
Abstract
Background
Surgical decompression to the optic-chiasmatic region in craneofacial fibrous dysplasia (CFD) must be performed safely to improve or stabilize visual loss.
Method
We describe a technical nuance when facing on a huge, deformed skull with potentially imbricated dura mater. Craniectomy was performed in concentric arches allowing to expose surgical field and elevated step by step. Bilateral micro-decompression was performed after without difficulties.
Conclusions
Decompressing both optic nerves using this technique is safe and relatively simple to perform.






Similar content being viewed by others


Abbreviations
- FD:
-
Fibrous dysplasia
- CFD:
-
Craneofacial fibrous dysplasia
- ON:
-
Optic nerve
- LE:
-
Left eye
- RE:
-
Right eye
- VA:
-
Visual acuity
- MRI:
-
Magnetic resonance imaging
- CT:
-
Computer tomography
References
Abe T, Sato K, Otsuka T, Kawamura N, Shimazu M, Izumiyama H, Matsumoto K (2002) Optic nerve decompression for orbitofrontal fibrous dysplasia. Skull Base 12(3): 145–152. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1656939/
Abe T, Sato K, Wada A (2006) Optic nerve decompression for orbitofrontal fibrous dysplasia. Recent development of surgical technique and equipment. Skull Base 16(3):145–155. https://doi.org/10.1055/s-2006-949517
Amit M, Collins MT, FitzGibbon EJ, Butman JA, Fliss DM, Gil Z (2011) Surgery versus watchful waiting in patients with craniofacial fibrous dysplasia. A meta-analysis. PLoS One 6(9):e25179. https://doi.org/10.1371/journal.pone.0025179
Arroyo J G, Lessell S, Montgomery W W (1991) Steroid-induced visual recovery in fibrous dysplasia. J Clin Neuroophthalmol 11(4):259–61. https://pubmed.ncbi.nlm.nih.gov/1838545/
Béquignon E, Cardinne C, Lachiver X, Wagner I, Chabolle F, Baujat B (2013) Craniofacial fibrous dysplasia surgery: a functional approach. Eur Ann Otorhinolaryngol Head Neck Dis 130(4):215–220. https://doi.org/10.1016/j.anorl.2012.07.005
Dumont AS, Boulos PT, Jane JA Jr, Ellegala DB, Newman SA, Jane JA Sr (2001) Cranioorbital fibrous dysplasia: with emphasis on visual impairment and current surgical management. Neurosurg Focus 10(5):E6. https://doi.org/10.3171/foc.2001.10.5.7
Michael CB, Lee AG, Patrinely JR, Stal S, Blacklock JB (2000) Visual loss associated with fibrous dysplasia of the anterior skull base. Case report and review of the literature. J Neurosurg 92(2):350–4. https://doi.org/10.3171/jns.2000.92.2.0350
Reem EMG, Rongsheng C (2018) Emergency optic canal decompression for vision salvage in fibrous dysplasia. World Neurosurg 109:134–137. https://doi.org/10.1016/j.wneu.2017.09.119
Yew Leong LT, Chang Chong Ming BJ (2015) Craniofacial fibrous dysplasia involving the orbit: a case report and literature review. Asia Pac J Ophthalmol (Phila) 4(3):151–154. https://doi.org/10.1097/APO.0000000000000043
Ying-Chien T, Chung-Chih Y, Chen-Nen C, Lih M, Yu-Ray C (2007) Optic nerve compression in craniofacial fibrous dysplasia: the role and indications for decompression. Plast Reconstr Surg 120(7):1957–1962. https://doi.org/10.1097/01.prs.0000287338.28018.c7
Acknowledgements
We are grateful to Dr. Ariel Kaen for hel** us with the video production, to Drs. Jorge Herrería and Cristina Romero for reviewing and editing, and to all authors for providing information, picture editing and text reviewing.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Key points
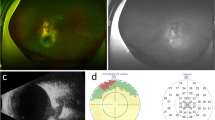
1. Preoperative study by MRI. Evaluate compromised structures, show the affectation of the superior orbital fissure, and look for atrophy of the ONs.
2. Do not operate patients with CFD without visual symptoms. Decompressing the optic canal has severe risks and is not indicated prophylactically.
3. Craniectomy in concentric arches. Removing the deformed bone in parts helps the surgeon to preserve the dura and easily pass the drills with direct control. (Figs. 3, 4).
4. Be aggressive. Wide resections are related to good cosmetic and definitive results, with lower rates of recurrence.
5. Bleeding. Fibrotic bone bleeds more than normal do. It could be controlled with no special maneuver. Avoid using electrocautery and reserve blood beforehand.
6. Extensive irrigation. This is the key to prevent damage of ONs. Do it through the micro-decompression [1,2] (Video 1).
7. Reshape the skull. In extensive CFDs, intervention only to decompress the ON is not indicated. Treat the aesthetic problem.
8. Add corticosteroids. Short therapies have been related to improvement in the VA before and after surgery and even with nerve atrophy.
9. Stop visual impairment. In cases where the VA does not improve, stop** the progression is also a therapeutic objective.
10. Evaluate the benefit of surgery. It is not always indicated.
This article is part of the Topical Collection on Neurosurgical technique evaluation
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 (MP4 138572 KB)
Rights and permissions
About this article

Cite this article
Butrón-Díaz, C., Rivero-Garvia, M. & Márquez-Rivas, J. Bilateral chiasm and optic nerve micro-decompression in a child with extensive cranial fibrous dysplasia: how I do it. Acta Neurochir 164, 1485–1491 (2022). https://doi.org/10.1007/s00701-021-05036-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-021-05036-2