
Abstract
Background
The loss of the viscoelastic properties of central arteries independently of blood pressure loads could stimulate the development of left ventricular hypertrophy and dysfunction, renal failure, or cerebral vascular injury.
Objective
The aim of the present study is to determine if an elevated systolic aortic pressure is a marker of more frequent target organ damage (TOD) in hypertensive low cardiovascular risk (CVR) patients.
Methods
Hypertensive non treated consecutive patients (p) assisted at first visit in a specialized center with a CVR according to WHO Americas B area score less than 10 % were included. Left ventricular mass index (LVMI) and tissue Doppler diastolic and systolic function were measured as Lang et al. (J Am Soc Echocardiogr 18:1440–1463, 2005) and Nagueh et al. (J Am Soc Echocardiogr 22:107–133, 2009). Cardiac TOD was considered according to 2013 European Society of Hypertension/European Society of Cardiology. Glomerular filtration rate (GFR) was calculated by MDRD formula, a value <60 ml/min/1.73 m2 was considered TOD. Systolic aortic pressured (CAoP) was measured by radial tonometry and classified according to criteria proposed by Herbert et al. (Eur Heart J 35:3100–3132, 2014). Continue variables are reported as means with standard deviation and discrete variables as absolute values and percentages. Statistical analysis was performed with Students t test, significant differences were considered with a p value < 0.05
Results
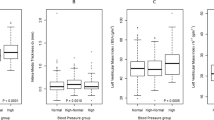
155 p were included; 23 p (14.8 %) had elevated CAoP while 132 p (85.2 %) had normal CAoP. Sample mean age was 54.1 + 12.9 years; 85 p (54.8 %) were males. Dyslipidemia was detected in 44 p (28.4 %), and 18 p (11.6 %) were smokers. Mean blood pressure was 143.7 + 17.1 mmHg/86.4 + 12.3 mmHg in p with normal (n) CAoP and 140.3 + 12 mmHg/81.9 + 6.8 mmHg in p with CAoP elevated e (p = NS). Mean CAoP in p with normal values was 117.4 + 10.9 mmHg and 116.9 + 10.7 in p with elevated values (p = NS). The average s wave was 7.42 + 1 cm/sec in n CAoP p vs 6.6 + 1 cm/sec in e CAoP p (p < 0.05) while and E/e′ ratio >13 was detected in 14.4 % n CAoP p vs 8.7 % e CAoP p (p = NS). Mean GFR was 105.4 + 40.5 ml/min/1.73 m2 in n CAoP p vs 103.9 + 45.6 ml/min/1.73 m2 in e CAoP p (p = NS) and GFR <60 ml/min/1.73 m2 was present in 4.5 % n CAoP p vs 26.1 % e CAoP p (p < 0.0125).
Conclusions
At the same level of CVR according to WHO Americas B score patients with elevated CAoP had lower longitudinal left ventricular systolic function and renal function was more deteriorated.

Similar content being viewed by others


References
Vlachopoulos K, Aznaouridis C. Stefanadis. Clinical appraisal of arterial stiffness: the Argonauts in front of the Golden Fleece. Heart. 2006;92:1544–50.
Palatini P, Casiglia E, Gąsowski J, Głuszek J, Jankowski P, Narkiewicz K, Saladini F, Stolarz-Skrzypek K, Tikhonoff V, Van Bortel L, Wojciechowska W, Kawecka-Jaszcz K. Arterial stiffness, central hemodynamics, and cardiovascular risk in hypertension. Vasc Health Risk Manag. 2011;7:725–39.
O’Rourke MF, Safar ME, Dzau V. The Cardiovascular Continuum extended: aging effects on the aorta and microvasculature. Vasc Med. 2010;15:461–8.
Miljkovic D, Perret-Guillaume C, Alla F, Salvi P, Erpelding ML, Benetos A. Correlation between peripheral blood pressure and pulse-wave velocity values in the institutionalized elderly persons 80 years of age and older: The PARTAGE Study. Am J Hypertens. 2013;26:163–73.
Laurent S, Cockcroft J, Van Bortel L, Boutouyrie P, Giannattasio C, Hayoz D, Pannier B, Vlachopoulos C, Wilkinson I, Struijker-Boudier H, European Network for Non-Invasive Investigation of Large Arteries. Expert concensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J. 2006;27:2588–605.
Vlachopoulos C, Aznaouridis K, O’Rourke MF, Safar ME, Baou K, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with central haemodynamics: a systematic review and meta-analysis. Eur Heart J. 2010;31:1865–71.
Vlachopoulos C, Aznaouridis K, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysis. J Am Coll Cardiol. 2010;55:1318–27.
Mancia G, Fagard R, Narkiewicz K, Redón J, Zanchetti A, Böhm M, Christiaens T, Cifkova R, De Backer G, Dominiczak A, Galderisi M, Grobbee DE, Jaarsma T, Kirchhof P, Kjeldsen SE, Laurent S, Manolis AJ, Nilsson PM, Ruilope LM, Schmieder RE, Sirnes PA, Sleight P, Viigimaa M, Waeber B, Zannad F, Task Force Members. 2013 ESH/ESC Guidelines for the management of arterial hypertension. The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2013;31:1281–357.
Weber MA, Schiffrin EL, White WB, Mann S, Lindholm LH, Kenerson JG, Flack JM, Carter BL, Materson BJ, Ram CV, Cohen DL, Cadet JC, Jean-Charles RR, Taler S, Kountz D, Townsend R, Chalmers J, Ramirez AJ, Bakris GL, Wang J, Schutte AE, Bisognano JD, Touyz RM, Sica D, Harrap SB. Clinical practice guidelines for the management of hypertension in the community: a statement by the American Society of Hypertension and the International Society of Hypertension. J Hypertens. 2014;32:3–15.
World Health Organization. Prevention of Cardiovascular Disease Guidelines for assessment and management of cardiovascular risk. http://www.who.int/cardiovascular_diseases/publications/Prevention_of_Cardiovascular_Disease/en/. Accessed 24 Aug 2007.
Herbert A, Cruickshank JK, Laurent S, Boutouyrie O, on behalf of The Reference Values for Arterial Measurements Collaboration. Establishing reference values for central blood pressure and its amplification in general healthy population and according to cardiovascular risk factor. Eur Heart J. 2014;35:3122–32.
Piskorz D, Tommasi A. La disfunción diastólica en pacientes hipertensos no es debida a hipertrofia ventricular izquierda. Ins Card. 2011;6:2–7.
Devereux RB, Alonso DR, Lutas EM, Gottlieb GJ, Campo E, Sachs I, Reichek N. Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. Am J Cardiol. 1986;57:450–8.
Devereux RB, Pini R, Aurigemma GP, Roman MJ. Measurement of left ventricular mass: methodology and expertise. J Hypertens. 1997;15:801–9.
Lang RM, Biering M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, Picard MH, Roman MJ, Seward J, Shanewise JS, Solomon SD, Spencer KT, Sutton MS, Stewart WJ, Chamber Quantification Writing Group, American Society of Echocardiography’s Guidelines and Standards Committee, European Association of Echocardiography. Recommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005;18:1440–63.
Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA, Waggoner AD, Flachskampf FA, Pellikka PA, Evangelista A. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. J Am Soc Echocardiogr. 2009;22:107–33.
Piskorz D, Bongarzoni L, Citta L, Citta N, Citta P, Keller L, Tommasi A. Association of systolic dysfunction with left ventricular hypertrophy and diastolic dysfunction in hypertensive patients. Rev Fac Cien Med Univ Nac Cordoba. 2014;71:158–64.
Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med. 1999;130:461–70.
Roman MJ, Devereux RB, Kizer JR, Okin PM, Lee ET, Wang W, Umans JG, Calhoun D, Howard BV. High central pulse pressure is independently associated with adverse cardiovascular outcome: the Strong Heart study. J Am Coll Cardiol. 2009;54:1730–4.
Booysen HL, Norton GR, Maseko MJ, Libhaber CD, Majane OHI, Sareli P, Woodiwiss AJ. Aortic, but not brachial blood pressure category enhances the ability to identify target organ changes in normotensives. J Hypertens. 2013;31:1124–30.
McEniery C, Barry McDonnell Y, Munnery M, Wallace SM, Rowe CV, Cockcroft JR, Wilkinson IB, Anglo-Cardiff Collaborative Trial Investigators. Central pressure: variability and impact of cardiovascular risk factors: The Anglo-Cardiff Collaborative Trial II. Hypertension. 2008;51:1476–82.
Wang KL, Cheng HM, Chuang SY, Spurgeon HA, Ting CT, Lakatta EG, Yin FC, Chou P, Chen CH. Central or peripheral systolic or pulse pressure: which best relates to target organs and future mortality? J Hypertens. 2009;27:461–7.
Roman MJ, Okin PM, Kizer JR, Lee ET, Howard BV, Devereux RB. Relations of central and brachial blood pressure to left ventricular hypertrophy and geometry: the Strong Heart Study. J Hypertens. 2010;28:384–8.
Chirinos JA, Segers P, Gillebert TC, Gupta AK, De Buyzere ML, De Bacquer D, St John-Sutton M, Rietzschel ER, on behalf of the Asklepios Investigators. Arterial properties as determinants of time-varying myocardial stress in humans. Hypertension. 2012;60:64–70.
Kraigher-Krainer E, Shah AM, Gupta DK, Santos A, Claggett B, Pieske B, Zile MR, Voors AA, Lefkowitz MP, Packer M, McMurray JJ, Solomon SD. PARAMOUNT Investigators Impaired systolic function by strain imaging in heart failure with preserved ejection fraction. JACC. 2014;63:447–56.
Shah AM, Solomon SD. Phenotypic and pathophysiological heterogeneity in heart failure with preserved ejection fraction. Eur Heart J. 2012;33:1716–7.
Totaro S, Khoury PR, Kimball TR, Dolan LM, Urbina EM. Arterial stiffness is increased in young normotensive subjects with high central blood pressure. J Am Soc Hypertens. 2015;9:285–92.
Chirinos JA, Segers P, Rietzschel ER, De Buyzere ML, Raja MW, Claessens T, De Bacquer D, St. John-Sutton M, Gillebert TC, on behalf of the Asklepios Investigators, Early and late systolic wall stress differentially relate to myocardial contraction and relaxation in middle-aged adults. The Asklepios Study. Hypertension. 2013;61:296–303.
Woodard T, Sigurdsson S, Gotal JD, Torjesen AA, Inker LA, Aspelund T, Eiriksdottir G, Gudnason V, Harris TB, Launer LJ, Levey AS, Mitchell GF. Mediation analysis of aortic stiffness and renal microvascular function. J Am Soc Nephrol. 2014. doi:10.1681/ASN.20140504501.
Mitchell GF. Central pressure should not be used in clinical practice. Artery Res. 2015;9:8–13.
Williams B, Lacy PS, Thom SM, Cruickshank K, Stanton A, Collier D, Hughes AD, Thurston H, O’Rourke M, The CAFE Investigators, for the Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT) Investigators. Differential impact of blood pressure-lowering drugs on central aortic pressure and clinical outcomes. Principal results of the Conduit Artery Function Evaluation (CAFE) Study. Circulation. 2006;113:1213–25.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Piskorz, D., Bongarzoni, L., Citta, L. et al. Functional Organ Damage in Cardiovascular Low Risk Patients with High Central Aortic Pressure. High Blood Press Cardiovasc Prev 22, 281–287 (2015). https://doi.org/10.1007/s40292-015-0105-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40292-015-0105-4