
Abstract
Exposure to ultraviolet radiation (UVR) leads to skin DNA damage, specifically in the form of cyclobutane pyrimidine dimers, with thymidine dimers being the most common. Quantifying these dimers can indicate the extent of DNA damage resulting from UVR exposure. Here, a new liquid chromatography-mass spectrometry (LC–MS) method was used to quantify thymidine dimers in the urine after a temporary increase in real-life UVR exposure. Healthy Danish volunteers (n = 27) experienced increased UVR exposure during a winter vacation. Individual exposure, assessed via personally worn electronic UVR dosimeters, revealed a mean exposure level of 32.9 standard erythema doses (SEDs) during the last week of vacation. Morning urine thymidine dimer concentrations were markedly elevated both 1 and 2 days post-vacation, and individual thymidine dimer levels correlated with UVR exposure during the last week of the vacation. The strongest correlation with erythema-weighted personal UVR exposure (Power model, r2 = 0.64, p < 0.001) was observed when both morning urine samples were combined to measure 48-h thymidine dimer excretion, whereas 24-h excretion based on a single sample provided a weaker correlation (Power model, r2 = 0.55, p < 0.001). Sex, age, and skin phototype had no significant effect on these correlations. For the first time, urinary thymidine dimer excretion was quantified by LC–MS to evaluate the effect of a temporary increase in personal UVR exposure in a real-life setting. The high sensitivity to elevated UVR exposure and correlation between urinary excretion and measured SED suggest that this approach may be used to quantify DNA damage and repair and to evaluate photoprevention strategies.
Graphical abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
It is well established that exposure to sunlight is the main cause of skin cancer [1, 2]. Additionally, exposure to ultraviolet radiation (UVR) results in DNA damage in the form of cyclobutane pyrimidine dimers (CPDs) [3]. These dimers can be measured directly while they form within skin cells after exposure to UVR [3], and the mutations they may cause can result in keratinocyte carcinoma [4].
The most prominent of the CPDs, thymidine dimers [1, 5], were first detected in urine by Ahmad et al. [6] and have since been used to measure DNA repair following UVR exposure. In 2001, Le Curieux and Hemminki described a novel method involving 32P-postlabeling and high-performance liquid chromatography [7] that has been used to quantify thymidine dimers from urine in several studies [8,9,10]. The accessibility of analytical methods to perform these measurements has, however, been limited by the complexity of the 32P-postlabeling method. Recently, liquid chromatography-mass spectrometry (LC–MS) has greatly increased the practicality of CPD analyses [11,12,13].
This analytical method facilitates the measurement of urinary thymidine dimers produced in response to UVR and enables researchers to evaluate the influence of other variables such as exposure period, exposed skin area, sunscreen use, age, sex, and skin phototype. It also enables researchers to evaluate how various data correction methods, such as adjusting for creatinine concentration, may affect the correlation between UVR and the level of thymidine dimers in the urine.
In this study, the aim was to quantify thymidine dimers in urine using the new method previously described by Lerche et al. [11] and correlate them with personal UVR exposure in a natural setting. Healthy volunteers from Denmark were exposed to high-intensity ambient UVR during vacations in countries with high UV indexes. Volunteers wore personal wrist-borne UVR dosimeters during their vacations. Furthermore, we investigated whether various correction methods and individual variables, such as clothing, affected the relationship between measured UVR exposure and the thymidine dimers produced.
2 Materials and methods
2.1 Study design and subjects
The participants in this study were healthy volunteers living in the Copenhagen area of Denmark who were going on vacation in February 2023 to destinations with a generally higher UV index (5–11 +) than Denmark (UV index = 1). Destinations included Thailand, the Caribbean, the USA (Florida), and the Canary Islands. Inclusion criteria were as follows: age ≥ 18 years, vacation ≥ 1 week, and written informed consent.
Exclusion criteria were as follows: UVR exposure from a vacation or from using sun beds within 4 weeks prior to the study start, pregnancy, breastfeeding, immunosuppression, skin diseases, taking medication that interferes with DNA repair, or increased photosensitivity.
One urine sample was collected pre-holiday, while three subsequent samples were collected post-holiday. Before their vacation, participants were provided with a measuring cup to quantify the volume of their morning urine, and four 50 mL tubes were provided for storage of urine samples. The participants also received a personal UVR dosimeter to be worn on the wrist. In addition, the participants received data sheets to document their demographic data, urine sample volumes, and the time of urination immediately prior to providing the collected sample (which reflected the time over which the urine sample provided had been accumulating in the body). Furthermore, the participants were asked to keep a diary with information about their clothing and factor of sunscreen used over three 4-h time intervals (07:00–11:00 h, 11:00–14:00 h, and 14:00–18:00 h) during all days of their vacation. The documents given to the participants are shown in the supporting information section.
2.2 Chemicals
Thymidylyl-3′-5′-thymidine ammonium (Carbosynth Limited, Berkshire, UK), isotope-labeled (13C2) cis-syn-thymidine dimers (Toronto Research Chemicals, Toronto, ON, Canada), creatinine (Merck KGaA, Darmstadt, Germany), and isotope-labeled (D3) creatinine (Merck KGaA) were used.
2.3 Sample collection and preparation
Urine samples were collected on the morning of the last day before the vacation and on the first three mornings after returning from vacation. The urine samples were stored at − 18 °C in freezers at the homes of the volunteers before being transferred to the hospital. After transfer to the hospital, the samples were thawed, distributed into Eppendorf tubes, and stored at − 20 °C until analysis.
Because unlabeled standard of cis-syn-thymidine dimers was unavailable, 30 mg Thymidylyl-3′-5′-thymidine ammonium was dissolved in 15 mL water with 18 μL acetophenone. A total of 15 mL of this solution was irradiated with ultraviolet B in a UV 200 L cabin (Waldmann, Villingen-Schwenningen, Germany) for 3 h resulting in a mixture of thymidine photoproducts including cis-syn, trans-syn thymidine dimers, and the 6–4 photoproducts from TpT, similar to previously described methods [11, 14]. In the following cis-syn-thymidine dimers are abbreviated T<>T.
2.4 Ultra-performance liquid chromatography tandem mass spectrometry
2.4.1 T<>T analysis
The ultra-performance liquid chromatography tandem mass spectrometry (UPLC-MS/MS) method used here was adapted from a previously published method by Lerche et al. [11]. The UPLC-MS/MS analysis was performed on an Acquity UPLC I-Class system (Waters, Milford, MA, USA) coupled to a Xevo TQ-XS tandem quadrupole mass spectrometer (Waters, Manchester, UK) using an electrospray ionization interface as the ion source.
For the T<>T analysis, 180 µL of urine sample was mixed with 10 µL of 400 ng/mL isotopically labeled internal standard and 10 µL of water, resulting in a concentration of 20 ng/mL internal standard. Calibration plots were created using standard concentrations of 32 ng/mL, 16 ng/mL, 8 ng/mL, 4 ng/mL, 2 ng/mL, 1 ng/mL, 0.5 ng/mL, 0.25 ng/mL, and 0.125 ng/mL, by adding known concentrations of standards to blank urine. After mixing the samples, these were diluted with 1400 µL 1% formic acid and transferred to LC–MS vials for analysis with three technical replicates performed for each sample. A linear calibration plot was obtained for T<>T in the range 0.25–32 ng/mL, with R2 > 0.985.
The parameters for the mass spectrometer were set to the following values: source temperature, 150 °C; desolvation temperature, 650 °C; desolvation gas flow rate, 1000 L/h; cone gas flow rate, 150 L/h; capillary voltage, 0.5 kV; and detector gain, 1.
The LC separation was performed on an Atlantis Premier BEH C18 AX VanGuard FIT column (1.7 μm, 2.1 × 100 mm; Waters, Milford, MA, USA) at a temperature of 55 °C. The mobile phases consisted of (A) 0.2% formic acid in 10 mM ammonium formate and (B) methanol. Separation was performed with gradient elution from 0 to 50% B over 3 min, followed by a 2-min washing step with 98% B and re-equilibration to initial conditions for 1.5 min. For the analysis, the mass spectrometer was operated using multiple reaction monitoring in negative ion mode using the m/z 545 → 79 transition of the T<>T and the m/z 547 → 79 transition of the 13C-labeled internal standard; the cone voltage was set to 84 V and the collision energy to 48 eV.
2.4.2 Creatinine analysis
For the creatinine analysis, a urine sample was diluted 2500-fold in milliQ water. A total of 500 µL of the diluted sample was mixed with 500 µL 100 ng/mL deuterated internal standard to generate a 50 ng/mL internal standard solution. Calibration plots were created by diluting with water to generate standard solution concentrations of 800 ng/mL, 400 ng/mL, 200 ng/mL, 100 ng/mL, 50 ng/mL, 25 ng/mL, and 12.5 ng/mL. The diluted samples were transferred to LC–MS vials for analysis, with three technical replicates performed for each sample.
The parameters for the mass spectrometer were set to the following values: source temperature, 150 °C; desolvation temperature, 500 °C; desolvation gas flow rate, 1000 L/h; cone gas flow rate, 150 L/h; capillary voltage, 0.5 kV; and detector gain, 1.
The LC separation was performed at a temperature of 55 °C. The mobile phases consisted of (A) 0.2% formic acid in 10 mM ammonium formate and (B) methanol. Separation was performed by isocratic elution with 100% A over 2 min, followed by a 1-min washing step with 100% B and re-equilibration to initial conditions for 1 min. For the analysis, the mass spectrometer was operated using multiple reaction monitoring in positive ion mode using the m/z 114 → 44 transition of creatinine and the m/z 117 → 47 transition of the deuterated internal standard; the cone voltage was set to 40 V and the collision energy to 14 eV.
2.5 Personal UV radiation exposure
Personal UVR exposure during vacations was measured using wrist-borne dosimeters [15]. The dosimeters measured UVR exposure as standard erythema doses (SEDs) every 5 s and recorded a mean reading every 5 min. The UVR dosimeters (SunSaver 3, Bispebjerg Hospital, Copenhagen, Denmark) were updated models of a previous dosimeter [16] and they were calibrated [17] before the study. The action spectra for producing CPDs and erythema in human skin are very similar [18]; therefore, we assume a linear relationship exists between erythema-weighted UVR reaching the skin and CPD formation in the skin. To adjust for the different clothing worn by participants during the study period, exposed body surface areas (m2) were calculated using the diary information clothing codes provided by the participants and the corresponding exposed skin fraction, as previously described by Datta et al. [19].
2.6 Conversion and correction of data
2.6.1 UVR data
The measured personal UV dose in SEDs was converted to erythema-weighted Joules delivered to the skin by adjusting for exposed body surface area in m2.
To account for differences in the clothing worn by participants, these conversions were calculated separately for each of the three time slots in each day using the clothing codes recorded by participants and the following equation:
where SED represents the standard erythema dose, 1 SED = 100 J/m2 erythema weighted; BSA represents the body surface area. UV dose (J) represents erythema-weighted joule corrected for exposed skin area.
Further conversions were also applied to UV doses to account for self-reported sunscreen use. For this purpose, two different approaches were used:
1) Correction of UV dose using the labeled sun protection factor (SPF).
2) Effective SPF was calculated from the labeled SPF based on previous reports of sunscreen application thickness for Scandinavians going on a vacation in the sun [20], using the formula for effective SPF described by Petersen et al. (Effective SPF = labeled SPF0,79/2) [8]:
The UV doses were corrected for sunscreen use only when the participants had applied sunscreen to their bodies, not just to their faces.
2.6.2 T<>T data
To correctly correlate the measured T<>T concentrations with personal UVR exposure, the measured levels were corrected either by using (1) creatinine measurements or (2) reported urine volumes. For this purpose, three methods were used and compared:
1) Correction based on the urinary flow rate of the volunteers (calculated from urine volume and the time over which the urine sample provided had been accumulating in the body):
2) Correction for expected daily creatinine excretion based on metadata (sex, age, and weight):
†The expected quantity of creatinine was calculated using excretion data sourced from Kampmann et al. [21] based on weight, sex, and age.
3) Correction based on creatinine excretion as a ratio:
2.7 Statistical analysis
The statistical data analysis was performed using IBM SPSS statistical software (ver. 29; IBM, Armonk, NY, USA). Age, BSA, UV dose (SED), and UV dose (J) were tested for normal distribution using Kolmogorov–Smirnov Test and p values > 0.2; therefore, descriptive data are presented as means ± standard deviation. The optimal relationship (i.e., greatest r2 value) between the measured T<>T in the urine and personal UVR exposure follows a power model (double logarithmic) after testing linear, logarithmic, inverse, power, and exponential models. The UV doses were tested as accumulated UV doses for the last 3–10 vacations days, both with and without correction for sunscreen use. The urine post-vacation T<>T sample days were tested individually and as totals from days 1 and 2, and from days 1, 2, and 3. The effects of age, skin phototype, and sex were investigated using multiple regression analyses. All tests were two sided and a p value < 0.05 was considered statistically significant.
2.8 Ethics
This study was conducted in accordance with the Declaration of Helsinki. This study was approved by the Danish Research Ethics Committee (H-20076172), the Danish Knowledge Center for Data Reviews (P-2021-591), and it was registered on ClinicalTrials.gov (NCT05277961). Written informed consent was obtained from all participants.
3 Results
3.1 Assessment of UVR exposure and T<>T
A total of 27 healthy volunteers signed up for this study. Of these, one withdrew, one was excluded due to an error with the battery in their dosimeter, and three had nonvalid urine volume records. One participant did not deliver the pre-vacation urine sample. The 22 remaining participants received a mean of 32.7 SEDs (range 1.63–60.80) during the last 7 days of their vacation, according to the dosimeter readings (Table 1). An example of dosimeter readings collected from one of the volunteers is shown in Fig. 1. Age, BSA, UV dose (SED), and UV dose (J) were all normal distributed (Kolmogorov–Smirnoff test, p values > 0.2).

a Example of UVR measurements (SED/h) by the wrist-borne dosimeter during the last week of vacation for one of the volunteers; b measurement data from a specific day with 5-min mean values; c photograph showing the UVR dosimeter in use. UVR ultraviolet radiation, SED standard erythema dose
The presence of T<>T in the post-vacation urine was detected in 20 of the 22 volunteers (Fig. 2). The two participants without detectable T<>T in the post-vacation urine where those receiving the lowest UVR doses (below 5 SED during the last week of vacation—Table 1).

Concentration (ng/mL) of T<>T in urine measured by liquid chromatography-mass spectrometry. Black bars represent median values. Day 0 data represent morning urine collected on the day before the vacation and days 1–3 data represent morning urine collected on the first 3 days after returning to Denmark. Concentrations below 0.3 ng/mL were considered out of range and set to 0
Interestingly, two participants also had measurable levels of thymidine dimers in their urine samples before their departure. No apparent reason was found for the pre-vacation level of thymidine dimers, but upon returning from vacation, both participants showed increased levels of thymidine dimers in all three urine samples collected.
3.2 Association between UVR exposure and T<>T
In our investigation of the correlation between UVR exposure and urinary T<>T levels, we analyzed each method individually. Furthermore, we investigated the relationship between T<>T quantities in the post-vacation urine samples and different numbers of days of accumulated UVR exposure. The correlations were based on the measurements from the healthy volunteers who provided all necessary data (n = 22).
When the measured T<>T levels were adjusted by either of the two creatinine correction methods or by the urinary flow rate (calculated from urine volume and collection time), we found a significant association between the UV dose delivered to the skin and the quantity of T<>T excreted in urine. For all correction methods, the strongest correlations were found when a power model was used, and the strongest correlation overall was found when the quantities of T<>T in urine from days 1 and 2 post-vacation were combined and urinary flow rate was used to correct the T<>T quantities ([ ] Fig. 3a). Correlations were influenced by the number of vacation days used to calculate accumulated UVR exposure, with the best correlations observed when accumulated UVR exposure was calculated over the last 6–9 vacation days (Figs. 3, S2, S3). The best method for correcting T<>T quantities in the urine depended on how many of urine samples were included: Correction for expected creatinine excretion produced the best correlations when only day 1 post-vacation urine was measured (Fig. S3), whereas correction for urinary flow rate produced the best correlations when measurements combined post-vacation urine from days 1 and 2, or days 1–3 (Figs. 3, S2). Correlations were also assessed after adjusting UVR exposure for reported sunscreen using either the labeled SPF or the effective SPF. Adjusting UVR exposure using the labeled SPF substantially weakened correlations (Fig. S1), whereas assuming real-life thicknesses of sunscreen applied (i.e., effective SPF) resulted in correlations that were similar to those for unadjusted UVR (Figs. 3b, S2b, S3b).
] Fig. 3a). Correlations were influenced by the number of vacation days used to calculate accumulated UVR exposure, with the best correlations observed when accumulated UVR exposure was calculated over the last 6–9 vacation days (Figs. 3, S2, S3). The best method for correcting T<>T quantities in the urine depended on how many of urine samples were included: Correction for expected creatinine excretion produced the best correlations when only day 1 post-vacation urine was measured (Fig. S3), whereas correction for urinary flow rate produced the best correlations when measurements combined post-vacation urine from days 1 and 2, or days 1–3 (Figs. 3, S2). Correlations were also assessed after adjusting UVR exposure for reported sunscreen using either the labeled SPF or the effective SPF. Adjusting UVR exposure using the labeled SPF substantially weakened correlations (Fig. S1), whereas assuming real-life thicknesses of sunscreen applied (i.e., effective SPF) resulted in correlations that were similar to those for unadjusted UVR (Figs. 3b, S2b, S3b).

R2 values for the association between T<>T and the cumulative UV dose to the skin based on the number of vacation days: a R2 values for the association between total T<>T dimers measured on days 1 and 2 after the vacation and the cumulative UV dose to the skin for the last 3–10 days of the vacation; b R2 values for the association between total T<>T measured on days 1 and 2 after the vacati on and the cumulative effective SPF adjusted UV dose to the skin for the last 3–10 days of the vacation. SPF sun protection factor, BSA body surface area, SED standard erythema dose, UVR ultraviolet radiation
The correlations were of similar strength regardless of the correction (normalization) method applied to the T<>T quantities in the urine. However, steeper slopes were observed for correlations when unadjusted UVR exposure was used, whereas more gradual increases were observed when UVR exposure was adjusted for effective SPF (Fig. 4). Correlations were unaffected by skin phototype (p > 0.68), sex (p > 0.11), or age (p > 0.74). Figure 4 indicates a bias toward higher exposure doses. This is partly due to the nature of the double logarithmic plot. The test for normal distribution of the exposure doses is passed and for the UV dose adjusted for clothing and BSA an interquartile range from 1464 to 6402 with median of 5055 only indicates a bias toward higher values.

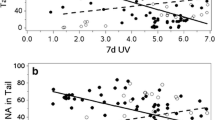
Associations between T<>T found in urine on days 1 and 2, and UV dose to the skin for the last 7 days of the vacation, based on different corrections for T<>T concentrations and ± adjustment of UV dose for effective SPF due to applied sunscreen. a T<>T (ng/48 h) on days 1 and 2, corrected for expected creatinine excretion. b T<>T (ng/48 h) on days 1 and 2, corrected for urinary flow rate. c mean ratio of T<>T/creatinine (nmol/mmol) for days 1 and 2. d T<>T (ng/48 h) on days 1 and 2, corrected for expected creatinine excretion; UV dose adjusted for effective SPF. e T<>T (ng/48 h) on days 1 and 2, corrected for urinary flow rate; UV dose adjusted for effective SPF. f Mean ratio of T<>T/creatinine (nmol/mmol) for days 1 and 2; UV dose adjusted for effective SPF. All correlations followed a power model (n = 22)
To evaluate the necessity of adjusting UVR exposure for exposed body surface, correlations were also tested using the SED measurements recorded by the dosimeters (Table 2). Compared with the adjusted UVR exposure levels, correlations obtained using the unadjusted SED measurements were generally weaker. However, these correlations were still significant and generally stronger than where UVR exposure was adjusted for sunscreen (Table 2).
4 Discussion
In this study, an LC–MS-based method was used for the first time to correlate DNA photoproducts excreted in urine with personal UVR exposure in a real-life setting. In addition, these T<>T results have been used in a qualitative intervention study to deliver biofeedback on personal risk perception, conducted in collaboration with the Danish Cancer Society (manuscript submitted for publication).
The method used in this study was able to measure DNA repair products in urine after personal UVR exposure, and increased levels of T<>T were observed in 20 of 22 study participants. Therefore, this method exhibited similar effectiveness to a method involving 32P-postlabeling that was previously described by Le Curieux and Hemminki [7] and to an LC–MS method described by Reynaud et al. [12] that was used to evaluate urine samples in 2023 [13]. The LC–MS method used in our study involves a much simpler sample preparation regimen with only dilution being required to pretreat the urine samples. By contrast, the LC–MS method described by Reynaud et al. relies on multiple sample preparation steps including solid-phase extractions, freeze drying, and 4 h of enzyme incubations to degrade thymidine dimer-containing oligonucleotides [12]. The enzymatic degradation of oligonucleotides may increase the quantity of photoproducts in samples [13], but this observation remains unconfirmed, and a correlation between the degradation products in urine and UVR exposure has not been demonstrated.
The correlations observed in this study follow a power model, similar to the relationship between UVR and thymidine dimers demonstrated in healthy volunteers after a vacation spent skiing or in the sun by Petersen et al. using a 32P-postlabeling method [8]. This is interesting since the studies are similar but differs in some important ways. Firstly, the TT dimers are measured by 2 very different methods. Secondly in the study by Petersen et al. the UVR exposure was measured by a special “UVB only” sensor in J/m2 [8], and in the current study, UVR was measured in SED. The correction for exposed BSA is also different. In the study by Petersen et al. the exposed BSA is expressed in percent recorded every 30 min [8], while this study only recorded clothing in 3 daily time intervals and used the individual exposed area in m2 for correction adjusting for differences in total BSA. If we assume a fixed factor for conversion of UVB doses to SED and only a small variation in the BSA of the participants in the study by Petersen et al., the slopes can be compared.
So despite these method differences, the slopes in the double logarithmic plots are very comparable: the study by Petersen et al. have a slope of 0.92 and our slope is 0.865 for TT dimer on day 1 using Kampmann et al. [21] for creatinine correction (Fig. 4a shows the relation between day 1 + day 2 TT dimers and UVR exposure to the skin).
We also found that correction of T<>T excretion for either creatinine excretion or urinary flow rate gave similar results and produced significant correlations with UVR exposure. Indeed, urinary flow rate produced the strongest correlations when the quantities of T<>T in post-vacation urine samples from days 1 and 2 (Fig. 3) or days 1, 2, and 3 (Fig. S2) were combined. This suggests that creatinine correction is not necessary if the urine volume and the time of urination immediately prior to providing the collected sample are carefully recorded by study participants. The urinary flow rate method may be particularly advantageous in studies with limited laboratory time or capacity.
Interestingly, when dimer quantities were corrected as ratios of creatinine concentration, similar correlations were observed, indicating that participant metadata and urine volumes may not be necessary to achieve viable T<>T results. This could considerably reduce both the workload and the risk of participant recording errors in future clinical studies, because participants would not be required to provide data.
The third correction method applied to the T<>T measurements was for expected creatinine excretion, which was calculated using the study participants’ ages, weights, and sex, based on reference data from Kampmann et al. [21]. Using this method, the strongest correlation between UVR exposure and urinary T<>T was observed when only the first post-vacation urine sample was measured (Fig. S3). This method requires more metadata from study participants and the results were not substantially better than those obtained using the creatinine ratio method. However, despite the greater uncertainty and necessity for participant records and analyses, this method may have important advantages. In particular, our study population was small, with all participants aged from 35 to 55 years and we had twice as many females than males. More heterogeneous study populations may necessitate more substantial adjustments to the T<>T quantities. Variation in urinary T<>T by age or sex may indicate differences in the efficiency and/or kinetics of NER pathways which would be of great interest as it could therefore relate to skin cancer risk.
Although the personal wrist-borne UVR dosimeters enabled us to collect continuous UVR exposure data [16], numerous variables may impact the UVR dosages received by the study participants. Importantly, the requirements and instructions for completing vacation diaries were minimized to maximize participant compliance. There was an inherent risk of bias associated with reporting the clothing codes. Clothing codes were registered by the participants during the vacation; however, it was only possible to register one code in an interval of 4 h. In addition, the participants were asked to record their use of sunscreen, to evaluate the extent to which sunscreen application might affect the correlations; such data collected in real-life settings are currently lacking [24].
The impact of sunscreen use was assessed when UVR exposure was adjusted either for the labeled SPF or the effective SPF. Adjusting for the labeled SPF substantially weakened the correlation between UVR exposure and urinary T<>T. Adjusting for effective SPF, also slightly weakened this correlation but it remained significant and similar to the correlation between unadjusted UVR exposure and urinary T<>T. Therefore, the model used to calculate effective SPF that was described by Petersen et al. [8] was effective, but the adjustment did not increase the correlation with urinary T<>T.
A recent study by Douki et al. found differences in the levels of urinary thymidine dimers measured in people who were educated in the use of sunscreen, compared to an uneducated group of people [13]. Therefore, sunscreen application may have had a greater effect on the correlations we measured if our participants had received instructions on how to apply it correctly. However, Douki et al. [13] collected general UVR exposure data, in contrast to using a dosimeter that accounts for personal behavior. Therefore, effectiveness of sunscreen is difficult to assess in the study by Douki et al. [13].
Although adjusting for sunscreen weakened the correlation between UVR exposure and urinary T<>T, adjusting for clothes and exposed body surface area strengthened this correlation. However, the increase was not as substantial as expected, and correlations between urinary T<>T and unadjusted UVR exposure were also significant. This may be because people on vacation in the sun wear similar clothing, which may decrease the relative effect of adjusting UVR exposure for covering by clothes. Interestingly, introducing the potential for human error by asking participants to record their levels of protection by clothes or sunscreen is unnecessary to achieve good correlations between UVR exposure and urinary T<>T dimers.
One difficulty in correlating UV doses with excretion of thymidine dimers in the urine may arise due to different lengths of the vacations: the effect of prolonged UVR exposure on urinary T<>T is currently unknown. Previous studies have shown that thymidine dimer excretion after single exposures to UVR is greatest 3–5 days after the last UVR exposure [11, 25, 26]. Interestingly, the correlations in our study were markedly stronger when UVR exposure periods of 6–9 days rather than 3–5 days were used. Therefore, although the greatest quantities of urinary T<>T may be excreted after a few days, UVR exposure prior to this can have a significant impact on the overall quantities of urinary T<>T.
Another limitation of our study was that skin phototypes were self-reported according to the guide in the supporting information section instead of pigment being measured objectively [27]. Furthermore, differences in traveling time on return journeys and the time of day on arrival may substantially alter the time from the last UVR exposure on vacation to the first post-vacation morning urine sample.
Despite these limitations and general biological variation, the LC–MS method demonstrated a significant correlation between urinary T<>T and real-life UVR exposure. The effectiveness and simplicity of this method suggests that T<>T in urine may be used as a noninvasive marker for UVR derived DNA damage and repair. Furthermore, we obtained important information regarding the necessity of various adjustments for UVR exposure, and corrections for measuring urinary T<>T. Future simple studies could be designed using the last 7 days UVR exposure and then 2 days of urine collection for T<>T analysis.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Ananthaswamy, H. N. (2001). Sunlight and skin cancer. Journal of Biomedicine & Biotechnology, 1, 49.
Ghissassi, F. E., Baan, R., Straif, K., et al. (2009). A review of human carcinogens—part D: Radiation. The lancet Oncology, 10, 751–752.
Douki, T., Court, M., Sauvaigo, S., Odin, F., & Cadet, J. (2000). Formation of the main UV-induced thymine dimeric lesions within isolated and cellular DNA as measured by high performance liquid chromatography-tandem mass spectrometry. Journal of Biological Chemistry, 275, 11678–11685.
Reardon, J. T., & Sancar, A. (2003). Recognition and repair of the cyclobutane thymine dimer, a major cause of skin cancers, by the human excision nuclease. Genes & Development, 17, 2539–2551.
Mouret, S., Baudouin, C., Charveron, M., Favier, A., Cadet, J., & Douki, T. (2006). Cyclobutane pyrimidine dimers are predominant DNA lesions in whole human skin exposed to UVA radiation. Proceedings of the National Academy of Sciences, 103, 13765–13770.
Ahmad, J., Cooke, M. S., Hussieni, A., Evans, M. D., Patel, K., Burd, R. M., Bleiker, T. O., Hutchinson, P. E., & Lunec, J. (1999). Urinary thymine dimers and 8-oxo-2’-deoxyguanosine in psoriasis. FEBS Letters, 460, 549–553.
Le Curieux, F., & Hemminki, K. (2001). Cyclobutane thymidine dimers are present in human urine following sun exposure: Quantitation using 32P-postlabeling and high-performance liquid chromatography. The Journal of Investigative Dermatology, 117, 263–268.
Petersen, B., Wulf, H. C., Triguero-Mas, M., et al. (2014). Sun and ski holidays improve vitamin D status, but are associated with high levels of DNA damage. The Journal of Investigative Dermatology, 134, 2806–2813.
Liljendahl, T. S., Blomqvist, A., Andersson, E. M., Barregard, L., & Segerbäck, D. (2013). Urinary levels of thymine dimer as a biomarker of exposure to ultraviolet radiation in humans during outdoor activities in the summer. Mutagenesis, 28, 249–256.
Narbutt, J., Philipsen, P. A., Lesiak, A., et al. (2018). Children sustain high levels of skin DNA photodamage, with a modest increase of serum 25-hydroxyvitamin D3, after a summer holiday in Northern Europe. British Journal of Dermatology, 179, 940–950.
Lerche, C. M., Philipsen, P. A., Hermansson, S., Heydenreich, J., & Wulf, H. C. (2022). Quantification of urinary thymidine dimers in volunteers after ultraviolet radiation using a new UPLC-MS/MS-based method. Anticancer Research, 42, 5069.
Reynaud, N., Belz, L., Béal, D., Bacqueville, D., Duplan, H., Géniès, C., Questel, E., Josse, G., & Douki, T. (2022). DNA photoproducts released by repair in biological fluids as biomarkers of the genotoxicity of UV radiation. Analytical and Bioanalytical Chemistry, 414, 7705–7720.
Douki, T., Caillat, S., Bacqueville, D., et al. (2023). Nuclear and urinary measurements show the efficacy of a SPF50+ sunscreen against DNA photoproducts upon “real-life” recreational exposure. JID Innovation. https://doi.org/10.1016/j.xjidi.2023.100227
Felton, S. J., Cooke, M. S., Kift, R., Berry, J. L., Webb, A. R., Lam, P. M. W., de Gruijl, F. R., Vail, A., & Rhodes, L. E. (2016). Concurrent beneficial (vitamin D production) and hazardous (cutaneous DNA damage) impact of repeated low-level summer sunlight exposures. British Journal of Dermatology, 175, 1320–1328.
Thieden, E., Agren, M. S., & Wulf, H. C. (2000). The wrist is a reliable body site for personal dosimetry of ultraviolet radiation. Photodermatology, Photoimmunology and Photomedicine, 16, 57–61.
Heydenreich, J., & Wulf, H. C. (2019). Personal electronic UVR dosimeter measurements: Specific and general uncertainties. Photochemical & Photobiological Sciences, 18, 1461–1470.
Heydenreich, J., & Wulf, H. C. (2005). Miniature personal electronic UVR dosimeter with erythema response and time-stamped readings in a wristwatch. Photochemistry and Photobiology, 81, 1138–1144.
Young, A. R., Chadwick, C. A., Harrison, G. I., Nikaido, O., Ramsden, J., & Potten, C. S. (1998). The similarity of action spectra for thymine dimers in human epidermis and erythema suggests that DNA is the chromophore for erythema. The Journal of Investigative Dermatology, 111, 982–988.
Datta, P., Philipsen, P. A., Idorn, L. W., & Wulf, H. C. (2021). Low vitamin D in dark-skinned immigrants is mainly due to clothing habits and low UVR exposure: A Danish observational study. Photochemical & Photobiological Science Official Journal of European Photochemical Association European Society of Photobiology, 20, 1573–1584.
Petersen, B., Datta, P., Philipsen, P. A., & Wulf, H. C. (2013). Sunscreen use and failures—on site observations on a sun-holiday. Photochemical & Photobiological Sciences, 12, 190–196.
Kampmann, J., Siersbæk-Nielsen, K., Kristensen, M., & Hansen, J. M. (1974). Rapid evaluation of creatinine clearance. Acta Medica Scandinavica, 196, 517–520.
Mosteller, R. D. (1987). Simplified calculation of body-surface area. New England Journal of Medicine, 317, 1098–1098.
Fitzpatrick, T. B. (1988). The validity and practicality of sun-reactive skin types I through VI. Archives of Dermatology, 124, 869–871.
Paul, S. P. (2019). Ensuring the safety of sunscreens, and their efficacy in preventing skin cancers: challenges and controversies for clinicians, formulators, and regulators. Frontiers in Medicine, 6, 195.
Cooke, M. S., Evans, M. D., Burd, R. M., Patel, K., Barnard, A., Lunec, J., & Hutchinson, P. E. (2001). Induction and excretion of ultraviolet-induced 8-oxo-2′-deoxyguanosine and thymine dimers in vivo: Implications for PUVA. The Journal of Investigative Dermatology, 116, 281–285.
Kotova, N., Hemminki, K., & Segerbäck, D. (2005). Urinary thymidine dimer as a marker of total body burden of UV-inflicted DNA damage in humans. Cancer Epidemiology, Biomarkers & Prevention, 14, 2868–2872.
Ravnbak, M. H. (2010). Objective determination of Fitzpatrick skin type. Danish Medical Bulletin, 57, B4153.
Funding
Open access funding provided by Copenhagen University. This research was supported by the Danish Research Center for Skin Cancer, Denmark (https://vfhk.org/en), Copenhagen University Hospital, Bispebjerg and Frederiksberg, Copenhagen, Denmark and by the Lundbeck Foundation, Copenhagen, Denmark (R307-2018-3318). This work was executed as a part of the Skin Cancer Innovation Clinical Academic Group (SCIN CAG), Greater Copenhagen Health Science Partners (https://gchsp.dk/en/).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Jonatan Riber Granborg, Peter Alshede Philipsen, and Catharina Margrethe Lerche. The first draft of the manuscript was written by Catharina Lerche and Jonatan Granborg and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lerche, C.M., Frederiksen, N.J.S., Thorsteinsson, I.S. et al. Urinary thymidine dimer excretion reflects personal ultraviolet radiation exposure levels. Photochem Photobiol Sci 23, 919–930 (2024). https://doi.org/10.1007/s43630-024-00563-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43630-024-00563-0