
Abstract
Cerebral blood flow (CBF) autoregulation (AR) can be monitored using invasive modalities, such as intracranial pressure (ICP) and arterial blood pressure (ABP) to calculate the CBF AR index (PRx). Monitoring PRx can reduce the extent of secondary brain damage in patients. Rheoencephalography (REG) is an FDA-approved non-invasive method to measure CBF. REGx, a CBF AR index, is calculated from REG and arm bioimpedance pulse waves. Our goal was to test REG for neuromonitoring. 28 measurement sessions were performed on 13 neurocritical care patients. REG/arm bioimpedance waveforms were recorded on a laptop using a bioimpedance amplifier and custom-built software. The same program was used for offline data processing. Case #1: The patient’s mean REGx increased from − 0.08 on the first day to 0.44 on the second day, indicating worsening intracranial compliance (ICC) (P < 0.0001, CI 0.46–0.58). Glasgow Coma Scale (GCS) was 5 on both days. Case #2: REGx decreased from 0.32 on the first recording to 0.07 on the last (P = 0.0003, CI − 0.38 to − 0.12). GCS was 7 and 14, respectively. Case #3: Within a 36-minute recording, REGx decreased from 0.56 to − 0.37 (P < 0.0001, 95%, CI − 1.10 to − 0.76). Central venous pressure changed from 14 to 9 mmHg. REG pulse wave morphology changed from poor ICC to good ICC morphology. Bioimpedance recording made it possible to quantify the active/passive status of CBF AR, indicate the worsening of ICC, and present it in real time. REGx can be a suitable, non-invasive alternative to PRx for use in head-injured patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
1.1 Neuromonitoring
Computerized monitoring of neurocritical care patients is in practice already. An additional improvement is if invasive methods can change to noninvasive. Our hypothesis is that the use of the bioimpedance technique can serve this principle. Clinical relevance is to have the same information without the risk of the invasive method, which can be caused by drilling a hole in the skull to implant a pressure sensor. On the battlefield, the principal causes of death within the first hour of injury among Service Members are hemorrhage and traumatic brain injury (TBI) [1]. Hypoxemia and hypotension are two considerable factors with poor prognosis in severe TBI patients and the prehospital setting [2]. In the civilian population, TBI is the most common cause of death under the age of 40 [3,4,5]. The objective of neuromonitoring is to prevent secondary brain damage due to raised ICP and decreased CBF. Elevated ICP can be due to stroke, edema formation, hypoxia, and vasospasm [6]. Invasive devices used in neuromonitoring include probes for monitoring ICP, brain tissue partial O2 pressure, temperature, CBF, and tissue perfusion [7, 8]. Noninvasive modalities include infrared spectroscopy (NIRS), transcranial Doppler (TCD), and neurophysiological methods [9]. Brain imaging methods are not suitable for continuous monitoring, they require technician’s support, they are large equipment, and they need for transporting the critically ill patient. And they are expensive. Brain imaging was designed for localizing morphological abnormalities of the brain and not for continuous monitoring. Ideally, neuromonitoring tools should be noninvasive, continuous, reliable, accurate, predictive for the outcome, and convenient both for patients and medical staff to apply. Continuous, but invasive neuromonitoring is available with ICM + software by calculating PRx [10].
1.2 ICP
The clinical importance of ICP monitoring was detailed here [7]. Normal ICP waveforms have 3 peaks: P1 = percussion wave, which represents arterial pulsation; P2 = tidal wave, which represents intracranial compliance (ICC); and P3 = dicrotic wave, which represents aortic valve closure and venous pulsations. In a normal waveform, P1 is the highest peak resulting in a “P1 > P2” or “good ICC” morphology [11,12,13,14]. In the case of a “poor ICC waveform”, P2 is higher than P1 (P2 > P1), indicating compromised ICC. An additional worsening of ICC results in a “triangle shape waveform” where P2 > P1 and P3 result in the 3 waves fusing into a triangular shape. In this publication, we use REG peak labeling identical to that used for ICP pulse waves [14, 15]. The magnitude of the ICP pulse waveform is traditionally associated with the steepness of the pressure-volume (compliance) curve - the steeper it is, the lower the compensatory reserve and the greater the ICP pulse amplitude [15]. Decreased ICC is a life-threatening condition; that can cause a herniation. Brain herniation occurs when something inside the skull produces pressure that moves brain tissues. This is most often the result of brain swelling or bleeding from a head injury, stroke, or brain tumor. When herniation occurs, it further lowers the chance of recovery. The outlook varies, depending on where in the brain the herniation occurs. Without treatment, death is likely. There can be damage to parts of the brain that control breathing and blood flow.
1.3 Cerebral blood flow autoregulation
When used in the context of cerebral circulation, CBF AR [16] generally refers to the capacity of CBF to remain relatively constant despite variations in cerebral perfusion pressure (CPP), the difference between mean arterial pressure (MAP), and ICP. Without AR, CBF would increase or decrease, with possible cerebral ischemia or edema, whenever the CPP increases or decreases. Thus, AR in cerebral circulation may be defined more pragmatically as the mechanism that protects the brain against the dangers of hypoxia at low perfusion pressures and against the risks of brain edema at high arterial pressures [17]. The organ of CBF AR is the arteriole and not the large artery which limits the usefulness of TCD in assessing CBF AR [18, 19]. To prevent secondary brain injury, the goal of neuromonitoring is to achieve early detection of decreased CBF subsequently leading to early intervention (to increase cerebral perfusion pressure). The clinical importance of CBF AR monitoring was presented here [20]. NB: Heart activity-related monitoring does not give the essential information: cessation of CBF or the lower limit of CBF AR (when CBF AR turns to passive from active) [17]. Hypotensive resuscitation or permissive hypotension is a resuscitation strategy used in trauma care. It is a resuscitation strategy that uses limited fluids and blood products during the early stages of treatment for hemorrhagic shock. Lower-than-normal blood pressure is maintained until operative control of the bleeding can occur. However, even brief episodes of hypotension occurring in the initial phase of resuscitation are significantly associated with increased mortality following brain injury [21]. Patients with brain injury have compromised CBF AR. There is no non-invasive way to assess the risk of implementing a hypotensive resuscitation strategy on AR in brain-injured patients. The pressure reactivity index, PRx [10] uses an advanced measurement algorithm to calculate a correlation of the coefficient between slow spontaneous changes in ICP and ABP [20]. A positive index (positive correlation, + 1) implies impaired cerebral autoregulation, while a negative index (inverse correlation, − 1) implies intact AR. PRx > 0.3 is considered the warning threshold (red line) for impaired cerebral compliance. Disturbance in the pressure reactivity index may be associated with bad outcomes [20]. NB: both ICP and ABP measurements are invasive. It is desirable to substitute them with noninvasive modalities. REG can fill that crucial role.
1.4 Rheoencephalography
The US Food and Drug Administration (FDA) defines REG as “a device used to estimate a patient’s cerebral circulation (blood flow in the brain) by electrical impedance methods with direct electrical connections to the scalp or neck area” [22]. REG pulse wave has a similar morphology to ABP or ICP waveforms. The physical basis of the REG measurement is that blood and cerebrospinal fluid are better conductors than the brain or other “dry” tissue. There are 4 and 2 electrode systems. Four electrode devices can measure total impedance as well as pulsatile impedance. Two electrode devices typically measure pulsatile components only, which represent a small percentage of total impedance. During blood inflow into the cranial cavity, electrical conductivity increases, and resistance decreases, as represented by increasing REG pulse amplitude [23]. REG pulse wave looks like an inverted arterial pulse wave at the output of a bioimpedance amplifier. Since REG is an impedance signal, its units are in Ohm. However, after the digital recording of the REG signal, its unit is in Volt. REG measurement is noninvasive in humans. Few studies have compared the results of measurements made with REG to measurements of invasive ICP [24,25,26,27,28,29]. In vitro study established a correlation between bioimpedance and fluid flow/volume signals [30]. Influencing factors of REG pulse waves (ICP, ABP, etc.) were detailed previously [31]. REG pulse wave rising portion called anacrotic time (from minimum to maximum) was described as pathologic, typical for cerebrovascular (arteriosclerotic) disease [25, 32]. Anacrotic time was considered arteriosclerotic if it was > 180 msec, based on Jenkner’s data [32]. A close correlation between PRx and REGx was established determining the lower limit of CBF AR between ICP and REG. If the PRx calculation uses REG instead of ICP, it is called REGx [28]. In this publication, the physiological basis of REG and ICP equivalency is demonstrated: the ICP slow waves are recapitulated in the REG and both are in opposite phases to ABP.
We hypothesized that (1) CBF AR (REGx) can calculate from REG and arm bioimpedance pulse waves. (2) REG pulse wave morphology would detect changes in intracranial compliance similarly to ICP.
2 Methods and patients
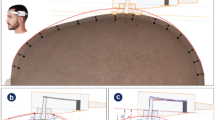
Bioimpedance/REG pulse wave measurements on neurocritical care patients started after local IRB approval in 2018 but halted in 2020 because of safety concerns regarding the Covid-19 pandemic. Patients or their families consented to participate after being informed of what the study would entail and its potential risks. Our ClinicalTrials.gov Identifier is NCT05170295 (December 27, 2021). Patients’ diagnoses included the following: Ischemic Stroke (IS), Subarachnoid Hemorrhage (SAH), Intracerebral Hemorrhage (traumatic and non-traumatic—ICH-T and ICH-NT), Hydrocephalus HCP), Intracranial Mass (tumor). Thirteen patients were measured 28 times, some repeatedly; twenty-three recordings were analyzed. The main age was 56.75 ± 16.11 years. The number of female patients was 7 and the males were 6. The mean recording time was 84.05 ± 44.73 min. Seven patients had an external ventricular drain (EVD). Before electrode placement, the skin surface was cleaned with alcohol and allowed to dry. REG/bioimpedance signals were recorded by using traditional ECG electrodes, placed on the frontotemporal area. Arm bioimpedance electrodes were placed on the left lower arm above the wrist and below the elbow. Traditional ECG electrodes were used on the arm, or fabric band circumferential electrodes (Hi-Meg, Velcro, Manchester, NH). Recordings were performed while patients were in bed, conscious or unconscious in the supine position. The REG/bioimpedance bipolar amplifier was part of the Cerberus system (Quintlab, Budapest, Hungary) used to generate bioimpedance pulse waves [33]. For analog-digital conversion, a 16-bit resolution device was used (NI USB-6211, National Instruments, Austin, TX). The sampling rate was 200 Hz. The bioimpedance measurement is using a 125 kHz frequency with 1 mA current. This amplifier previously passed FDA clearance and electrical safety tests. Data collection was performed via a laptop (G74S, ASUS, Taiwan, China) connected to a medical-grade isolation transformer (ISB 060 A, Toroid Co, Salisbury, MD). For visualization, recording, and processing of analog physiological signals, custom-built software was used (DataLyser, Walter Reed Army Institute of Research, Silver Spring, MD). Data files from each patient were saved automatically with their own, computer-generated identification. Data were processed offline.
2.1 Patient selection
We began the project by recording bioimpedance signals for any patient with reasonable suspicion of elevated ICP or change in intracranial compliance based on clinical status. From this point, we transitioned to monitoring patients that also had invasive ICP monitoring in place and with an external ventricular drain. Unfortunately, extracting the ICP waveform from the bedside monitor as an analog signal and recording simultaneously with REG pulse waves was not possible. We were, however, reliably able to extract the patient’s recorded Glasgow Coma Scale (GCS) from the electronic medical record. Two of the patients suffered from ischemic strokes and one patient suffered from hydrocephalus secondary to ventriculoperitoneal shunt malfunction. We present here (1) three patients, representing the status of improvement, worsening, and changing intracranial compliance during one recording; (2) REGx data of 8 patients who have repeated measurements.
2.2 Data analysis
-
(1)
REGx was calculated in DataLyser, in real-time as well as offline. REGx is the continuous Pearson’s correlation coefficient between thirty consecutive time-averaged (10 s) REG and peripheral pulse bioimpedance values. A positive index (positive correlation) implies impaired, passive CBF AR, while a negative index (inverse correlation) implies intact, active AR. REGx was calculated, identical to PRx calculation [10, 20] substituting the ICP and ABP waveforms with REG bioimpedance waveforms from the cranium and forearm, respectively. Mean REGx was calculated with GraphPad Prism (San Diego, CA). P values of less than 0.05 were considered significant; Table 1.
-
(2)
For REG pulse wave analysis, minimum-maximum time values of 5–10 REG pulse waves were measured and averaged in Excel (Microsoft, Redmond, WA). Also, it was considered pathological if the anacrotic portion was longer than 180 msec [32, 33].
-
(3)
REG pulse wave morphology was analyzed by inspecting the peaks of P1 and P2.
-
(4)
Status of systemic circulation was evaluated by shock index: (heart rate in beats per minute)/(systolic blood pressure in mmHg) [34]; and balance of the autonomic nervous system by modified Kerdo index: (1 − diastolic blood pressure/heart rate) + 100 [33, 35]. DataLyser was used to generate numerical values of REG pulse anacrotic time. The shock and Kerdo index were calculated from the patient’s record in a spreadsheet (Excel, Microsoft, Redmond, WA). For significance, a student t-test was used. Data analysis included collected data however, artifact-contaminated REG pulse waves were omitted; those waves cannot have the minimum-maximum distance measured on the pulse wave.
3 Results
3.1 Patient 1
A 26-year-old female with a history of IV drug use developed hydrocephalus and worsening ICC and cerebral edema, secondary to bilateral posterior cerebral artery circulation and bilateral anterior cerebral artery ischemic infarcts—Fig. 1.

Patient 1. Develo** hydrocephalus and worsening cerebral edema in patient 1 between recording day one 8/30 (left) and recording day two 8/31 (right)
Imaging demonstrates dilation of the third ventricle diameter measuring approximately 0.6 cm secondary to mass effect at the level of the cerebral aqueduct. The patient’s REGx mean was − 0.08 on the first day, and 0.44 on the second day, indicating worsening CBF AR. Coincidentally, ICC decreased, indicating increased P2 of REG pulse amplitude, Fig. 2.

Patient 1. The change of REG pulse waveform morphology of the patient with progressively worsening cerebral edema secondary to posterior circulation and bilateral anterior cerebral artery ischemic infarcts. NB: Respiratory subharmonics interfering with REG pulse wave morphology causing alternation of the highest peak. Upper panel—1st recording, REGx mean is − 0.08. Lower panel, 2nd day, REGx is 0.44. IC is compromised. ICP is elevated
ABP was 127/72 and the 1st day and 134/65 on the 2nd day. The Kerdo index was 100.48 on the 1st day of recording and 100.39 on the 2nd day. The shock index was 1.09 on the 1st day and 0.79 on the 2nd day. The heart rate was 138 bpm on the 1st day and 106 on the 2nd day.
3.2 Patient 2
A 49-year-old female with a history of subarachnoid hemorrhage status post ventriculoperitoneal shunt in 2009 presented with hydrocephalus secondary to ventriculoperitoneal shunt malfunction. Five successful recordings were performed throughout the patient’s stay and throughout the patient’s interventions. She underwent shunt externalization initially and finally underwent repair on the 3rd recording day. The radiographic progression of the patient’s hydrocephalus can be seen in Fig. 3.

Patient 2. Radiographic progression of a patient with ventriculoperitoneal shunt malfunction from the date of initial recording on 1/4 (left) to repair on the 5th day (middle) and follow-up on the 8th day (right)
Between recordings on the 1st and 5th recording days, the patient improved clinically from a GCS of 7 to 9 and then improved again between the 3rd and 4th recordings from a GCS of 9 to 14 which can be seen in Fig. 4. The patient underwent shunt revision on January 9 (marked J9 in Fig. 4). This led to a significant clinical improvement (GCS 7 improved to January 14 (J14) as well as a significant improvement in the appearance of the REG pulse waveform from a P2 > P1, poor ICC waveform, to P1 > P2, good compliance waveform (see Fig. 4).

Patient 2. REG pulse waveform morphology changes. 1st recording is on the top, last is on the bottom. One day—one recording. Time window: 5 s
Mean REGx values can be seen in Table 1. REGx mean was 0.32 on the 1st recording and 0.07 on the last. P-value: 0.0003, 95% confidence interval: − 0.38 to − 0.12. GCS was 7 and 14, respectively. The mean REGx value correlated clinically and radiographically with the patient’s status. ABP was 121/71 and the 1st day and 143/63 on the 5th day. The Kerdo index was 100.44 on the 1st day of recording and 100.43 on the 5th day. The shock index was 1.05 on the 1st day and 0.78 on the 5th day. The heart rate was 121 bpm on the 1st day and 111 on the 5th day.
3.3 Patient 3
An 88-year-old male with a past medical history of atrial fibrillation, hyperlipidemia, and left intracerebral hemorrhage 7 years prior to a presentation presented with right middle cerebral artery ischemic stroke treated by thrombectomy. Day 5 post thrombectomy, head CT revealed an interval increase in mass effect produced by persistent cerebral edema. The midline shift increased from 4.6 mm 4 days prior to 6.8 mm with compression of the right lateral ventricle and entrapment of the left lateral ventricle. The 36-minute REGx recording initially (left side) showed passive CBF AR—decreased CBF AR (REGx mean 0.61). During this time REG pulse morphology was: P2 > P1 Fig. 5.

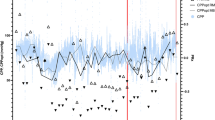
REGx and REG waveform morphology of a patient. In the beginning, the REGx mean was 0.61 ± 0.001 and at the end, it was − 0.49 ± 0.139; an average of 4 min (CBF AR is passive close to + 1 and active close to − 1). Accordingly, at the beginning REG pulse wave 2nd peak was higher, reflecting elevated ICP, while at the end peak 1 was higher, reflecting decreased ICP. REG electrodes were on the left frontotemporal area. REG anacrotic time 102.5 msec (mean of N = 10 pulse waves), reflecting non-sclerotic brain arteries. The time window of REGx is 36 min. Patient #3
In the second half of the REGx recording, CBF AR was active—and CBF AR was normal (REGx: − 0.49, PP2 (Fig. 5) ABP was 118/64 and the 1st day and 153/7 on the 2nd day. The Kerdo index was 100.3 on the 1st day of recording and 100.19 on the 2nd day. The shock index was 0.78 on the 1st day and 0.62 on the 2nd day. The heart rate was 92 bpm on the 1st day and 95 on the 2nd day.
3.4 Group results
There were 5 IS, 3 tumors, 1 ICH-T 2 ICH-NT, 1 SAH, and 1 HCP patient. The mean GCS was 9.79 ± 4.49. Mean systolic arterial pressure was 138.61, ± 23.77 mmHg, and diastolic was 68.57, ± 12.61 mmHg. The mean heart rate was 91.35, ± 27.01/min. The mean shock index was 0.69 ± 0.27; the mean Kerdo index was 117.99 ± 30.33. The mean REGx number was 0.49 ± 0.10. The mean REG anacrotic time in the normal group (5 patients, n = 15 measurements) was 110 ± 26 msec; in the arteriosclerotic group, it was 226 ± 20 msec (5 patients, n = 8 measurements). REG pulse wave was irregular in 17 recordings (74%). The linear correlation of REG anacrotic time to age was R2 = 0.3385. The mid-line shift was measured only 12 times. ICP was available 7 times. The mean REGx was 0.4 ± 0.21 (n = 28). REGx showed slow oscillations in both positive and negative areas but did not reach + 1/− 1, except in the case of an artifact. Artifacts caused sharp REGx changes that clearly correlated with patients’ movement or physical examination, causing artifacts in input signals. Event/note recording was helpful to identify the cause of these artifacts. REGx, recorded over several days (n = 8) is shown in Table 1. The difference between the first and third recordings was significant: p = 0.0177; 95% CI − 0.52 to − 0.05. Thisdifference supports the use of REGx monitoring.
3.5 REG pulse wave morphology
The distribution of REG pulse wave peak dominance was the following: (1) peak 1 was highest in 19 recordings; (2) peak 2 was highest in 11 recordings and (3) a triangle shape was present in one case. However, within recorded time, there was often an alteration of peak dominance, which correlated with the change of REGx numbers—Fig. 5. Irregularity (partial or full) was observed in all patients except one. In that case, however, the anacrotic time was pathological. This information supports the use of REG pulse morphology monitoring.
4 Discussion
We used REGx for real-time monitoring of CBF AR as well as observed REG pulse wave morphology as a function of changing intracranial compliance (referring to ICP). It is known that the brain damage resulting from traumatic as well as non-traumatic insults is not due solely to the direct consequences of the primary injury. A significant and potentially preventable contribution to the overall morbidity arises from secondary brain injury. Cerebral edema accompanied by elevated ICP prevents adequate cerebral perfusion. Detection of raised ICP could be useful in alerting clinicians to the need to improve cerebral perfusion, with consequent reductions in brain injury [36]. Hydrocephalus is also a commonly encountered and treatable cause of secondary brain injury. Patients 1 and 2 showed worsening CBF AR, as measured by increasing REGx values, and worsening ICC, as estimated by REG waveform changing to P2 > P1 waveform that correlated with the clinical picture. This patient’s REG pulse waveform improvement with clinical correlation as well as the previous patients’ REG pulse waveform worsening with clinical correlation indicates the use of REG as a noninvasive neuromonitoring method. Above mentioned changes support our hypothesis that REG can be used for neuromonitoring as was demonstrated in improving and worsening cases.
4.1 REGx
REGx values oscillate between ± 1, similar to PRx, monitoring in real-time. However, a notable trend in the mean REGx was detected for the future development of an alarm system. Our measurements demonstrated the clinical significance of the patient-specific change of mean REGx suggesting the importance of presenting mean REGx for the detection of changes in CBF AR. Like presenting blood pressure and relative changes in blood pressure rather than absolute changes in blood pressure or specific values. REGx is a realistic means of future non-invasive neuromonitoring. PRx > 0.3 is considered the warning threshold for impaired intracerebral compliance [10]. PRx > 0.3 is associated with an increase in ICP above 25 mmHg by minutes to hours and in some cases by 2 or 3 days [37]. Therefore, PRx > 0.3 is a threshold to detect worsening ICC. There is a need to create a standard for REGx in healthy patients since it does not exist for PRx. Probably no IRB would approve placing an ICP probe and needle into the radial artery in healthy subjects.
4.2 ICP and REG
Bedside monitors can show ICP pulse waves and their mean values. The size of the trace is about 25 mm. With such a resolution, probably the P1 and P2 positions are not real to expect to identify. However, “ICP is more than a number” [15]. ICP waveform alteration during elevated ICP was published [14, 15]. REG pulse wave alteration during elevated ICP (presumably due to worsening ICC) had a nearly identical shape as ICP waveform alteration during elevated ICP [12, 14, 15, 27, 37,38,39]. The presence of three or more inflection points was thought as characteristic of regressive changes in the arterial wall in patients with chronic subdural hematoma [40]. Similar results were described during the study in patients with normal-pressure hydrocephalus [27]. The authors evaluated this as a reduction in autoregulatory reserve. Similarly, ICP waveforms have 3 peaks [14, 15]. REG waves often have identical 3 or more peaks on the catacrotic portion. The described alteration of the REG waveform was identical to our observation, however, REGx did not show passive (close to + 1) status. REG changes were described previously during subdural hematoma and cerebrovascular alteration/arteriosclerosis [40]. An automatic detection algorithm was developed for ICP waveform analysis based on a similar observation as REG pulse wave distortion described here [41]. The relationship between non-invasive multi-frequency transcranial impedance measurements of the brain and skull and ICP in TBI patients in a previous study resulted in no correlation [42]. This type of measurement does not record the pulse wave. They recorded bioimpedance parameters of Zc (impedance at the characteristic frequency) and R0 (resistance to a direct current) which were then modeled against ICP using unadjusted and adjusted linear models. These bioimpedance variables did not seem to reflect CBF AR. It has been claimed that REG reflects head-skin blood flow and not intracranial blood flow. Waveform differences between extra and non-extracranial components of REG are significant and these differences could be used in a method to distinguish one from the other. However, a significant part of the REG signal is caused by a non-extracranial source and, therefore, it should not be used as a footprint of the extracranial blood flow [43]. However, during Trendelenburg’s position, an increase in extracranial blood volume will interfere (mask) with intracranial (vasoconstriction) change, so REG will reflect extracranial blood volume increase and not CBF AR [44].
4.3 Shock and Kerdo index
The shock index is the ratio of the heart rate to systolic blood pressure. The index is a sensitive indicator of left ventricular dysfunction and can become elevated following a reduction in left ventricular stroke work. It can be used in the Emergency Department and Intensive Care Unit to identify patients needing a higher level of care despite vital signs that may not appear strikingly abnormal. Normal values include 0.5 to 0.7. An elevated shock index (> 0.9) was found helpful by Rady et al. [34] to identify patients in the Emergency Department requiring admission and/or intensive care despite apparently stable vital signs. Persistent elevation of the shock index has been associated with poor outcomes in critically ill patients. The shock index of our patients was in the normal range. Kerdo index modified by Sipos [33] shows the balance of sympathetic and parasympathetic dominance: <100 is sympathicotonia. The Kerdo index of our patients indicated moderate sympathicotonia. The Kerdo index indicated circulatory stress in an animal study [45].
5 Conclusion
The novelty and value of this descriptive study are, that we presented that REG can be used (1) to measure the status of CBF AR in real-time (REGx); (2) REGx decrease indicated the improved status of a patient; (3) REGx change coincided with REG pulse wave morphology change and improvement of brain imaging; (4) REG pulse wave morphology alteration was identical to the published ICP pulse wave morphology change during worsening of the ICC (increased P2). These results are a continuation of previous observations which suggested that REG can be used to reflect CBF AR and ICP change [26, 29]. We demonstrated the possibility to switch from invasive (ICP, ABP—PRx) to noninvasive (bioimpedance—REGx) neuromonitoring. REG/REGx potentially offers a predictive value for worsening CBF AR and ICC in the setting of acute brain injury. This may offer a cheaper, non-invasive, continuous, and convenient alternative monitoring tool to prevent secondary brain injury. Particularly in settings where invasive monitoring is not possible, including the battlefield and the pre-hospital settings. REG monitoring fits into the USU Surgical Critical Care Initiative (SC2i), which focuses on develo** Clinical Decision Support Tools for critical care [46]. Naturally, such an approach can be used in a civilian environment as well. Future correlation studies between ICP and REG and PRx and REGx can justify the use of REG in neurocritical care. Additionally, a bioimpedance module can be added to the bedside monitors, which can calculate REGx. We plan to create a program capable to generate a trigger if (1) PRx/REGx is > 0.3; (2) if REG P2 is > P1; (3) to create a healthy standard for REGx since it is not available for PRx.
Data availability
Available upon reasonable request.
References
Bellamy R, Safar P, Tisherman SA et al. (1996) Suspended animation for delayed resuscitation. Crit Care Med 24: 24-47.
Knuth T, Letarte PB, Ling G, Moores LE, Rhee P, Tauber D, Trask A. Guidelines for Field Management of Combat-Related Head Trauma. 2005. https://www.braintrauma.org/uploads/02/09/btf_field_management_guidelines_2.pdf. Accessed 30 Dec 2021
BOOST-2. Brain Tissue Oxygen Monitoring in Traumatic Brain Injury (TBI)—Full-Text View—ClinicalTrials.gov. 2022. https://clinicaltrials.gov/ct2/show/NCT00974259?cond=Brain+Tissue+Oxygen+Monitoring+in+Traumatic+Brain+Injury+%28TBI%29&draw=2&rank=1. Accessed 22 Sep 2022
Hutchinson P. Current status of multimodality monitoring in TBI. Codman Neuro Critical Care Monitoring webinars, 20th November 2020. https://icmplus.neurosurg.cam.ac.uk/codman-monitoring-webinars_2020/. Acessed 30 Dec 2021
Leach MR, Shutter LA. How much oxygen for the injured brain - can invasive parenchymal catheters help? Curr Opin Crit Care. 2021;27(2):95–102. https://doi.org/10.1097/MCC.0000000000000810.
Steiner LA, Andrews PJ. Monitoring the injured brain: ICP and CBF. Br J Anaesth. 2006;97:26–38. https://doi.org/10.1093/bja/ael110.
Czosnyika M, Hutchinson P, Kirkpatrick PJ, Pickard JD. (2009) Monitoring of the brain: pressures flow, and brain tissue probes. In: Jallo J and Loftus CM (eds) Neurotrauma and Critical Care of the Brain. Thieme, New York, pp 66–105
Mendelson A, Gillis C, Henderson WR, Ronco J, Dhingra V, Griesdale DE. Intracranial pressure monitors in traumatic brain injury: a systematic review. Can J Neurol Sci. 2012;39:571–6. https://doi.org/10.1017/s0317167100015286.
Rubin M, Yo M, Agostini MA, Madden J, Diaz-Arrastia RR. Noninvasive monitoring. In: Jallo J, Loftus CM, editors. Neurotrauma and critical care of the brain. New York: Thieme; 2009. pp. 53–65.
Anonymous. ICM + program: Software for Brain Monitoring in Neurological Intensive Care. 2021. http://www.neurosurg.cam.ac.uk/pages/ICM/about.php Accessed 30 Dec 2021
Hawthorne C, Piper I. Monitoring of intracranial pressure in patients with traumatic brain injury. Front Neurol. 2014;5(121):1–16. https://doi.org/10.3389/fneur.2014.00121.
Kawoos U, McCarron RM, Auker CR, Chavko M. Advances in intracranial pressure monitoring and its significance in managing traumatic Brain Injury. Int J Mol Sci. 2015;16:28979–97. https://doi.org/10.3390/ijms161226146.
Harary M, Dolmans RGF, Gormley WB. Intracranial pressure monitoring - review and avenues for development. Sens (Basel). 2018;18(465):1–15. https://doi.org/10.3390/s18020465.
Ellis T, McNames J, Aboy M. Pulse morphology visualization and analysis with applications in cardiovascular pressure signals. IEEE Trans Biomed Eng. 2007;54:1552–9. https://doi.org/10.1109/TBME.2007.892918.
Czosnyka M, Czosnyka Z. Origin of intracranial pressure pulse waveform. Acta Neurochir (Wien). 2020;162:1815–7. https://doi.org/10.1007/s00701-020-04424-4.
Strandgaard S, Paulson OB. Cerebral autoregulation. Stroke. 1984;15:413–6. PMID: 2201348.
Chillon JM, Baumbach GL. Autoregulation: arterial and intracranial pressure. In: Edvinsson L, Krause DN, editors. Cerebral blood flow and metabolism – 2. Philadelphia: Lippincott Williams & Wilkins; 2002. pp. 395–412.
Guyton AC. Textbook of medical physiology. 8th ed. Philadelphia: Saunders; 1991.
Kontos HA, Wei EP, Navari RM, Levasseur JE, Rosenblum WI, Patterson JL Jr. Responses of cerebral arteries and arterioles to acute hypotension and hypertension. Am J Physiol. 1978;234:H371–83. https://doi.org/10.1152/ajpheart.1978.234.4.H371.
Donnelly J, Aries MJ, Czosnyka M. Further understanding of cerebral autoregulation at the bedside: possible implications for future therapy. Expert Rev Neurother. 2015;15:169–85. https://doi.org/10.1586/14737175.2015.996552.
Manley G, Knudson MM, Morabito D, Damron S, Erickson V, Pitts L. Hypotension, hypoxia, and head injury: frequency, duration, and consequence. Arch Surg. 2001;136:1118–23. https://doi.org/10.1001/archsurg.136.10.1118.
Anonymous. Rheoencephalograph (a) Identification Code of Federal Regulations Title 21, vol 8, Sect. 882.1825, Washington, DC: US Government Printing Office; Revised as of April 1, 1997. https://www.law.cornell.edu/cfr/text/21/882.1825. Accessed: Sept 21, 2022
Grimnes S, Martinsen O. (2008) Bioimpedance and Bioelectricity Basics, 2nd Edition. Academic Press, Amsterdam
Bodo M, Montgomery LD, Pearce FJ, Armonda R. Measurement of cerebral blood flow autoregulation with rheoencephalography: a comparative pig study. J Electr Bioimp. 2018;9:123–32. https://doi.org/10.2478/joeb-2018-0017.
McHenry LC. Rheoencephalography: a clinical appraisal. Neurology. 1965;15:507–17. https://doi.org/10.1212/wnl.15.6.507.
Bodo M, Racz J, Ilias L, et al. Rheoencephalographic changes during increased intracranial pressure. In: Krieglstein J, editor. Pharmacology of cerebral ischemia. Amsterdam: Elsevier; 1986. pp. 265–9. https://www.researchgate.net/publication/279850836_Rheoencephalographic_changes_during_increased_intracranial_pressure.
Traczewski W, Moskala M, Kruk D, Gościński I, Szwabowska D, Polak J, Wielgosz K. The role of computerized rheoencephalography in the assessment of normal pressure hydrocephalus. J Neurotrauma. 2005;22:836–43. https://doi.org/10.1089/neu.2005.22.836.
Brady KM, Mytar JO, Kibler KK, et al. Monitoring cerebrovascular pressure reactivity with rheoencephalography. J Phys Conf Ser. 2010;201:224012089. https://doi.org/10.1088/1742-6596/224/1/012089.
Bodo M, Simovic M, Pearce F, Ahmed A, Armonda R. Correlation of rheoencephalogram and intracranial pressure: results of a rat study. Physiol Meas. 2015;36:N115–26. https://doi.org/10.1088/0967-3334/36/10/N115.
Bodo M, Garcia A, Pearce F, van Albert S, Armonda R. Influence of volume and change on the electrical impedance signal (in vitro). J Phys Conf Ser. 2010;22:012111. https://doi.org/10.1088/1742-6596/224/1/012111.
Moskalenko YE. Biophysical Aspects of cerebral circulation. Oxford: Pergamon; 1980.
Jenkner FL. Clinical rheoencephalography: a non-invasive method for automatic evaluation of cerebral hemodynamics. Vienna: Ertldruck; 1986.
Bodo M, Thuroczy G, Nagy I, et al. A complex cerebrovascular screening system (CERBERUS). Med Prog Technol. 1995;21:53–66. PMID: 7565396.
Rady MY, Smithline HA, Blake H, Nowak R, Rivers E. A comparison of the shock index and conventional vital signs to identify acute, critical illness in the emergency department. Ann Emerg Med. 1994;24:685–90. https://doi.org/10.1016/s0196-0644(94)70279-9.
Kerdo I. An index for the evaluation of vegetative tonus calculated from the data of blood circulation. Acta Neuroveg (Wien). 1966;29:250–68. https://doi.org/10.1007/BF01269900.
Forsyth RJ, Raper J, Todhunter E. Routine intracranial pressure monitoring in acute coma. Cochrane Database Syst Rev. 2015;11:CD002043. https://doi.org/10.1002/14651858.CD002043.pub3.
Czosnyka M, Aries M, Weersink C, et al. “Solid Red Line”: an observational study on death from refractory intracranial hypertension. Acta Neurochir Suppl. 2016;122:113–6. https://doi.org/10.1007/978-3-319-22533-3_22.
Kim MO, Adji A, Orourke MF et al. (2016) Change in pulsatile cerebral arterial pressure and flow waves as a therapeutic strategy? Acta Neurochir Suppl 122:167 – 70. DOI: https://doi.org/10.1007/978-3-319-22533-3_34
Czosnyka M, Pickard JD, Steiner LA. Principles of intracranial pressure monitoring and treatment. Handb Clin Neurol. 2017;140:67–89. https://doi.org/10.1016/B978-0-444-63600-3.00005-2.
Krupa M, Traczewski W, Moskała M, Szwabowska D, Gościński I. Prognostic value of computerized rheoencephalography in chronic posttraumatic subdural hematoma: a preliminary report. Neurol Neurochir Pol. 2005;39:213–9. PMID: 15981159.
Aboy M, McNames J, Goldstein B. Automatic detection algorithm of intracranial pressure waveform components. Conference Proceedings of the 23rd Annual International Conference of the IEEE Engineering in Medicine and Biology Society, pp. 2231–2234 vol. 3. 2001. https://ieeexplore.ieee.org/document/1017216 Accessed 12 30, 2021.
Hawthorne C, Shaw M, Piper I, Moss L, Kinsella J. Transcranial bioimpedance measurement as a non-invasive estimate of intracranial pressure. Acta Neurochir Suppl. 2018;126:89–92. https://doi.org/10.1007/978-3-319-65798-1_19.
Perez JJ. To what extent is the bipolar rheoencephalographic signal contaminated by scalp blood flow? A clinical study to quantify its extra and non-extracranial components. Biomed Eng Online. 2014;13:131. https://doi.org/10.1186/1475-925X-13-131.
Bodo M, Mahon R, Razumovsky A, et al. Comparison of cerebrovascular reactivity tests: a pilot human study. J Electr Bioimp. 2017;8:25–33. https://sciendo.com/article/10.5617/jeb.3939.
Montgomery LD, Montgomery RW, Bodo M, Mahon RT, Pearce FJ. Thoracic, peripheral, and cerebral volume, circulatory and pressure responses to PEEP during simulated hemorrhage in a pig model: a case study. J Electr Bioimp. 2021;12:103–16. https://doi.org/10.2478/joeb-2021-0013.
USU. Department of Surgery: Surgical critical care initiative: The future of precision medicine. 2021. https://medschool.usuhs.edu/sur/research/sc2i Accessed 12, 2021.
Acknowledgements
The authors thank the measured patients for their participation; Lajos Baranyi, Matt Dennie, and Fred Pearce for the development of DataLyser and REGx calculation.
Funding
The authors did not receive support from any organization for the submitted work.
Author information
Authors and Affiliations
Contributions
LAC: conception and design of the work; clinical data analysis, interpretation of data. II: conception and design of the work, revising the manuscript. VR: acquisition of data, acquisition of clinical data, revising the manuscript. MB: acquisition of data (bio-impedance signals), analysis, drafting the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose.
Ethical approval
The protocol was approved by the local IRB.
Consent to participate
All patients or family members gave written informed consent prior to study participation.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Cannizzaro, L.A., Iwuchukwu, I., Rahaman, V. et al. Noninvasive neuromonitoring with rheoencephalography: a case report. J Clin Monit Comput 37, 1413–1422 (2023). https://doi.org/10.1007/s10877-023-00985-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10877-023-00985-8