
Abstract
Clear cell renal cell carcinoma (CCRCC) is a common tumor of the urological system for which surgery is the preferred treatment, but there is a lack of therapeutic options after surgery. This study aims to explore the biological role of GNG7 on CCRCC from a genetic perspective. Differences in mRNA expression and patient survival of GNG7 in patients with CCRCC and healthy patients were analyzed using the TCGA database. It was observed that GNG7 gene expression was downregulated in CCRCC tissue compared with healthy tissue, and high GNG7 predicted better prognosis for patients, and GNG7 also showed strong variability in clinical and TMN staging. The immune relevance of GNG7 and related genes was explored using renal cancer data from CCLE and TISIDB database. It was verified that the risk score constructed by 7 GNG7-related regulators might be used as an independent prognostic risk factor for CCRCC. A CCRCC prognostic model that involved 7 immune genes was further established to predict the survival probabilities of patients. At last, the GEO database and immunochemical tissue staining were used to validate GNG7 expression in CCRCC. Our study proposed a novel panel of genes to predict CCRCC OS based on GNG7-related immune genes, which may help to accurately predict the prognosis of CCRCC patients and make better clinical decisions for individual treatment.
Similar content being viewed by others


Introduction
Renal cancer is a common urinary system tumor [1]. Due to the lack of obvious clinical features in the early stage of renal cancer, it is impossible to make a more accurate early diagnosis of the disease. Surgical treatment is the preferred choice for renal cancer, since it does not show satisfactory sensitivity to chemotherapy and radiotherapy [2, 3]. Typically, clear cell renal cell carcinoma (CCRCC) is the most important tissue subtype of renal cancer, accounting for 80% of all cases [4]. CCRCC patients are associated with higher mortality and metastasis rates [5]. Therefore, improving the survival rate of CCRCC patients after surgical treatment has always been a problem for urologists. Fortunately, with the advancement in knowledge of biology and comprehensive treatment of CCRCC, tumor immunotherapy has gradually become a promising alternative treatment approach for some urinary tract tumors due to its high accuracy and safety [6,7,8]. The immune system can generate anti-tumor immunity by affecting tumor growth and mutation behaviors. Meanwhile, tumor cells may damage immune cells in different ways [9, 10]. The efficacy of immunotherapy in urinary system tumors has been confirmed [11, 12]. However, similar to other therapies, only a fraction of patients with urinary tract tumors can benefit from immunotherapy [13,14,15]. Some evidence suggests that tumor-infiltrating white blood cells are related to clinical efficacy and cancer prognosis, including CCRCC [16, 17]. However, the molecular characteristics of tumor immune microenvironment (TIME) still need to be explored in depth. Therefore, it is necessary to comprehensively understand the immunology and molecular regulatory mechanisms of CCRCC, so as to ensure the success of immunotherapy.
GNG7 belongs to the large family of G proteins [18]. In the mating pheromone response pathway, G-protein-mediated growth arrest induced by cell contact has been confirmed, while GNG7 may be involved in this process to prevent growth arrest in multicellular organisms and control cell proliferation [19]. According to this hypothesis, cells exposed to GNG7 will stop further proliferation and start the differentiation process mediated by G protein signals. On the other hand, GNG7 is a promising therapeutic target for cancer. Decreased GNG7 expression has been detected in multiple tumors, including head and neck squamous epithelial tumors, breast cancer (BC), gastric cancer (GC), kidney cancer, colorectal cancer (CRC) and lung adenocarcinoma (LUAD) [19,20,21,22,23]. So far, the mechanism supporting the carcinogenic effect of down-regulated GNG7 expression in CCRCC remains largely unclear. In previous reports, genes and methylation are suggested to be related to GNG7’s effect on suppressing tumor progression [19, 24]. However, up to now, no existing study has reported whether GNG7 affects the occurrence and progression of tumor diseases by participating in the immune system.
As for the early detection of tumors, the previously reported techniques include the more costly conventional assays such as protein blotting, immunohistochemistry and reverse transcription-polymerase chain reaction (RT-PCR) [25,26,27]. In recent years, the development of low-cost biosensors for cancer markers has increased rapidly due to the rapid improvement in bioanalytical technology that has made it possible to explore large-scale data [28]. Some studies have indicated that the use of cell surface sialic acid-rich glycoproteins to detect kidney cancer cells in human urine can be better used for the diagnosis of CCRCC and is well compatible in metastatic kidney cancer [29]. In future research efforts, the development and selection of biosensors and biomarkers will definitely be a trend for early cancer diagnosis.
Based on previous studies, there is a reasonable assumption that GNG7 may exert a suppressive role in certain pathogenic aspects of tumors. Our hypothesis posits that GNG7, serving as a potential biomarker in clear cell renal cell carcinoma (CCRCC), could significantly influence the oncogenesis and progression of tumor disease by actively participating in the regulation of the immune system. To test this hypothesis, we utilized the TIMER database to investigate the relationship between GNG7 and immune cells in CCRCC. Subsequently, we carefully selected GNG7-related genes from CCLE kidney cancer cell lines and performed Gene Ontology (GO) and Kyoto Encyclopedia of Genes and Genomes (KEGG) analyses to explore the immune pathways associated with GNG7.
To further validate our findings, we developed a CCRCC prognostic model based on seven GNG7-related immunomodulators. This model's feasibility was subsequently verified through multi-factor regression analysis, using GNG7-related immunomodulators from the TISIDB database.
Through our ongoing study, we aim to discuss the immunological relevance of GNG7 in CCRCC, construct a clinical prognostic model, and identify novel immunotherapeutic targets for CCRCC. We believe that these investigations will contribute to a deeper understanding of the role of GNG7 in tumor-immune interactions, potentially leading to the development of more effective personalized treatment strategies for CCRCC patients. The detailed flow chart of this study is shown in Fig. 1.

Workflow for downstream analysis
Methods and materials
TCGA Datasets
TCGA is a cancer and tumor gene map** project initiated by the U.S. government. It utilizes genome analysis technology, especially for the large-scale genome sequencing, to map the genome mutations of all human cancers and conduct systematic analysis, so as to improve people’s scientific understanding towards the molecular basis of cancer pathogenesis and improve our ability to diagnose, treat and prevent cancer. The CCRCC dataset was obtained from TCGA project. All the RNA-seq transcriptome data and clinical features of 539 cancer tissues and 72 healthy tissues were included. Meanwhile, the selected samples also contained GNG7 gene expression profiles and related clinical information, including age, gender, TNM stage, and grade [30]. The LIMMA software package in R software was used to process the above data [31]. GSE40435(normal:101,tumor:101) was downloaded from GEO database and used for differential analysis validation.
Clinical Proteomic Tumor Analysis Consortium (CPTAC) and UALCAN
CPTAC is a mass spectrometry-based proteomics database that provides protein data for 7 different cancer types. Here, the protein expression of GNG7 was analyzed in detail from CPTAC through UALCAN, an online web resource used to analyze the publicly available cancer data [32].
Detection of tumor infiltrating immune cells in renal cell carcinoma
CIBERSORT is an online data processing website, which uses RNA-Seq data to analyze the immune infiltration profiles of cells through linear support vector regression. After extracting the characteristics of immune cells, the proportions of various cell components in Bulk-seq were reversed on this basis [33]. In the CIBERSORT method, cell components are calculated using the principle of deconvolution, usually linear deconvolution. This method can be used to identify and quantify a total of 22 different types of immune cells in tissues.
GNG7 and tumor immune infiltration
Tumor Immune Evaluation Resources is an online website that can perform detailed analysis and evaluation of immune cell infiltration status in pan-cancer. The website provides three modules for immunization, exploration, and evaluation to investigate the association between immune infiltration and genetic or clinical characteristics, and four modules to explore the association with cancer in TCGA cohort. Each module can generate a functional heat map. The infiltration profiles of six immune cells and four immunosuppressive cells of GNG7 in CCRCC were obtained through this online tool [34].
Gene set enrichment analysis (GSEA)
Cancer Cell Line Encyclopedia (CCLE) is a database developed to investigate the expression of multiple omics in tumor cell lines. The database contains 1457 cell lines and relevant data on the expression profiles, copy numbers, and methylation of genes in the cell lines. CCLE allows to visually map genes expressed in tumors from the perspective of cell lines, including cell line distribution, mutation data, and CpG methylation. In this study, the RNA-seq data of 32 renal cancer cell lines were downloaded and processed from the CCLE online database. After processing and filtering data with P ≥ 0.05, 207 genes significantly related to GNG7 gene were finally obtained. With a limit of 50 genes, a correlation heat map showing the positive and negative correlations with GNG7 expression was obtained. Subsequently, GO functional annotation and KEGG enrichment analysis of GNG7-related genes were further performed.
Immunomodulator
The TISIDB database (www.http://cis.hku.hk/TISIDB/) has calculated the associations between multiple genes and immune characteristics of 30 TCGA cancer types, such as lymphocytes, immunomodulators, and chemokines [35]. The data in this database come from 4176 unpublished records in 2530 individuals, and the publications report 988 genes related to anti-tumor immunity. High-throughput sequencing and genomic analysis data were used to identify genes related to tumor cell immune infiltration. Using P ≤ 0.05 as the threshold, immunoinhibitors and immunostimulators significantly related to GNG7 gene expression were obtained. Thereafter, these obtained immune modulators were uploaded to two web-based tools (https://string-db.org/, http://www.webgestalt.org/). Later, the interaction relationship between proteins, such as physical contact and targeted regulation, was visualized by constructing a protein–protein interaction (PPI) network diagram using the former tool [36]. While the latter tool was employed for KEGG pathway enrichment analysis on GNG7-related immune modulators [37].
Survival analysis
This study aimed to develop a multiple immune gene signal based on the GNG7-related immunomodulators to predict prognosis. Cox regression, which is also referred to as Cox proportional hazard model, is an important method for survival analysis. British statisticians have linked death risk with related factors to construct a new formula, which is expressed as h(t) = h0(t)exp(β1 × 1 + β2 × 2 = …… + βjxj). Where h(t) stands for the risk function of the research object, which changes with time; × 1, × 2…xj are the independent variables, while β1, β2…, βj are the regression coefficients. Next, Kaplan–Meier (K-M) curves, together with univariate and multivariate Cox regression, were used to analyze the relationship between the clinical characteristics of patients and the overall survival (OS) rate of the disease in GNG7-related genes and clinical features. Finally, by combining the clinical characteristics and risk scores of patients, a nomogram was constructed to predict cancer prognosis [38].
External validation
GSE40435(normal:101, tumor:101) was downloaded from GEO database. Each sample contains the amount of GNG7 expression and is used for differential analysis of GNG7 gene expression. Tissue sections were constructed by the Pathology Department of the Second Affiliated Hospital of Chongqing Medical University Paraffin sections were washed with xylene and deparaffinized and hydrated with graded ethanolic solutions. Afterwards, the sections were boiled in sodium citrate buffer, followed by dropwise addition of 3% hydrogen peroxide to inactivate tissue endogenous peroxidase. Then, the incubated and washed sections were incubated with polyclonal GNG7 antibody (A10690-1) overnight at 4 °C, and washed with a biotin-conjugated secondary antibody at 37 °C for 40 min. Sections were then stained with hematoxylin–eosin, and finally, photographs were taken under a light microscope [39].
Statistical analysis
R software (version 3.6.3 and 4.1.1) was adopted for all statistical analyses. Differences between CCRCC and healthy tissues were determined using paired t-test and Mann–Whitney U test. The ggplot2 and survivalROC packages in R software were employed to visualize the differences between tissues and to construct the survival curves.
Results
Here in this study, we first examined the oncogenic role of GNG7 in CCRCC, then further analyzed the relationship between the GNG7 gene and immune infiltrating cells in CCRCC and also discussed the relationship between GNG7-related genes in the immune function pathway in kidney cancer cell lines. To conclude, GNG7-related immunomodulators were identified through the TISIDB online website, and a prognostic prediction model for CCRCC patients was constructed based on key immune prognostic genes, and then the expression of GNG7 in CCRCC was validated using the GEO external validation set and immunohistochemical experiments.
Differential expression and clinicopathological analysis of GNG7 in CCRCC and healthy tissues
The expression of GNG7 in pan-cancer was obtained from TIMER. It was observed from the results that, GNG7 was lowly expressed in most tumors and was significantly different from the expression in healthy tissues (Fig. 2). The expression of GNG7 in CCRCC was further explored based on TCGA database.Consistent with the findings of previous studies, GNG7 expression was significantly correlated between tumor samples and normal samples, including MRNA expression in unpaired and paired samples and protein expression in unpaired samples (Supplementary Figure S1A-C). Moreover, it was figured out based on clinicopathological analysis that, GNG7 expression gradually decreased with the increase in patient age and tumor stage (Fig. 3A, B, D, E). From the perspective of tumor staging, patients with distant metastasis also had lower GNG7 expression than those without distant metastasis (Fig. 3C). Combined with the above results, it was concluded that GNG7 mRNA and protein expression showed consistent attenuation in CCRCC tissues. Moreover, KM curve revealed that GNG7expression was significantly positively correlated with OS (Fig. 3F), and the down-regulated GNG7 expression was more obvious in advanced tumors.

Expression pattern of GNG7 in Pan-cancer perspective. The mRNA expression of GNG7 was downregulated in 17 of 18 cancer types compared with normal tissues. Ns, no significance; *p < 0.05; **p < 0.01; ***p < 0.001

Relationships between GNG7 mRNA levels and clinical pathological characteristics and Kaplan–Meier curves forGNG7. GNG7 mRNA expression was significantly correlated with T stage (A), N stage (B), M stage (C), pathologic stage (D) and age (E). (ns, no significance, *P < 0.05, **P < 0.01, ***P < 0.001), (F) Kaplan–Meier survival curves indicated that CCRCC patients with low GNG7 mRNA expression had a shorter OS than those with high-level of GNG7 (P < 0.001)
Immunohistochemistry and GEO database validation of GNG7 in CCRCC
Immunohistochemistry (IHC) scores the specimens according to the staining intensity, and the staining intensity can be divided into 3 grades, grade 0 with no positive staining, grade 1 weakly positive in pale yellow, grade 2 moderately positive in tan, and grade 3 strongly positive in tan. We made a total of 5 specimens, including 3 renal clear cell carcinoma tissues and 2 adjacent tissues, and made two immunohistochemical sections for each specimen. Immunohistochemical results showed that GNG7 was positive in light yellow in adjacent tissues, while tumor tissues showed no positive staining (Fig. 4A). The expression of GNG7 in adjacent tissues was higher than that in the control group. The results show that GNG7 is low expressed in tumors and significantly different from that in normal tissues (Fig. 4B), which is consistent with our results.

Validation of external GNG7 expression. A Immunohistochemical staining to detect the expression of GNG in kidney tissue. B Expression of GNG7 in kidney tissue in GSE40435
Immune cell infiltration in CCRCC and normal tissues
At first, the characteristic gene expression profiles were extracted and processed by the CiberSort method to systematically describe the infiltration patterns of immune cells. Compared with healthy tissues, the ratios of T cells CD8, T cell CD4 naive, T cells follicular helper, T cells regulatory, Macrophages M0, and Macrophages M1 in CCRCC patients increased significantly, while those of B cells naive, plasma cells, and T cells CD4 memory resting, dendritic cells resting, and mast cells resting significantly reduced (Supplementary Figure S2A). Based on the 32 renal cancer cell lines in the CCLE database, 207 genes significantly related to GNG7 were obtained upon the threshold of P < 0.05. Accordingly, gene data positively and negatively related to GNG7 were obtained (Supplementary Figure S2B 2C). In addition, GO functional annotation was used to evaluate the molecular functions (MFs), biological processes (BPs) and cellular components (CCs) of these genes (Fig. 5A). Moreover, KEGG enrichment analysis of GNG7-related genes was conducted, which suggested that the ERBB signaling pathway was related to the immune status mediated by GNG7, and the Colorectal cancer pathway was associated with the tumor status mediated by GNG7 (Fig. 5B, C, D). The above results indicated that GNG7 might play a role in the tumor environment and immune regulation of CCRCC.

Gene functional enrichment analysis. (A) GO-term function enrichment analysis of GNG7-related genes. (B) KEGG-term function enrichment analysis of GNG7-related genes. Differentially expressed genes were involved in the ERBB signaling pathway (C) and the Colorectal cancer pathway (D)
The associations between GNG7 and immune cells
Next, GNG7 expression profiles in six tumor-infiltrating immune cells (TIICs) and four immunosuppressive cells were obtained based on the TIMER database to further investigate the effect of GNG7 on the immune system (Supplementary Figure S3A-B). The above results indicated that GNG7 might play a role in the immune mechanism of CCRCC. After defining the statistical significance as p ≤ 0.05, 17 Immunoinhibitors and 30 Immunostimulators were obtained from the TISIDB online website (Figs. 6 and 7). Thereafter, the PPI network diagram of GNG7-related immune modulators and the KEGG volcano diagram were plotted using the online tools (Fig. 8A, C) [40]. The credibility threshold of PPI map** was set to 0.4. As shown by the KEGG volcano map, T cell receptor signaling pathway, Intestinal immune network for IgA production, Natural killer cell mediated cytotoxicity, Autoimmune thyroid disease and other pathways were related to the immune status mediated by GNG7-related immune modulators (Fig. 8B), which again verified that GNG7 might participate in and mediate the immune events of CCRCC.

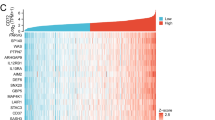
Correlation between GNG7 expression levels and Immunoinhibitors (Only expressions that differ from GNG7 will be displayed)

Correlation between GNG7 expression levels and Immunostimulators (Only expressions that differ from GNG7 will be displayed)

Identification and analysis of immunomodulators associated with the GNG7 gene. A Protein–protein network of 47 GNG7-associated immunomodulators in CCRCC, produced by the STRING online server. B Gene Ontology annotation of 47 GNG7-associated immunomodulators in CCRCC. C Kyoto Encyclopedia of Genes and Genomes pathway analysis of the abovementioned 47 genes
Prognostic significance of immunomodulators related to GNG7 in renal cell carcinoma
The studied variables were subject to univariate and multivariate COX analyses, so as to explore the prognostic value of GNG7-related immunomodulators in CCRCC. Upon univariate Cox regression analysis on GNG7-related immune regulators, the top 21 prognostic genes in CCRCC were obtained, including 17 high-risk genes and 4 low-risk genes (P < 0.01) (Fig. 9A). Thereafter, the corresponding risk score of each sample was obtained by the sum of the product of gene expression and the correlation coefficient, and then the median risk score of all samples was calculated as the threshold to classify samples into high-risk and low-risk groups. Using this method, 7 immune genes related to the prognosis of CCRCC were obtained, including 4 high-risk and 3 low-risk genes (Fig. 9B, Table 1). Furthermore, the K-M survival curve demonstrated that patients with low-risk scores had significantly longer survival time than those with high-risk scores (log-rank test, statistical threshold P < 0.001, Fig. 9C). Also, the risk score chart showed that the risk score increased with the increase in risk, whereas the survival status chart indicated that patients with death risk were concentrated in the high-risk score area (Fig. 9D, E). The risk heat map clearly revealed that the risk scores of patients were significantly positively correlated with IL10RB, KLRK1, TNFSF4, and TNFSF14, but significantly negatively correlated with KDR, PDCD1, and HHLA2 (Fig. 9F). In the univariate Cox regression model, age (HR = 1.032, P < 0.001), stage (HR = 2.279, P < 0.001), clinical grade (HR = 1.863, P < 0.001) and risk score (HR = 1.400, P < 0.001) were significantly related to the survival rate of patients (Fig. 10A). In addition, by multivariate Cox regression analysis after adjusting for age, gender, grade, TMN stage, it was concluded that age (HR = 1.033, P < 0.001), stage (HR = 1.325, P = 0.019), clinical grade (HR = 1.614, P < 0.001) and risk score (HR = 1.382, P < 0.001) were the independent indicators for predicting the prognosis of CCRCC (Fig. 10B). Additionally, the ROC curve was plotted to verify the sensitivity of the model (Fig. 10C). Finally, the prognostic nomogram of CCRCC was obtained and validated by evaluating all the clinical information to predict the survival probability of an individual (Fig. 10D). As revealed by the calibration curve, the red line, which represented the model-predicted survival probability of an individual, was well matched with the grey line, which represented the ideal reference line for the 3-year and 5-year survival rates of an individual in the nomogram (Fig. 10E, F).

The development of prognostic gene signatures based on 47 GNG7-associated immunomodulators. The hazard ratios of genes integrated into the prognostic signatures are shown in the forest plots for CCRCC based on Univariate Cox regression analyses (A) and multivariate Cox regression analyses (B). Kaplan–Meier curves for CCRCC (C). Distribution of risk scores (D), along with survival statuses (E), and gene expression profiles (F) for CCRCC

Construction of a GNG7-related immunomodulator risk model. Univariate (A) and multivariate (B) independent prognostic analysis of independent risk factors for OS in patients with ccRCC. (C) Time-independent ROC analysis of risk scores for OS prediction in the TCGA database. (D) A nomogram for predicting 1-,3- and 5-year survival possibilities of individual CCRCC patients. The calibration curve of 3-year (E) and 5-year survival of CCRCC patients (F). The 45◦ grey line represented a perfect uniformity between nomogram-predicted and real possibilities
Discussion
Tumor immunity includes antigen presentation, T cell activation, avoidance of local suppression and tumor cell killing, which is a complex process [41]. Failure of each of these steps may reduce the efficacy of immunotherapy and cause incalculable harm. Therefore, the appropriate choice of immunotherapy is a major challenge in oncology treatment. Biomarkers that reflect the efficacy of immunotherapy and the prognosis of tumor patients are very important for treatment decisions in CCRCC.
GNG7 (G protein γ subunit 7) is a subunit of heterotrimeric G protein [42]. Previous experiments have shown that GNG7 expression reduces tumor volume in mice [23]. GNG7 is the first autophagy-inducing regulator of Gγ protein reported [43]. A study shows that low expression of GNG7 may induce the proliferation of LUAD tumor cells, increase the probability of invasion in vitro, and promote tumor growth and development in vivo [44]. In addition, GNG7 inhibits cell division by regulating the actin cytoskeleton, and it shows low expression in many tumors [19,20,21,22,23, 43, 45]. Ohta et al. reported that the expression of GNG7 in esophageal cancer was extremely suppressed compared with that in normal tissues. Such inhibition is related to tumor invasion and disease prognosis and is regulated by miRNAs. However, the GNG7 expression-induced progression of esophageal cancer may be attributed to the hypermethylation of GNG7 promoter [24]. In addition, Hartmann et al. also drew the same conclusion in head and neck tumors that the expression of GNG7 was related to tumor size. They also found that the expression of GNG7 protein was significantly related to tumor keratinization, and the lack of keratinization usually indicates tumor progression [6]. Recent studies suggested that GNG7 is highly associated with the B-cell receptor signaling pathway. Low levels of B-cell infiltration in patients with low GNG7 expression often suggest a poorer prognosis [46].
Consistent with the results of previous studies, our results showed that GNG7 mRNA and protein expression was down-regulated in CCRCC tissues, and the down-regulation degree was extremely related to tumor grade. K-M curve survival analysis verified that GNG7 down-regulation was significantly related to high mortality. Multivariate Cox analysis indicated that the expression of GNG7 served as an independent risk factor for the OS of CCRCC. Moreover, the tumor prognostic model constructed based on GNG7-related immunomodulators was able to predict the 3-year and 5-year survival of CCRCC. In addition, the model analysis curve was well matched with the standard curve of CCRCC survival. Based on previous studies and this research, it was reasonably speculated that GNG7 predicted the diagnosis and prognosis of CCRCC well, and it was also used as an important evaluation factor for tumor recurrence and early metastasis.
In the presented study, we used COX regression analysis to obtain 7 immune regulators associated with GNG7, after deriving 7 immune genes based on further risk scoring. Among them, KDR, PDCD1, and HHLA2 are prognostic protective genes for CCRCC, in contrast to IL10RB, KLRK1, TNFSF4, and TNFSF14, which are risk factors for prognosis in CCRCC. SU et al. concluded by sequencing that epigenetic silencing of the KDR gene could affect the methylation of CCRCC and thus the tumor invasion [47]. ** disease development [9]. Before this, immune cells have been confirmed to exhibit a unique distribution and infiltration ratio in the tumor microenvironment (TME), and immunotherapy has gradually become an alternative treatment for many cancer patients [53]. The immune cell characteristics in CCRCC are manifested by infiltration of a variety of T cells, including CD8 + T cells and CD4 + T cells [54, 55]. The prognosis of CCRCC patients can be predicted clinically based on the infiltration patterns of different immune cells. Liu et al. found that GNG7 served as the autophagy-inducing gene mainly because it interacts with and inhibits the mTOR1 signaling pathway, and comprehensively suppresses the growth of effector cells by inducing autophagic cell death and cell division inhibition [43]. Therefore, it is reasonably speculated that GNG7 may be involved in the progression, metastasis, immune control, and drug resistance of CCRCC. In this study, we found that GNG7 was tightly related to TIICs. Previous reports indicate that high CD8 + T cell infiltration is associated with poor prognosis of CCRCC [54, 55]. Our research also discovered that GNG7 was negatively correlated with CD8 + T cell infiltration. Such result seems to further prove that GNG7, a tumor suppressor gene, is involved in tumor progression to some extent in the immune mechanism of tumors.
Furthermore, GNG7-related immunomodulators were used as the research object and a prognostic model for CCRCC was established through multivariate analysis. According to our results, the model was well matched with the actual survival time. According to the above results, we can construct a prognostic model for CCRCC based on the immune infiltration characteristics, and the expression of GNG7 and the characteristics of related TIICs can serve as the prognostic biomarkers and immunotherapeutic targets for CCRCC.
Conclusions
In summary, our study suggests that low expression of GNG7 is strongly associated with immune cell infiltration patterns in CCRCC tumors. GNG7 may function as a tumor suppressor gene through immune pathways in CCRCC. We have developed a prognostic prediction model based on GNG7-related immunomodulators to forecast CCRCC patient outcomes. GNG7 shows promise as a potential therapeutic target for CCRCC. However, further validation through clinical trials and experimental studies is warranted to fully assess its clinical significance.
Availability of data and materials
Publicly available datasets were analyzed in this study. This data can be found here: TCGA database (https://portal.gdc.cancer.gov/) and GEO database (https://www.ncbi.nlm.nih.gov/geo/).
References
Siegel RL, Miller KD, Fuchs HE, et al. Cancer Statistics, 2021. CA Cancer J Clin. 2021;71(1):7–33.
Barata PC, Rini BI. Treatment of renal cell carcinoma: Current status and future directions. CA Cancer J Clin. 2017;67(6):507–24.
Escudier B, Porta C, Schmidinger M, et al. Renal cell carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann Oncol. 2019;30(5):706–20.
Grignon DJ, Che M. Clear cell renal cell carcinoma. Clin Lab Med. 2005;25(2):305–16.
Perazella MA, Dreicer R, Rosner MH. Renal cell carcinoma for the nephrologist. Kidney Int. 2018;94(3):471–83.
Hammers H. Immunotherapy in kidney cancer: the past, present, and future. Curr Opin Urol. 2016;26(6):543–7.
Chowdhury N, Drake CG. Kidney cancer: an overview of current therapeutic approaches. Urol Clin North Am. 2020;47(4):419–31.
D Grivas P, G Redman B. Immunotherapy of kidney cancer. Curr Clin Pharmacol. 2011; 6:(3) 151–163
Fridman WH, Zitvogel L, Sautès-Fridman C, et al. The immune contexture in cancer prognosis and treatment. Nature reviews. Clin Oncol. 2017;14(12):717–34.
Gandellini P, Andriani F, Merlino G, et al. Complexity in the tumour microenvironment: Cancer associated fibroblast gene expression patterns identify both common and unique features of tumour-stroma crosstalk across cancer types. Semin Cancer Biol. 2015;35:96–106.
Motzer RJ, Rini BI, McDermott DF, et al. Nivolumab plus ipilimumab versus sunitinib in first-line treatment for advanced renal cell carcinoma: extended follow-up of efficacy and safety results from a randomised, controlled, phase 3 trial. Lancet Oncol. 2019;20(10):1370–85.
Motzer RJ, Penkov K, Haanen J, et al. Avelumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. New Engl J Med. 2019;380(12):1103–15.
Challis GB, Stam HJ. The spontaneous regression of cancer. A review of cases from 1900 to 1987. Acta Oncologica (Stockholm, Sweden). 1990; 29(5):545–550.
Everson TC, Cole WH. Spontaneous regression of cancer: preliminary report. Ann Surg. 1956;144(3):366–83.
Janiszewska AD, Poletajew S, Wasiutyński A. Spontaneous regression of renal cell carcinoma. Contemp Oncol (Poznan, Poland). 2013;17(2):123–7.
Aran D, Sirota M, Butte AJ. Systematic pan-cancer analysis of tumour purity. Nat Commun. 2015;6:8971.
Binnewies M, Roberts EW, Kersten K, et al. Understanding the tumor immune microenvironment (TIME) for effective therapy. Nat Med. 2018;24(5):541–50.
Shibata K, Mori M, Tanaka S, et al. Identification and cloning of human G-protein gamma 7, down-regulated in pancreatic cancer. Biochem Biophys Res Commun. 1998;246(1):205–9.
Shibata K, Tanaka S, Shiraishi T, et al. G-protein gamma 7 is down-regulated in cancers and associated with p 27kip1-induced growth arrest. Cancer Res. 1999;59(5):1096–101.
Hartmann S, Szaumkessel M, Salaverria I, et al. Loss of protein expression and recurrent DNA hypermethylation of the GNG7 gene in squamous cell carcinoma of the head and neck. J Appl Genetics. 2012;53(2):167–74.
Mei J, Wang T, Zhao S, et al. Osthole inhibits breast cancer progression through upregulating tumor suppressor GNG7. J Oncol. 2021;2021:6610511.
Xu S, Zhang H, Liu T, et al. G Protein γ subunit 7 loss contributes to progression of clear cell renal cell carcinoma. J Cell Physiol. 2019;234(11):20002–12.
Zheng H, Tian H, Yu X, et al. G protein gamma 7 suppresses progression of lung adenocarcinoma by inhibiting E2F transcription factor 1. Int J Biol Macromol. 2021;182:858–65.
Ohta M, Mimori K, Fukuyoshi Y, et al. Clinical significance of the reduced expression of G protein gamma 7 (GNG7) in oesophageal cancer. Br J Cancer. 2008;98(2):410–7.
Argani P, Hicks J, De Marzo AM, et al. Xp11 translocation renal cell carcinoma (RCC): extended immunohistochemical profile emphasizing novel RCC markers. Am J Surg Pathol. 2010;34(9):1295–303.
Fromowitz FB, Viola MV, Chao S, et al. ras p21 expression in the progression of breast cancer. Hum Pathol. 1987;18(12):1268–75.
Livak KJ, Schmittgen TD. Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method. Methods. 2001;25(4):402–8.
Stobiecka M, Ratajczak K, Jakiela S. Toward early cancer detection: focus on biosensing systems and biosensors for an anti-apoptotic protein survivin and survivin mRNA. Biosens Bioelectron. 2019;137:58–71.
Zhang L, Yu C, Gao R, et al. An impedimetric biosensor for the diagnosis of renal cell carcinoma based on the interaction between 3-aminophenyl boronic acid and sialic acid. Biosens Bioelectron. 2017;92:434–41.
Tomczak K, Czerwińska P, Wiznerowicz M. Wiznerowicz. The Cancer Genome Atlas (TCGA): an immeasurable source of knowledge. Contemp Oncol (Pozn). 2015; 19(1a): A68–77.
Ritchie ME, Phipson B, Wu DI, et al. limma powers differential expression analyses for RNA-sequencing and microarray studies. Nucleic Acids Res. 2015;43(7).
Chen F, Chandrashekar DS, Varambally S, et al. Pan-cancer molecular subtypes revealed by mass-spectrometry-based proteomic characterization of more than 500 human cancers. Nat Commun. 2019;10(1):5679.
Newman AM, Liu CL, Green MR, et al. Robust enumeration of cell subsets from tissue expression profiles. Nat Methods. 2015;12(5):453–7.
Li T, Fu J, Zeng Z, et al. TIMER2.0 for analysis of tumor-infiltrating immune cells. Nucleic Acids Res. 2020; 48(W1):W509-w514.
Ru B, Wong CN, Tong Y, et al. TISIDB: an integrated repository portal for tumor-immune system interactions. Bioinformatics. 2019;35(20):4200–2.
Szklarczyk D, Gable AL, Lyon D, et al. STRING v11: protein-protein association networks with increased coverage, supporting functional discovery in genome-wide experimental datasets. Nucleic Acids Res. 2019;47(D1):D607-d613.
Kanehisa M, Furumichi M, Tanabe M, et al. KEGG: new perspectives on genomes, pathways, diseases and drugs. Nucleic Acids Res. 2017;45(D1):D353-d361.
Yin CD, Hou YL, Liu XR, et al. Development of an immune-related prognostic index associated with osteosarcoma. Bioengineered. 2021;12(1):172–82.
Uhlén M, Fagerberg L, Hallström BM, et al. Proteomics. Tissue-based map of the human proteome. Science. 2015; 347:(6220) 1260419.
Kanehisa M, Furumichi M, Sato Y, et al. KEGG for taxonomy-based analysis of pathways and genomes. Nucleic Acids Res. 2023;51(D1):D587-d592.
Greten TF, Mauda-Havakuk M, Heinrich B, et al. Combined locoregional-immunotherapy for liver cancer. J Hepatol. 2019;70(5):999–1007.
Schwindinger WF, Mirshahi UL, Baylor KA, et al. Synergistic roles for G-protein γ3 and γ7 subtypes in seizure susceptibility as revealed in double knock-out mice. J Biol Chem. 2012;287(10):7121–33.
L Liu J, Ji X, Li Z, et al. G protein γ subunit 7 induces autophagy and inhibits cell division. Oncotarget. 2016; 7(17):24832–24847.
Zhao X, Zhang XC, Zang K, et al. MicroRNA miR-19b-3p mediated G protein γ subunit 7 (GNG7) loss contributes lung adenocarcinoma progression through activating Hedgehog signaling. Bioengineered. 2021;12(1):7849–58.
Zhang X, Bedigian AV, Wang W, et al. G protein-coupled receptors participate in cytokinesis. Cytoskeleton (Hoboken, N.J.). 2012; 69(10):810–818.
Wei Q, Miao T, Zhang P, et al. Comprehensive analysis to identify GNG7 as a prognostic biomarker in lung adenocarcinoma correlating with immune infiltrates. Front Genet. 2022;13.
Su X, Zhang J, Mouawad R, et al. NSD1 Inactivation and SETD2 mutation drive a convergence toward loss of function of H3K36 writers in clear cell renal cell carcinomas. Cancer Res. 2017;77(18):4835–45.
**ang Z, Shen E, Li M, et al. Potential prognostic biomarkers related to immunity in clear cell renal cell carcinoma using bioinformatic strategy. Bioengineered. 2021;12(1):1773–90.
Zhou QH, Li KW, Chen X, et al. HHLA2 and PD-L1 co-expression predicts poor prognosis in patients with clear cell renal cell carcinoma. J Immunother Cancer. 2020;8:(1):e000157.
Jiang Y, Gou X, Wei Z, et al. Bioinformatics profiling integrating a three immune-related long non-coding RNA signature as a prognostic model for clear cell renal cell carcinoma. Cancer Cell Int. 2020;20:166.
He J, Zhong Y, Sun Y, et al. Construction of an immune-related prognostic model by exploring the tumor microenvironment of clear cell renal cell carcinoma. Anal Biochem. 2022;643.
Wu T, Dai Y. Tumor microenvironment and therapeutic response. Cancer Lett. 2017;387:61–8.
Sharma P, Hu-Lieskovan S, Wargo JA, et al. Primary, adaptive, and acquired resistance to cancer immunotherapy. Cell. 2017;168(4):707–23.
Chevrier S, Levine JH, Zanotelli VR, et al. An immune atlas of clear cell renal cell carcinoma. Cell.2017; 169(4):736–749.e718.
Şenbabaoğlu Y, Gejman RS, Winer AG, et al. Tumor immune microenvironment characterization in clear cell renal cell carcinoma identifies prognostic and immunotherapeutically relevant messenger RNA signatures. Genome Biol. 2016;17(1):231.
Acknowledgements
Not applicable.
Funding
This work was supported by the National Natural Science Foundation of China (Grant No. 81803057); Kuanren Talent Program of the Second Affiliated Hospital of Chongqing Medical University (KY2019Y2016).
Author information
Authors and Affiliations
Contributions
Conceptualization and Methodology: Jun Zheng, Weili Zhang; Date Analysis and Writing—Original Draft Preparation: Jun Zheng; Writing—Review and Editing and Supervision: Junyong Zhang, Weili Zhang; Project Administration: Jun Zheng, Weili Zhang. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The relevant data provided by TCGA and GEO are publicly available and open, and do not require the approval of the local ethics committee. The studies involving human participants were reviewed and approved by The Second Affiliated Hospital of Chongqing Medical University(number:2021–283).Informed consent was taken from all patients prior to using the tissues samples for scientific research. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
All of the authors declared there are no conflicts of interests for this manuscript.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Figure S1. The mRNA and protein expression of GNG7 in CCRCC.(A) The mRNA expression levels of GNG7 in 72 CCRCC and matched-adjacent normal samples. (B) The mRNA expression levels of CCRCC in 539 CCRCC samples and 72 normal samples. (C) The protein expression levels of GNG7 based on CPTAC. (ns, no significance, *P < 0.05, **P < 0.01, ***P < 0.001).
Additional file 2:
Figure S2. Correlation of immune cell infiltration and the heatmaps of differentially expressed genes (DEGs) regulated by GNG7 in CCRCC. (A) Violin plot visualizing the difference in immune infiltration between normal and tumor tissues. Gene data related to GNG7 positively (B) and negatively (C) can be obtained. (*P < 0.05, **P < 0.01, ***P < 0.001).
Additional file 3:
Figure 3. The relationship between GNG7 expression and tumor immune cell infiltration. (A) Relationships between the GNG7 expression and six tumor-infiltrating immune cells. (B) Relationships between the GNG7 expression and 4 types of immunosuppressive cells.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zheng, J., Zhang, W. & Zhang, J. Establishment of a new prognostic risk model of GNG7 pathway-related molecules in clear cell renal cell carcinoma based on immunomodulators. BMC Cancer 23, 864 (2023). https://doi.org/10.1186/s12885-023-11265-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-023-11265-8