dose
Consumption of ADHD medicines exceeds predictions after COVID
For each country and for Europe in total, we calculated the difference between the actual ADHD medication consumption for the period from 2020 to 2022 and the predicted consumption under non-pandemic conditions. Towards this end, seasonal autoregressive integrated moving average (SARIMA) models of order [1])× [1])4 were fitted using the maximum-likelihood method to the quarterly consumption during 2014 Q1 to 2019 Q4. Based on the thus fitted models, quarterly forecasts for the consumption levels in 2020, 2021, and 2022 were obtained. Hence, the pre-pandemic trends in national ADHD medicine consumption were extrapolated under the assumption of unchanged conditions, i.e., without the occurrence of the COVID-19 pandemic, see Fig. 3.

Predicted and actual global quarterly consumption of ADHD medication. DDD = defined daily dose
In the first year of the pandemic, we found lower consumption than predicted in most of the European countries. Twenty of the 28 European countries recorded a drop of ADHD medication consumption in 2020 (Table 5; Fig. 4). The highest losses were in Romania, Portugal, and Italy. Only in three countries (Latvia, Greece, and the Netherlands) did consumption substantially exceed the predictions. In Europe, ADHD medicine consumption amounted to 2.64 instead of the predicted 2.71 DDD per 1000 inhabitants per day, which corresponds to a relative loss of 2.34%. On country average, the national ADHD consumption in 2020 was 4.8% lower than predicted.

Percentage difference of actual and predicted ADHD medication consumption in 28 European countries in DDD per 1000 inhabitants per day in 2020, 2021 and 2022. DDD = defined daily dose
In 2021, ADHD medication consumption in European countries on average returned back to the predicted level (Table 5; Fig. 4). While ten countries still recorded lower actual sales than forecasted, the remaining 18 countries met or even exceeded predictions. On average, the actual national ADHD medicine sales in 2021 were 0.98% above their predictions. Highest losses were recorded in Romania, Slovakia, and Italy, whereas Latvia, Greece, and the Netherlands again surpassed predictions the most. Throughout Europe, the actual consumption in 2021 (2.98 DDD per 1000 inhabitants per day) was 2.65% higher than predicted (2.90 DDD per 1000 inhabitants per day).
In 2022 however, medication usage levels were not only close to pre-pandemic predictions, but clearly exceeded them (Table 5; Fig. 4). In 23 of the 28 countries, the actual ADHD medication consumption was higher than predicted; in ten countries consumption surpassed predictions by more than 20%. The average relative deviation revealed a mean exceedance of national consumption forecasts by 16.4% in 2022. Only in five countries ADHD medicine sales were below the predictions. Belgium (-9%), Slovakia (-6%), the Czech Republic (-4%), Romania (-16%), and Italy (-6%). These countries were also among those most negatively impacted in 2020 and 2021.
Throughout Europe, the consumption in 2022 was predicted as 3.08 DDD per 1000 inhabitants per day without the emergence of COVID-19, whereas the actual consumption amounted to 3.43 DDD per 1000 inhabitants per day, which corresponds to an increase of 11.5%.
Comparing the mean national (unweighted averages) relative differences per quarter (Fig. 5), we found remarkably high exceedances of the predictions in the last three quarters of 2022. While in the first quarter of 2022, the actual consumption levels were on average 7% above forecast, which is about the same extent as the last quarter in 2021, consumption in the second and the third quarters surpasses the pre-pandemic trends by 18.7% and 17.3%, respectively. In Quarter 4 of 2022, the actual consumptions were on average even 23.3% higher than predicted, which contradicts the assumption of the increased ADHD medication use being only a catch-up effect of 2020.

Mean relative difference between actual and predicted ADHD medicine consumption (in DDD per 1000 inhabitants per day) per quarter, 2020–2022. DDD = defined daily dose
Discussion
In this study, we found an increased consumption growth of ADHD medications in Europe after the pandemic. A possible cause is the general increase of mental health issues caused by anti-pandemic mitigation measures, including the worsening of ADHD symptoms [6, 21]. Recent research showed a medium-term impact of pandemic-related stress on children with ADHD [26]. Social withdrawal is also associated with a decreased likelihood of symptom remission in patients with major psychiatric disorders [20], which potentially led to greater ADHD medication demand in the long run. However, other factors unrelated to the pandemic might have also been contributing to the rise in ADHD medication sales. Changing diagnosis criteria as well as increasing awareness of ADHD in media and social media, indicated, e.g., by a steadily increasing popularity of the Google search term “ADHD” [13], led to a significantly increased prevalence in recent years, especially in individuals of colour and females [1]. Although the role of social media and “ADHD influencer” are a relatively new phenomenon, the number of views on TikTok of the hashtag #ADHD was frequently reported as 11 billion as of May 2022 [17] and has reached 33 billion now [27]. Also, access to an ADHD diagnosis has become easier. In several countries, the initial referral to a diagnosis can now be carried out be a GP rather than a psychotherapist [2, 3]. This is a response to the high demand of psychiatric support in comparison to the limited resource, resulting in long waiting times to diagnoses and therapies. Both of these effects, social media and easier access, potentially have been amplified by the pandemic, where access to healthcare resources was limited, but the psychological burden of social isolation and the time spent on social media largely increased.
In line with our results, other studies analyzing the impact of the pandemic on medication use found a significant increase in the consumption of psychotropic drugs in the French population after March 2020 [7] and an increase in rates of psychotropic medication use and psychiatric disorder diagnoses for Danish youths from March 2020 to June 22 [8]. We have also carried out analogous analysis for 17 other countries in different regions of the world. With four notable exceptions (e.g. China, Indonesia), a very similar picture emerges throughout the world. However, as we do not have complete data coverage of the world, most notably, not of North America, which is by far the biggest market of ADHD medicine, this study focused on Europe. Although Europe comprises different cultural areas with quite diverse histories and perceptions of ADHD and strong differences in the diagnosis prevalence, the increase in the consumption trend was observed throughout all considered European countries. This provides evidence that this is not a localized effect that can be attributed to cultural or healthcare-system-specific reasons.
In this study, the use of international pharmaceutical sales data enabled an analysis and quantification of the medium- and long-term effect of the COVID-19 pandemic response measures on ADHD medication consumption in Europe. However, the prevalence of ADHD was not examined as this study only evaluates sales data of ADHD medications. Furthermore, the data do not contain individual-level treatment data necessary to measure trends by age, gender, or appropriateness of prescribing. Therefore, we cannot draw any conclusions regarding overuse, underuse, or misuse.
Conclusion
This study examined the medium-term impact of the COVID-19 pandemic on ADHD medication use by analyzing sales data of 28 European countries from 2014 to 2022. Consistent with previous research [5, 23], we observed a wide variation in ADHD medication use, with the highest usage levels in Northern countries and lower levels in Eastern Europe. However, all countries except Luxembourg and Romania recorded an increasing trend in linear regression models significant at the 5% level in the pre-pandemic period from 2014 to 2019. After a drop in 2020, especially in the second quarter, when social mitigation measures were taken to prevent the spread of the at the time novel Coronavirus, medication consumption returned to the predicted level by 2021 in most countries. Towards the end of 2021, usage levels even tended to exceed predictions. Throughout Europe, the actual consumption was 2.3% below predictions in 2020. In contrast, in 2021, consumption surpassed pre-pandemic predictions by 2.6%. While these exceedances in 2021 might be a catch-up effect due to reduced consumption in previous quarters, the noticeably increased growth observed in all four quarters of 2022 argues in favour of the pandemic having a catalyzing effect on ADHD medication consumption growth in the long run. Throughout Europe, the annual ADHD medicine consumption, predicted as 3.08 DDD per 1000 inhabitants per day, achieved an actual value of 3.43 DDD per 1000 inhabitants per day, corresponding to a relative rise of 11.5%. At country-level, 23 of the 28 European countries recorded higher ADHD medication sales volumes than predicted, ten of them even surpassed expectations by more than 20%. On average, national annual consumption was 16.4% higher than predicted. Quarterly comparisons of predictions and actual values revealed relatively small deviations in Quarter 1 of 2022 but increasing positive deviations in the following quarters with Quarter 4 showing the highest mean national exceedance of forecasts by more than 23%.
In all European countries examined, the estimated regression time trend parameter in the post-pandemic period (2021 to 2022) was higher than in the pre-pandemic period (2014 to 2019). Decreasing trends in Romania and Luxembourg were reversed after the pandemic. In 26 of the 28 countries, the post-pandemic time trend was significantly larger than before the pandemic. In the European total, the slope estimator rose significantly (p < 0.001) from 0.03 in the pre-pandemic period to 0.11 in the post-pandemic period.
Further research is needed to investigate the long-term impact of the pandemic on ADHD prevalence and prescribing patterns as well as medication trends beyond the study period. Moreover, analyses of this study should also be carried out for countries in other continents, to examine if this is a European trend only or if similar effects can be observed globally. Health care systems should build strategies that can prevent population at risk from long term effects caused by socially disruptive events like the pandemic effectively.
Availability of data and materials
The data that support the findings of this study are available from IQVIA but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of IQVIA. Please note that if you do wish to share your raw data and do not have consent from all patients to publish this data, it will need to be de-identified.
Abbreviations
- ADHD:
-
Attention Deficit Hyperactivity Disorder
- DDD:
-
Defined Daily Dose
- SARIMA:
-
Seasonal Autoregressive Integrated Moving Average
- WHO:
-
World Health Organization
References
Abdelnour E, Jansen MO, Gold JA. ADHD diagnostic trends: increased recognition or overdiagnosis? Mo Med. 2022;119(5):467–73.
ADHD Aware. 2022; https://adhdaware.org.uk/what-is-adhd/getting-nhs-diagnosis/ (accessed: 23 Nov 2023).
ADHD City. ; https://adhdcity.nl/en/getting-started (accessed: 23 Nov 2023).
Asherson P, Agnew-Blais J. Annual Research Review: does late‐onset attention‐deficit/hyperactivity disorder exist? J Child Psychol Psychiatry. 2019;60(4):333–52.
Bachmann CJ, Wijlaars LP, Kalverdijk LJ, et al. Trends in ADHD medication use in children and adolescents in five western countries, 2005–2012. Eur Neuropsychopharmacol. 2017;27(5):484–93.
Behrmann JT, Blaabjerg J, Jordansen J, de López KMJ. Systematic review: investigating the impact of COVID-19 on mental health outcomes of individuals with ADHD. J Atten Disord. 2022;26(7):959–75.
Benistand P, Vorilhon P, Laporte C, Bouillon-Minois J-B, Brousse G, Bagheri R, Ugbolue UC, Baker JS, Flaudias V, Mulliez A, Dutheil F. Effect of the COVID-19 pandemic on the psychotropic drug consumption. Front Psychiatry. 2022;13:1020023.
Bliddal M, Rasmussen L, Andersen JH, et al. Psychotropic medication Use and Psychiatric disorders during the COVID-19 pandemic among Danish children, adolescents, and young adults. JAMA Psychiatry. 2022;80(2):176–80.
Bolea-Alamañac B, Nutt DJ, Adamou M, et al. Evidence-based guidelines for the pharmacological management of attention deficit hyperactivity disorder: update on recommendations from the British association for psychopharmacology. J Psychopharmacol. 2014;28(3):179–203.
Brockwell PJ, Davis RA. Introduction to Time Series and forecasting. Springer texts in Statistics 2016, New York. Springer International Publishing.
Frick MA, Meyer J, Isaksson J. The role of comorbid symptoms in perceived stress and sleep problems in adolescent ADHD. Child Psychiatry Hum Dev. 2022;54(4):1141–51.
Gimbach S, Vogel D, Fried R, Faraone SV, Banaschewski T, Buitelaar J, Döpfner M, Ammer R. The impact of the COVID-19 pandemic on ADHD medicine consumption in 47 countries and regions. Eur Neuropsychopharmacol. 2023;73:24–35.
Google Trends. 2023; https://trends.google.com/trends/explore?date=all&q=adhd (accessed: 23 Nov 2023).
Hartman CA, Rommelse N, van der Klugt CL, Wanders RBK, Timmerman ME. Stress exposure and the course of ADHD from Childhood to Young Adulthood: comorbid severe emotion dysregulation or Mood and anxiety problems. J Clin Med. 2019;8:1824.
Humphreys KL, Watts EL, Dennis EL, King LS, Thompson M, Gotlib IH. Stressful life events, ADHD symptoms, and Brain structure in early adolescence. J Abnorm Child Psychol. 2019;47:421–32.
Karlstad O, Zoega H, Furu K, et al. Use of drugs for ADHD among adults - a multinational study among 15.8 million adults in the nordic countries. Eur J Clin Pharmacol. 2016;72:1507–14.
Korducki KM. TikTok trends or the pandemic? What’s behind the rise in ADHD diagnoses. The Guardian. 2022; https://www.theguardian.com/society/2022/jun/02/tiktok-trends-or-the-pandemic-whats-behind-the-rise-in-adhd-diagnoses (accessed: November 22, 2023).
Moffitt TE, Houts R, Asherson P, Belsky DW, Corcoran DL, Hammerle M, Harrington H, Hogan S, Meier MH, Polanczyk GV, Poulton R, Ramrakha S, Sugden K, Williams B, Rohde LA, Caspi A. Is adult ADHD a childhood-onset neurodevelopmental disorder? Evidence from a four-Decade Longitudinal Cohort Study. Am J Psychiatry. 2015;172(10):967–77.
National Institute for Health and Care Excellence (NICE)., 2019. Attention deficit hyperactivity disorder: diagnosis and management. NICE guideline, no. 87. https://www.nice.org.uk/guidance/ng87 (accessed: 22 Nov 2023).
Oliva V, Fanelli G, Kasper S, et al. Social Withdrawal as a trans-diagnostic predictor of short-term remission: a meta-analysis of five clinical cohorts. Int Clin Psychopharmacol. 2022;37(2):38–45.
Panda PK, Gupta J, Chowdhury SR, Kumar R, Meena AK, Madaan P, Sharawat IK, Gulati S. Psychological and Behavioral Impact of Lockdown and Quarantine Measures for COVID-19 Pandemic on Children, Adolescents and Caregivers: A Systematic Review and Meta-Analysis. J Trop Pediatr. 2021;67(1):fmaa122.
R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing 2021, Vienna, Austria. https://www.R-project.org/.
Raman S, Man K, Bahmanyar S, et al. Trends in attention-deficit hyperactivity disorder medication use: a retrospective observational study using population-based databases. Lancet Psychiatr. 2018;5(10):824–35.
Rogers MA, MacLean J. ADHD symptoms increased during the Covid-19 pandemic: a Meta-analysis. J Atten Disord. 2023;27(8):800–11.
Sciberras E, Patel P, Stokes M, et al. Physical health, media use, and mental health in children and adolescents with ADHD during the COVID-19 pandemic in Australia. J Atten Disord. 2022;26(4):549–62.
Summerton A, Bellows ST, Westrupp EM, Stokes MA, Coghill D, Bellgrove MA, Hutchinson D, Becker SP, Melvin G, Quach J, Efron D, Stringaris A, Middeldorp CM, Banaschewski T. Sciberras E. Longitudinal associations between COVID-19 stress and the Mental Health of Children with ADHD. J Atten Disord. 2023;27(10):1065–74.
TikTok for Business. #adhd Trending Hashtag on TikTok, see #adhd analytics. 2023. https://ads.tiktok.com/business/creativecenter/hashtag/adhd?period=1095&countryCode=DE& (accessed: 23 Nov 2023).
United Nations (UN). World population prospects 2022, Online Edition. ; 2022. https://population.un.org/wpp/Download/Standard/Population/ (accessed: 28 July 2023).
WHO Collaborating Centre for Drug Statistics Methodology Oslo., 2022. https://www.whocc.no/ (accessed 3 June 2023).
Acknowledgements
We thank MEDICE Arzneimittel Pütter GmbH & Co. KG for funding this study. We further thank IQVIA for their assistance and information regarding the use of MIDAS data. The authors thank Michaela Ruhmann for a thorough proofreading of the manuscript and Ann-Kathrin Gersmann for fruitful discussions on data collection and interpretation.
Funding
The licence for the IQVIA MIDAS data was funded by MEDICE Arzneimittel Pütter GmbH & Co. KG.
Author information
Authors and Affiliations
Contributions
SG drafted the manuscript, conducted the literature search, made the figures and carried out the data preparation and analysis. DV conceptualised the study, contributed to the statistical methodology and drafted the Technical Appendix in the Supplement. RF advised on and reviewed the data analysis. RA acquired the data and the funding. All authors contributed to the interpretation of the data, the literature search, edited and critically revised the manuscript for important intellectual content.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
SG and DV are employees of MEDICE Arzneimittel Pütter GmbH & Co. KG. RF holds grants from the German Research Foundation (Deutsche Forschungsgemeinschaft) and the German Federal Ministry of Education and Research (Bundesministerium für Bildung und Forschung) unrelated to this work. SVF has received royalties from Elsevier, Guilford Press, Oxford University Press, holds grants from Noven, Otsuka, Shire/Takeda, Arbor, Johnson & Johnson and Supernus, has received consulting fees/honoraria from Akili Interactive Labs, Arbor, Aardvark, Aveksham, Genomind, Ironshore, KemPharm/Corium, Noven, Ondosis, Rhodes, Vallon, holds stock options of Aardvark, Akili, Ironshore, Genomind, and is holder of the US Patent US20130217707 A1. TB has received royalties from Hogrefe, Kohlhammer, CIP Medien, Oxford University Press, has received consulting fees/honoraria from Infectopharm, Janssen Cilag, Medice, Takeda, and is on advisory boards of eyelevel, Infectopharm, Lundbeck, MEDICE, Neurim Pharmaceuticals, Oberberg GmbH, Roche, Takeda. JB is on advisory boards of MEDICE, Angelini, Boehringer-Ingelheim, Servier. MD received consulting income and research support from Lilly, MEDICE, Shire, Takeda, and eyelevel and research support from the German Research Foundation, German Ministry of Education and Research, German Ministry of Health, and Innovation Fund. He received income as head, supervisor, and lecturer of the School of Child and Adolescent Cognitive Behaviour Therapy at the University Hospital Cologne and as consultant for Child Behaviour Therapy at the National Association of Statutory Health Insurance Physicians (Kassenärztliche Bundesvereinigung). He also received royalties from treatment manuals, books and psychological tests published by Beltz, Elsevier, Enke, Guilford, Hogrefe, Huber, Kohlhammer, Schattauer, Springer, Wiley. AR is owner and CEO of MEDICE Arzneimittel Pütter GmbH & Co.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Gimbach, S., Vogel, D., Fried, R. et al. ADHD medicine consumption in Europe after COVID-19: catch-up or trend change?. BMC Psychiatry 24, 112 (2024). https://doi.org/10.1186/s12888-024-05505-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-024-05505-9