
Abstract
Although the COVID-19 pandemic has largely not clinically affected infants in neonatal intensive care units around the globe, it has affected how care is provided. Most hospitals, including their NICUs, have significantly reduced parental and family visitation privileges. From an ethical perspective, this restriction of parental visitation in settings where infectious risk is difficult to understand. No matter what the right thing to do is, NICUs are currently having to support families of their patients via different mechanisms. In this perspective, we discuss ways NICUs can support parents and families when they are home and when they are in the NICU as well as provide infants the support needed when family members are not able to visit.
Similar content being viewed by others
Introduction
To say the COVID-19 pandemic has upended the delivery of healthcare in the United States and the rest of the world would be a gross understatement. While the neonatal intensive care unit (NICU) has escaped, for the most part, the ramifications of having patients critically ill with COVID-19, the impact of this pandemic snaked its way through row upon row of incubators [31]. Hall et al. recommend offering peer support to NICU families as one of the primary components of family-centered care [32]. Most studies evaluating peer support in the NICU have looked at in-person programs moderated by former NICU parents. However, with visitation restrictions and recommendations for social distancing in the era of COVID-19, it is unlikely that these support programs can meet in or outside of the hospital. With that, families may look to internet support groups even more. Benefits to online support groups include the ability to access groups specific to their needs (i.e., congenital anomalies, genetic disorders) and on their own time [32]. In addition, parents can post anonymously, there may be decreased biases based on gender or socioeconomic status, and support can continue beyond hospitalization [32,33,34,35]. Of course, internet support groups can have drawbacks. Nonsupportive posts, misinformation, or unreliable data may be shared, especially if the group is not followed by experienced or knowledgeable moderators [32, 36]. Some online support groups can be found in Table 1 and additional support groups sorted by country can be found at the European Foundation for the Care of Newborn Infants website. Additional strategies for families while away from their infant include journaling and tracking NICU milestones and developments [37].
Supporting families in the NICU
When parents are allowed to visit in the NICU, supporting them in the moment is imperative. Studies have shown that in general, parents do feel supported in the NICU from both nursing and medical providers [38]. However, there is consistent desire for more information on their child as well as emotional support [38,39,40]. In times of reduced visitation, how do we enhance psychosocial support of NICU parents? Hall et al. provide several recommendations that can be quickly implemented and/or augmented (Table 2) [41]. Ensuring that mental health professionals such as psychologists and social workers continue to work with families is imperative. Pastoral or religious care personnel can also supplement support while families are in the NICU. Palliative care teams and ethics committees may also benefit certain populations within the NICU and ensuring that these services are still provided is important.
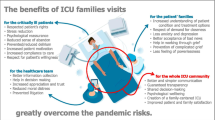
For institutions that severely limited visitation of parents to the NICU, a central tenet of modern neonatology was unable to be performed by the parents. Kangaroo Care has been a part of neonatology since 1978 [42]. Countless neonates have benefitted from Kangaroo Care with benefits including; improved temperature regulation, improved sleep-wake cycles, and augmented growth [43]. To deny parents the experience to provide kangaroo care and neonates the demonstrated ability to reap its benefits seems imprudent, especially when, if available, PPE could mitigate unwanted effects of a viral agent. Other ways that families can impact the care when they are visiting include reading to their infants. Several studies have demonstrated improved parental bonding and decreased severity of postpartum depression after reading to their baby [44,45,46]. Parent talk has also been demonstrated to be the strongest predictor of preterm infant vocalizations at 32 and 36 weeks’ gestation [47]. It was noted that infants were exposed to more conversational language when parents were present than when parents were absent [47].
Supporting infants in the NICU
The impact on reduced visitation does not simply affect the visitor, but also has profound impact on the patient as well. The neurobehavioral impact of parental visitation on infants is undeniable [48, 49]. So, in time of reduced visitation, the NICU team needs to ensure that care typically provided by parents does not stop. Talking in conversations to the infant, holding and interacting all can have significant impact over time. Music therapy has been shown to reduce infant respiratory rates and may have other physiological benefits [50]. Ensuring that therapy services such as occupational, speech, and physical therapists continue to help provide developmental support is imperative during this time.
In conclusion, although there is substantial evidence that would suggest parental visitation should not change in the NICU environment, we understand that hospital and infectious disease policies may supersede unit guidelines in the attempt to mitigate viral spread. If parental visitation is restricted, there are mechanisms that NICUs can utilize to ensure that families and infants continue to be supported both in the hospital and when they are away from the hospital.
References
Zeng L, **a S, Yuan W, Yan K, **ao F, Shao J, et al. Neonatal early-onset infection with SARS-CoV-2 in 33 neonates born to mothers with COVID-19 in Wuhan, China. JAMA Pediatr. 2020;174:722–25.
Lavizzari A, Klingenberg C, Profit J, Zupancic JAF, Davis AS, Mosca F, et al. International comparison of guidelines for managing neonates at the early phase of the SARS-CoV-2 pandemic. Pediatr Res. 2020. https://doi.org/10.1038/s41390-020-0976-5. [Epub ahead of print].
Jester BJ, Uyeki TM, Patel A, Koonin L, Jernigan DB. 100 years of medical countermeasures and pandemic influenza preparedness. Am J Public Health. 2018;108:1469–72.
Horby P. Improving preparedness for the next flu pandemic. Nat Microbiol. 2018;3:848–50.
Barfield WD, Krug SE. Committee on Fetus and Newborn, Disaster Preparedness Advisory Council. Disaster preparedness in neonatal intensive care units. Pediatrics. 2017;139:e20170507.
Wynia M. Ethics and public health emergencies: restrictions on liberty. Am J Bioeth. 2007;7:1–5.
John Stuart Mill. On Liberty. Oxford, England. Oxford University Press; 1859.
Siracusa Principles on the Limitation and Derogation Provisions in the International Covenant on Civil and Political Rights, U.N. Doc E/CN.4/1985/4, Annex (1985).
Silva D, Smith M. Limiting rights and freedoms in the context of Ebola and other public health emergencies: how the principle of reciprocity can enrich the application of the Siracusa Principles. Health Hum Rights. 2015;17:E52–7.
Cook TM. Personal protective equipment during the coronavirus disease (COVID) 2019 pandemic—a narrative review. Anaesthesia. 2020;75:920–27.
Bai Y, Yao L, Wei T, Tian F, ** DY, Chen L, et al. Presumed asymptomatic carrier transmission of COVID-19. JAMA. 2020;323:1406–7.
Shul JE, Messina M, Hill-Ricciuti A, Maykowski P, Leone T, Sahni R, et al. Impact of respiratory viruses in the neonatal intensive care unit. J Perinatol. 2018;381:1556–65.
NICHD extremely preterm birth outcomes tool. https://www.nichd.nih.gov/research/supported/EPBO/use. Accessed 10 May 2020.
Blendon RJ, Koonin LM, Benson JM, Cetron MS, Pollard WE, Mitchell EW, et al. Public response to community mitigation measures for pandemic influenza. Emerg Infect Dis. 2008;14:778–86.
Murad Y. As Trump eyes restarting economy, nearly 3 in 4 voters support national quarantine. 2020. Morning Consult. https://morningconsult.com/2020/03/25/coronavirus-national-quarantine-trump/. Accessed 10 May 2020.
Turpin H, Urben S, Ansermet F, Borghini A, Murray MM, Muller-Nix C. The interplay between prematurity, maternal stress and children’s intelligence quotient at age 11: a longitudinal study. Sci Rep. 2019;9:450.
Committee on Hospital Care. Family-centered care and the pediatrician’s role. Pediatrics. 2003;112:691–96.
Epstein EG, Arechiga J, Dancy M, Simon J, Wilson D, Alhusen JL. Integrative review of technology to support communication with parents of infants in the NICU. J Obstet Gynecol Neonatal Nurs. 2017;46:357–66.
Epstein E, Sherman J, Blackman A, Sinkin RA. Testing the feasibility of skype and facetime updates with parents in the neonatal intensive care unit. Am J Crit Care. 2015;24:290–96.
Globus O, Leibovitch L, Maayan-Metzger A, Schushan-Eisen I, Morag I, Mazkereth R, et al. The use of short message services (SMS) to provide medical updating to parents in the NICU. J Perinatol. 2016;36:739–43.
Gray JE, Safran C, Davis RB, Pompilio-Weitzner G, Stewart JE, Zaccagnini L, et al. Baby CareLink: using the internet and telemedicine to improve care for high-risk infants. Pediatrics. 2000;106:1318–24.
Gund A, Sjoqvist BA, Wigert H, Hentz E, Lindecrantz K, Bry K. A randomized controlled study about the use of eHealth in the home health care of premature infants. BMC Med Inform Decis Mak. 2013;13:22.
Joshi A, Chyou PH, Tirmizi Z, Gross J. Web camera use in the neonatal intensive care unit: impact on nursing workflow. Clin Med Res. 2016;14:1–6.
Lindberg B, Axelsson K, Ohrling K. Experience with videoconferencing between a neonatal unit and the families’ home from the perspective of certified paediatric nurses. J Telemed Telecare. 2009;15:275–80.
Lindberg B, Axelsson K, Ohrling K. Taking care of their baby at home but with nursing staff as support: the use of videoconferencing in providing neonatal support to parents of preterm infants. J Neonatal Nurs. 2009;15:47–55.
Piecuch RE, Roth RS, Clyman RI, Sniderman SH, Riedel PA, Ballard RA. Videophone use improves maternal interest in transported infants. Crit Care Med. 1983;11:655–56.
Rhoads SJ, Green A, Gauss CH, Mitchell A, Pate B. Web camera use of mothers and fathers when viewing their hospitalized neonate. Adv Neonatal Care. 2015;15:440–46.
Rhoads SJ, Green A, Mitchell A, Lynch CE. Neuro-protective core measure 2: partnering with families—exploratory study on web-camera viewing of hospitalized infants and the effect on parental stress, anxiety, and bonding. Newborn Inform Nurs Rev. 2015;15:104–10.
Yeo C, Ho SK, Khong K, Lau Y. Virtual visitation in the neonatal intensive care: experience with the use of internet and telemedicine in a tertiary neonatal unit. Perm J. 2011;15:32–36.
Northwestern Now. New app allows NICU families to ‘visit’ baby during COVID-19 pandemic. https://news.northwestern.edu/stories/2020/03/nicu-app-limited-visitation-covid-19/. Accessed 5 May 2020.
Dahan S, Bourque CJ, Reichherzer M, Prince J, Mantha G, Savaria M, et al. Peer-support groups for families in neonatology: why and how to get started? Acta Paediatr. 2020. https://doi.org/10.1111/apa.15312. [Epub ahead of print].
Hall SL, Ryan DJ, Beatty J, Grubbs L. Recommendations for peer-to-peer support for NICU parents. J Perinatol. 2015;35:S9–13.
Dunham P, Hurshman A, Litwin E, Gusella J, Ellsworth C, Dodd P. Computer-mediated social support: single young mothers as a model system. Am J Community Psychol. 1998;26:281–306.
McNamara D. Health-oriented telecommunication: a community resource. Nurs Manag. 1994;25:40–41.
Kiesler S, Siegel J, McGuire T. Social psychological aspects of computer mediated communication. Am Psychol. 1984;39:1123–34.
Scharer K. Internet social support for parents: the state of the science. J Child Adolesc Psychiatr Nurs. 2005;18:26–35.
Carley A. Can journaling provide support for NICU families? J Spec Pediatr Nurs. 2012;17:254–57.
Franck LS, Axelin A. Differences in parents’, nurses’ and physicians’ views of NICU parent support. Acta Paediatr. 2013;102:590–96.
Mok E, Leung SF. Nurses as providers of support for mothers of premature infants. J Clin Nurs. 2006;15:726–34.
Tran C, Medhurst A, O’Connell B. Support needs of parents of sick and/or preterm infants admitted to a neonatal unit. Neonatal Paediatr Child Health Nurs. 2009;12:12–17.
Hall SL, Cross J, Selix NW, Patterson C, Segre L, Chuffo-Siewaert R, et al. Recommendations for enhancing psychosocial support of NICU parents through staff education and support. J Perinatol. 2015;35:529–36.
Charpak N, Ruiz JG, Zupan J, et al. Kangaroo Mother Care: 25 years after. Acta Paediatr. 2005;94:514–22.
Campbell-Yeo ML, Disher TC, Benoit BL, et al. Understanding kangaroo care and its benefits to preterm infants. Pediatr Health Med Ther. 2015;6:15–32.
Scala M, Seo S, Lee-Park J, McClure C, Scala M, Palafoutas JJ, et al. Effect of reading to preterm infants on measures of cardiorespiratory stability in the neonatal intensive care unit. J Perinatol. 2018;38:1536–41.
Levesque BM, Tran A, Levesque E, Shrestha H, Silva R, Adams M, et al. Implementation of a pilot program of Reach Out and Read in the neonatal intensive care unit: a quality improvement initiative. J Perinatol. 2018;38:759–66.
UVAToday. “Story time: a novel solution for preemies, moms suffering from postpartum depression.” 2019. https://news.virginia.edu/content/story-time-novel-solution-preemies-moms-suffering-postpartum-depression. Accessed 12 May 2020.
Caskey M, Stephens B, Tucker R, Vohr B. Importance of parent talk on the development of preterm infant vocalizations. Pediatrics. 2011;128:910–16.
Reynolds LC, Duncan MM, Smith GC, Mathur A, Neil J, Inder T, et al. Parental presence and holding in the neonatal intensive care unit and associations with early neurobehavior. J Perinatol. 2013;33:636–41.
Latva R, Lehtonen L, Salmelin RK, Tamminen T. Visiting less than every day: a marker for later behavioral problems in Finnish preterm infants. Arch Pediatr Adolesc Med. 2004;158:1153–57.
Bieleninik L, Ghetti C, Gold C. Music therapy for preterm infants and their parents: a meta-analysis. Pediatrics. 2016;138:e20160971.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Murray, P.D., Swanson, J.R. Visitation restrictions: is it right and how do we support families in the NICU during COVID-19?. J Perinatol 40, 1576–1581 (2020). https://doi.org/10.1038/s41372-020-00781-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41372-020-00781-1
- Springer Nature America, Inc.
This article is cited by
-
Families as partners in neonatal neuro-critical care programs
Pediatric Research (2024)
-
Multisensory stimulation bundles on sleep and neurobehavioral development in the first year after birth in very preterm infants: a randomized crossover controlled study protocol
Trials (2023)
-
The predictive roles of parental stress and intolerance of uncertainty on psychological well-being of parents with a newborn in neonatal intensive care unit: a hierarchical linear regression analysis
BMC Pediatrics (2023)
-
Relatives’ experiences of visiting restrictions during the COVID-19 pandemic’s first wave: a PREMs study in Valais Hospital, Switzerland
BMC Health Services Research (2023)
-
Perceived stress of mothers and fathers on two NICUs before and during the SARS-CoV-2 pandemic
Scientific Reports (2023)