
Summary
Background
Kidney transplant recipients (KTR) are a group of patients with heterogeneous risks for adverse outcomes with COVID-19, but risk stratification tools in this patient group are lacking.
Methods and participants
This retrospective observational, hypothesis-generating study included 49 hospitalized adult KTR patients with COVID-19 at the University Hospital of Split (August 2020 to October 2021) and evaluated the performance of novel risk score CROW-65 (age, Charlson Comorbidity Index [CCI] lactate dehydrogenase to white blood cell [LDH:WBC] ratio, and respiratory rate oxygenation [ROX index]). The primary outcome of the study was 30-day postdischarge all-cause mortality.
Results
A total of 8 fatal events (16.3%) occurred during the study follow-up. When comparing CROW-65 by survival status, it was significantly increased in patients with fatal event (P < 0.001). Using the Cox proportional hazards regression analysis, the CROW-65 risk score showed statistically significant association with mortality (HR 1.11, 95% CI 1.01–1.23, P = 0.027), while receiving operator characteristics (ROC) showed significant discrimination of all-cause mortality with an AUC of 0.85 (95% CI 0.72–0.94, P < 0.001), and satisfactory calibration (χ2 4.91, P = 0.555 and Harrell’s C 0.835). Finally, survival Kaplan-Meier analysis confirmed significantly higher cumulative incidence of mortality with increasing risk score tertiles and curve separation after 13 days (P = 0.009).
Conclusion
A novel risk score CROW-65 showed significant association with all-cause mortality in KTR yielding important hypothesis-generating findings. Further powered studies should reassess the performance of CROW-65 risk score in this population, including predictability, calibration and discrimination.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Novel SARS-CoV‑2 disease (COVID-19) is a tremendous global health burden leading to substantial morbidity and mortality, especially among patients with established chronic diseases [1, 2]. Chronic kidney disease (CKD) is one of the important risk factors for adverse outcomes associated with COVID-19, but its heterogeneity and specific settings still impede from drawing strong conclusions [2,3,4].
In the light of the COVID-19 pandemic, numerous studies have investigated the interaction of COVID-19 and CKD and its subpopulations such as kidney transplant recipients (KTR) [3, 5,6,7,8,9,10,11,12]. The latter population is particularly of interest due to frailty and predisposition to worse outcomes, and previous studies have suggested high mortality rates associated with COVID-19 ranging from 18.6% to 44.3% [6, 11]. Adverse outcomes in KTR could be attributed to a few pathophysiological mechanisms. Firstly, due to the chronic immunosuppressive therapy and ensuing suppression of cellular immunity, this population is at higher risk of viral infections [5]. Secondly, chronic immunosuppressive therapy has various immunomodulatory effects and could impair with the immunologic response during COVID-19 [5, 13,14,15]. Furthermore, frailty and susceptibility for recurrent kidney impairments during any infection portends these patients to adverse events. Increased cardiovascular risk, anemia, fluid imbalance, electrolyte disorders, and other companions of CKD could additionally impact the prognosis of these patients [14].
Therefore, identification of KTR patients with COVID-19 who are particularly prone to worse outcomes in this at risk population could improve the focus and quality of care. Previous studies have mainly evaluated the management and outcomes of these patients, but risk scores for objective assessment and stratification of this heterogenic population are rare. Only one recently developed web-based risk calculator has been studied for prediction of COVID-19-associated mortality in KTR [16]. Similarly, our author group newly developed a novel risk score CROW-65 (age, Charlson comorbidity index [CCI], lactate dehydrogenase to white blood cell [LDH:WBC ratio], and respiratory rate oxygenation [ROX index]) with the respectable prediction of in-hospital mortality among hospitalized COVID-19 patients treated with high-flow nasal oxygen (HFNO) [17]; however, further validation of this risk score in different patient populations with COVID-19 is warranted.
This study, therefore, aimed to examine the association of the novel risk score CROW-65 with all-cause mortality of these patients within 30 days of discharge. In addition, the aim was to provide exploratory findings about baseline differences between risk score tertiles, including the association of individual components of the aforementioned risk score with mortality.
Methods
Rationale for the study
Despite the growing pandemic, risk scoring system for assessment of KTR patients with COVID-19 are generally lacking [16]. With that incentive, authors aimed to evaluate a novel, recently constructed CROW-65 risk score in this patient population. This risk score was primarily computed on the non-transplant patients with COVID-19 treated with HFNO; however, having in mind the importance of individual components of the CROW-65 risk score in this population (age, comorbidities, i.e. CCI and ROX index), it is hypothesized that it could have accuracy in this population as well. Due to a limited sample size, retrospective design, small number of events and selected KTR population, this study has hypothesis-generating purpose.
Ethical and institutional considerations
All the proceedings and clinical research were performed according to the ethical standards and amendments of the Declaration of Helsinki. The study protocol was approved by the Ethics Committee of the University Hospital of Split, Croatia (No. 2181-147-01/06). All the collected data were stored and kept confidential.
Study design and patients
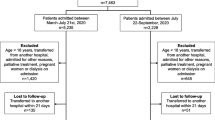
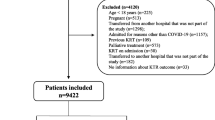
This single-center observational retrospective study included 49 eligible adult KTR who developed COVID-19 and were treated at the University Hospital of Split from August 2020 to October 2021. Analysis included in-hospital and 30-day postdischarge period. Active COVID-19 was diagnosed and confirmed in all patients with the specific 3‑sequence (E-gen; ORF 1ab-gen; N‑gen) reverse transcription-polymerase chain reaction (RT-PCR) test (Liferiver Novel Coronavirus [Shanghai ZJ Bio-Tech Co, Shanghai, China] RT-PCR Kit/MIC qPCR cycler). Patients of both sexes were included in the study. Exclusion criteria were incomplete medical documentation and active malignant disease. The initial patient screening included a total of 51 patients, but study eligibility was confirmed in 49 patients who were finally included in the analysis (per protocol population). The flow diagram of the study is shown in Supplementary Fig. 1. Due to routine ambulatory follow-up within the kidney transplant database, there was no loss to follow-up. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist for observational studies is reported in Appendix A.
Data sources
Relevant medical data were obtained from the hospital’s electronic medical records, therapeutic lists, and paper documentation.
Clinical, laboratory and radiologic assessment
All enrolled patients underwent detailed clinical, laboratory and radiologic assessment. Baseline clinical characteristics included age, sex, vital parameters, comorbidities, transplant-related data (transplant duration, chronic medication therapy), COVID-19-related data (symptoms, symptom duration, medical findings, active hospital treatment, chronic medication dose modification), and vaccination status. The following laboratory parameters were collected (admission values, if not specified otherwise): WBC, red blood cells (RBC), hemoglobin, platelets, C‑reactive protein (CRP), blood urea nitrogen (BUN), creatinine, D‑dimers, and LDH. The estimated glomerular filtration rate (eGFR) was calculated using a CKD-EPI formula [18]. The comorbidity burden was determined using CCI [19]. The ROX index was calculated using the ratio of oxygen saturation/fraction of inspired oxygen (derived from oxygen flow rate and application method), and respiratory rate.
CROW-65 risk score
The recently developed risk score CROW-65 represents a promising simple tool for the stratification of patients with COVID-19 [17]. It has been primarily constructed using data on hospitalized COVID-19 patients who were treated with HFNO. It showed satisfactory discrimination of in-hospital mortality (AUC 0.925, 95% CI 0.870–0.981). Using the predefined weighting, CROW-65 is calculated from age, CCI, LDH:WBC ratio, and ROX index. A total score ranges between a minimum value of 3 and maximum value of 41. In the original study, higher score values were associated with worse outcomes [17].
Outcomes
A primary outcome was the association of the CROW-65 risk score and 30-day postdischarge all-cause mortality. Secondary exploratory analyses included the comparison of baseline characteristics across risk score tertiles, and association of each individual component of the CROW-65 risk score and 30-day postdischarge all-cause mortality.
Statistical analysis
Continuous data were presented as median (IQR) and analyzed using the Kruskal Wallis test, while categorical variables were expressed as numbers (percentages) and analyzed using the χ2-test. Patients were stratified based on CROW-65 risk score tertiles (≤ 6.33, 6.33–8.67, ≥ 8.67) only to evaluate exploratory differences in baseline characteristics between tertile groups. All the remaining analyses were conducted using CROW-65 as a continuous variable in order to improve accuracy of the models.
Univariate Cox proportional hazard regression analysis was conducted to assess the association of selected variables with all-cause mortality and described as hazard ratio (HR) and 95% confidence intervals (95% CI). The following variables were investigated: CROW-65, age, CCI, LDH:WBC ratio and ROX index. Furthermore, the performance of CROW-65 and each component of the score in discriminating all-cause mortality was tested using receiver operating characteristic (ROC), with a calculation of area under the curve (AUC). Calibration/goodness-of-fit was assessed by the Hosmer-Lemeshow goodness-of-fit test, Harrell’s C concordance index and visually by calibration plots [20, 21]. Between-AUC comparison was tested using an algorithm based on the methodology of Hanley and McNeil [22]. Additionally, survival analysis was estimated using the Kaplan-Meier approach, and significance was assessed using the Mantel-Cox log-rank test.
The aforementioned statistical methods were used to 1) account for standard approach for survival data analysis (hazard ratios and Kaplan-Meier approach); 2) detect prognostic performance of risk score. A two-sided P-value of < 0.05 was considered significant. P-values were not adjusted for multiple tests and should be interpreted as exploratory only. Statistical data analysis was carried out using a Statistical Package for the Social Sciences (SPSS) software (IBM Corp, Armonk, NY, USA; version 20) and Stata software (StataCorp, College Station, TX, USA; version 17).
Results
Prior to the analysis, 2 patients were excluded due to incomplete medical documentation (both patients survived to discharge). A total of 49 adult patients of both sexes were finally included in the analysis. In the exploratory analysis, there was no statistically significant difference in baseline characteristics between the study groups according to CROW-65 risk score tertiles (P > 0.05), except for age (1st tertile: 56.5 IQR 50.5–64.0 years vs. 2nd tertile: 62.0 IQR 50.5–71.5 years vs. 3rd tertile: 67.0 IQR 61.0–72.8 years, P = 0.013) and transplant duration (1st tertile: 4.5 IQR 2.0–8.8 vs. 2nd tertile: 6.0 IQR 2.5–10.5 vs. 3rd tertile: 10.0 IQR 6.0–17.0 years, P = 0.023) (Table 1). When comparing laboratory results between study groups, there was a statistically significant difference only in RBC (1st tertile: 4.9 IQR 4.6–5.4 vs. 2nd tertile: 4.4 IQR 4.1–4.7 vs. 3rd tertile: 4.5 IQR 3.9–5.0 × 1012/L, P = 0.039), hemoglobin (1st tertile: 138.0 IQR 129.6–160.0 vs. 2nd tertile: 127.0 IQR 119.0–139.0 vs. 3rd tertile: 130.5 IQR 109.8–149.8 g/L, P = 0.077), and D‑dimers (1st tertile: 0.6 IQR 0.4–0.8 vs. 2nd tertile: 0.8 IQR 0.5–1.1 vs. 3rd tertile: 0.9 IQR 0.8–1.6 mmol/L, P = 0.011) (Table 1). When comparing chronic immunosuppression therapy between the study groups, there was no difference in the baseline therapy nor in the therapy modification during the index hospitalization (P > 0.05) (Table 1 and 2). There was no difference in vaccination status between the study groups (P > 0.05) (Table 1). Importantly, there was no significant difference in the need for oxygen supplementation, utilization of remdesivir, and corticosteroid therapy (P > 0.05) (Table 2). The only statistically significant difference between the groups in terms of the clinical picture was the higher presence of X‑ray-confirmed pneumonia in 2nd and 3rd CROW-65 tertiles (13, 76.5% and 13, 81.3%, respectively), compared to 1st tertile (7, 43.8%, P = 0.047) (Supplementary Table 1).
A total of 8 fatal events (16.3%) occurred during the study follow-up. When comparing CROW-65 by survival status, it was significantly increased in patients with fatal event (P < 0.001) (Fig. 1). Using the univariate Cox proportional hazard regression analysis, the CROW-65 risk score proved to be a statistically significantly associated with all-cause mortality (HR 1.11 95% CI 1.01–1.23, P = 0.027) (Table 3).

Distribution of CROW-65 by survival status. CROW-65 risk score composed of age, ROX index, LDH:WBC ratio, and CCI score. CCI Charlson Comorbidity Index, LDH lactate dehydrogenase, ROC receiver operating characteristics, ROX the ratio of oxygen saturation and a fraction of inspired oxygen, WBC white blood cells
In addition, the risk score model CROW-65 showed significant discrimination of all-cause mortality, with an AUC of 0.85 (95% CI 0.72–0.94, P < 0.001) (Table 4 and Fig. 2b). When evaluating individual risk score components, all of them showed statistically significant discrimination of all-cause mortality, except LDH:WBC ratio (P = 0.281) (Table 4 and Fig. 2a). Comparison of different ROC curves revealed that there was no statistically significant difference in ROC curves between CROW-65 and individual risk score components (age, CCI, and ROX), except between CROW-65 and LDH:WBC ratio (difference between areas 0.22, P = 0.042) (Supplementary Table 2). The Hosmer-Lemeshow test and Harrell’s C concordance index proved adequate calibration of the models, specifically CROW-65 (χ2 4.91, P = 0.555 and C 0.835), CCI (χ2 0.93, P = 0.920 and C 0.804), LDH-to-WBC ratio (χ2 6.91, P = 0.546 and C 0.637), ROX (χ2 2.75, P = 0.840 and C 0.879), and age (χ2 9.18, P = 0.328 and C 0.762). Model calibration was additionally assessed visually as depicted in Supplementary Fig. 2.

Receiver operating characteristics of the: a Individual components of the CROW-65 risk score; b CROW-65 risk score. CROW-65 risk score composed of age, ROX index, LDH-to-WBC ratio, and CCI score. CCI Charlson Comorbidity Index, LDH lactate dehydrogenase, ROC receiver operating characteristics, ROX the ratio of oxygen saturation and a fraction of inspired oxygen, WBC white blood cells
Finally, when looking at the survival Kaplan-Meier analysis, the cumulative incidence of all-cause mortality was significantly different between risk score tertiles, with separation of curves after 13 days, and the 3rd CROW-65 tertile having the highest all-cause mortality (P = 0.009) (Fig. 3).

Survival analysis (Kaplan Meier) in different patient groups based on CROW-65 risk score tertiles. CROW-65 risk score composed of age, ROX index, LDH:WBC ratio, and CCI score
Discussion
This is the first study to evaluate the performance of a novel risk score CROW-65 in the KTR population with COVID-19. Having in mind the lack of risk stratification tools in this fragile patient population, this study could add novel evidence to the existing literature regarding these patients. There are several important findings of this study. Firstly, KTR patient population has substantial mortality associated with COVID-19. Secondly, CROW-65 showed significant association with all-cause mortality in this population. Finally, due to a limited sample size, retrospective design, and selected KTR population, these findings have only hypothesis-generating purpose.
The global health burden associated with COVID-19 forced the scientific community to develop different risk prognostic scores; however, most of them are validated in the general population, and their application in specific patient groups such as KTR is questionable. One of them, the VACO index, predicts 30-day mortality based on demographic characteristics and comorbidities, without taking into account clinical presentation and laboratory parameters [23]. Furthermore, Knight et al. developed the 4C Mortality Score which, in addition to demographic data and comorbidities, includes clinical and laboratory parameters for prediction of in-hospital mortality [24]. Another interesting risk score was recently developed and showed an excellent discrimination of all-cause mortality in KTR with COVID-19 [16]. As previously mentioned, the CROW-65 risk score was also recently developed for the prediction of in-hospital mortality in COVID-19 patients treated with HFNO [17]. As opposed to the abovementioned risk scores, CROW-65 includes both clinical factors (ROX index) and laboratory factors (LDH:WBC ratio) in addition to patient characteristics and comorbidity burden; however, clinical application of this score in specific settings such as the KTR population warrants validation and further research.
To the best of our knowledge, only one study validated prognostic risk score in KTR patients with COVID-19 [16]. It has been previously suggested that some patient characteristics are particularly associated with adverse outcomes in COVID-19. Specifically, older age was associated with higher COVID-19 associated mortality in a recent meta-analysis comparing the KTR survivors and non-survivors (weighted mean difference 10.5, IQR 9.3–11.8, P < 0.001) [25]. The association of older age and worse outcomes in KTR patients is consistent with this and other studies [2, 7, 12]. Comorbidity burden was shown to be equally important in this at risk population, particularly the presence of diabetes mellitus, cardiovascular diseases, and active cancer (pooled odds ratios of mortality: 1.80 (1.43, 2.26), P < 0.001; 2.21 (1.60, 3.06), P < 0.001; and 2.00 (1.05, 3.80), P = 0.034; respectively) [25]. The clinical presentation also had a significant prognostic impact with pneumonia (OR 10.64, 95% CI 3.37–33.56, P < 0.001), dyspnea (OR 5.68, 95% CI 2.11–15.33, P < 0.001), and acute kidney injury (OR 3.24, 95% CI 1.36–7.70, P = 0.008) carrying the worst effects [25]. In addition, ROX index as a well-established prognostic risk factor for invasive ventilation previously showed a significant prediction of overall mortality in immunocompromised patients [26]. Differing findings were previously reported for LDH:WBC ratio in COVID-19 settings. A meta-analysis examining mortality risk factors in the KTR population with COVID-19 showed that LDH and WBC do not exhibit significant weighted mean differences between the survivors and non-survivors (117.4, −13.2–248.0, P < 0.08 and 1.61, −0.14–3.36, P = 0.07, respectively) [25]. On the contrary, Vidal-Cevallos et al. have shown that LDH is associated with worse prognosis in COVID-19 [27]. There are several theoretical concepts supporting the potential utility of LDH:WBC ratio as a biomarker in severe COVID-19, including the burden of unspecific cellular damage (leading to increased LDH) and immune disorder (measured as decreased WBC). This study revealed disagreeing findings about the association of LDH:WBC ratio and all-cause mortality, which were mediated by limited sample size and consequently small effect size. Finally, there was no between-group difference in vaccination status, as well as in COVID-19-related medical management, which strengthens the association of increased CROW-65 values and worse outcomes observed in this study.
Therefore, an important hypothesis-generating findings of a significant association of CROW-65 with all-cause mortality in this study are not surprising; however, due to a limited sample size, retrospective design, small number of events and selected KTR population, clinical applicability of these findings is not certain. Further powered studies should reassess the characteristics of CROW-65 risk score, including predictability, calibration and discrimination. Nevertheless, literature is lacking clinical studies and risk scores for proper stratification of KTR populations with COVID-19, outlining the importance of similar studies to improve the quality of care of these fragile and important patients.
As aforementioned, this study has several limitations. Firstly, single-center data encompassing a relatively small sample size with low number of events could affect results and warrant additional studies. Secondly, the observational retrospective design of this study has inherent limitations, including potential selection bias. Thirdly, original derivation study on CROW-65 risk score has similar limiting factors (small sample size, retrospective design, single-center analysis). The CROW-65 risk score was originally designed on HFNO-treated population which could affect its performance in the remaining KTR population. Similarly, the impact of different pandemic phases and viral strains on CROW-65 risk score performance is not clear. Also, the non-accountable effects of unmeasured variables could not be eliminated. Finally, this study evaluated the performance of CROW-65 on short-term outcomes (≤ 30-day postdischarge) and does not apply to long-term outcomes.
In conclusion, a novel clinical risk score CROW-65 showed significant association with all-cause mortality in KTR patients with COVID-19. Further powered studies should investigate the clinical applicability of CROW-65 risk score in KTR population, including the evaluation of its predictability, calibration and discrimination.
Abbreviations
- AUC:
-
Area under the curve
- BUN:
-
Blood urea nitrogen
- CCI:
-
Charlson comorbidity index
- CKD:
-
Chronic kidney disease
- CRP:
-
C reactive protein
- EGFR:
-
Estimated glomerular filtration rate
- HFNO:
-
High-flow nasal oxygen
- IQR:
-
Interquartile range
- LDH:
-
Lactate dehydrogenase
- PCR:
-
Polymerase chain reaction
- RBC:
-
Red blood cells
- ROC:
-
Receiver operating characteristic
- ROX index:
-
The ratio of oxygen saturation and a fraction of inspired oxygen
- KTR:
-
Kidney transplant recipient
- SPSS:
-
Statistical Package for the Social Sciences
- WBC:
-
White blood cells
References
Gao YD, Ding M, Dong X, Zhang JJ, Azkur KA, Azkur D, et al. Risk factors for severe and critically ill COVID-19 patients: a review. Allergy. 2021;76(2):428–55.
Williamson EJ, Walker AJ, Bhaskaran K, Bacon S, Bates C, Morton CE, et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature. 2020;584(7821):430–6.
ERA-EDTA Council, ERACODA Working Group. Chronic kidney disease is a key risk factor for severe COVID-19: a call to action by the ERA-EDTA. Nephrol Dial Transplant. 2021;36(1):87–94.
Clark A, Jit M, Warren-Gash C, Guthrie B, Wang HHX, Mercer SW, et al. Global, regional, and national estimates of the population at increased risk of severe COVID-19 due to underlying health conditions in 2020: a modelling study. Lancet Glob Health. 2020;8(8):e1003–17.
Caillard S, Chavarot N, Francois H, Matignon M, Greze C, Kamar N, et al. Is COVID-19 infection more severe in kidney transplant recipients? Am J Transplant. 2021;21(3):1295–303.
Raja MA, Mendoza MA, Villavicencio A, Anjan S, Reynolds JM, Kittipibul V, et al. COVID-19 in solid organ transplant recipients: a systematic review and meta-analysis of current literature. Transplant Rev. 2021;35(1):100588.
Hilbrands LB, Duivenvoorden R, Vart P, Franssen CFM, Hemmelder MH, Jager KJ, et al. COVID-19-related mortality in kidney transplant and dialysis patients: results of the ERACODA collaboration. Nephrol Dial Transplant. 2020;35(11):1973–83.
Mahalingasivam V, Craik A, Tomlinson LA, Ge L, Hou L, Wang Q, et al. A systematic review of COVID-19 and kidney transplantation. Kidney Int. 2021;6(1):24–45.
Abolghasemi S, Mardani M, Sali S, Honarvar N, Baziboroun M. COVID-19 and kidney transplant recipients. Transpl Infect Dis. 2020;31:e13413.
Azzi Y, Bartash R, Scalea J, Loarte-Campos P, Akalin E. COVID-19 and solid organ transplantation: a review article. Transplantation. 2021;105(1):37–55.
Jager KJ, Kramer A, Chesnaye NC, Couchoud C, Sánchez-Álvarez JE, Garneata L, et al. Results from the ERA-EDTA Registry indicate a high mortality due to COVID-19 in dialysis patients and kidney transplant recipients across Europe. Kidney Int. 2020;98(6):1540–8.
Cravedi P, Mothi SS, Azzi Y, Haverly M, Farouk SS, Pérez-Sáez MJ, et al. COVID-19 and kidney transplantation: results from the TANGO International Transplant Consortium. Am J Transplant. 2020;20(11):3140–8.
Blanco-Melo D, Nilsson-Payant BE, Liu WC, Uhl S, Hoagland D, Møller R, et al. Imbalanced host response to SARS-CoV‑2 drives development of COVID-19. Cell. 2020;181(5):1036–1045.e9.
Yilmaz G, Ebru O, Ibrahim B, Ulkem C. Assessment of clinical outcomes in renal transplant recipients with COVID-19. J Med Virol. 2021;93(12):6760–4.
Vishnevetsky A, Levy M. Rethinking high-risk groups in COVID-19. Mult Scler Relat Disord. 2020;42:102139.
Modelli de Andrade LG, de Sandes-Freitas TV, Requião-Moura LR, Viana LA, Cristelli MP, Garcia VD, et al. Development and validation of a simple web-based tool for early prediction of COVID-19-associated death in kidney transplant recipients. Am J Transplant. 2022;22(2):610–25.
Kljakovic Gaspic T, Pavicic Ivelja M, Kumric M, Matetic A, Delic N, Vrkic I, et al. In-hospital mortality of COVID-19 patients treated with high-flow nasal oxygen: evaluation of biomarkers and development of the novel risk score model CROW-65. Life. 2021;11(8):735.
Levey AS, Inker LA, Coresh J. GFR estimation: from physiology to public health. Am J Kidney Dis. 2014;63(5):820–34.
Setter NW, Peres ML, de Almeida BMM, Petterle RR, Raboni SM. Charlson comorbidity index scores and in-hospital prognosis of patients with severe acute respiratory infections. Intern Med J. 2020;50(6):691–7.
Hosmer DW, Hosmer T, Lemeshow S. A Goodness-of-Fit Tests for the Multiple Logistic Regression Model. Communications in Statistics. 1980;10:1043–69. https://doi.org/10.1080/03610928008827941.
Harrell FE, Califf RM, Pryor DB, Lee KL, Rosati RA. Evaluating the Yield of Medical Tests. 1982;247(18):2543–6. https://doi.org/10.1001/jama.1982.03320430047030.
Hanley J, McNEil B. The Meaning and Use of the Area under a Receiver Operating Characteristic (ROC) Curve. Radiology. 1982:143;29–36. https://doi.org/10.1148/radiology.143.1.7063747.
King J Jr, Yoon JS, Rentsch CT, Tate JP, Park LS, Kidwai-Khan F, et al. Development and validation of a 30-day mortality index based on pre-existing medical administrative data from 13,323 COVID-19 patients: the Veterans Health Administration COVID-19 (VACO) Index. PLoS ONE. 2020;15(11):e241825–11.
Knight SR, Ho A, Pius R, Buchan I, Carson G, Drake TM, et al. Risk stratification of patients admitted to hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: development and validation of the 4C Mortality Score. BMJ. 2020;370:m3339.
Udomkarnjananun S, Kerr SJ, Townamchai N, Susantitaphong P, Tulvatana W, Praditpornsilpa K, et al. Mortality risk factors of COVID-19 infection in kidney transplantation recipients: a systematic review and meta-analysis of cohorts and clinical registries. Sci Rep. 2021;11(1):20073.
Lemiale V, Dumas G, Demoule A, Pène F, Kouatchet A, Bisbal M, et al. Performance of the ROX index to predict intubation in immunocompromised patients receiving high-flow nasal cannula for acute respiratory failure. Ann Intensive Care. 2021;11:17.
Vidal-Cevallos P, Higuera-De-La-Tijera F, Chávez-Tapia NC, Sanchez-Giron F, Cerda-Reyes E, Rosales-Salyano VH, et al. Lactate-dehydrogenase associated with mortality in hospitalized patients with COVID-19 in Mexico: a multi-centre retrospective cohort study. Ann Hepatol. 2021;24:100338.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
J. Domjanović, A. Matetic, D. Baković Kramarić, T. Domjanović Škopinić, D. Borić Škaro, N. Delić, F. Runjić and I. Jeličić declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Josipa Domjanović and Andrija Matetic contributed equally to the research as joint first authors.
All authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their interpretation.
Supplementary Information
Additional material is provided which contains Supplementary Tables: ;
508_2022_2052_MOESM1_ESM.docx
Supplementary Table 1 (Title: Comparison of symptoms and clinical findings in the study groups; File format: .docx), Supplementary Table 2 (Title: Comparison of ROC curves between different factors; File format: .docx)
508_2022_2052_MOESM5_ESM.pdf
Appendix A includes the Strengthening The Reporting of OBservational Studies in Epidemiology) Checklist; Appendix A (Title: STROBE checklist of the study; File format: .pdf)
Rights and permissions
About this article

{kind=link}
{kind=link}
Cite this article
Domjanović, J., Matetic, A., Baković Kramarić, D. et al. Association of the novel CROW-65 risk score and mortality in hospitalized kidney transplant recipients with COVID-19. Wien Klin Wochenschr 134, 842–849 (2022). https://doi.org/10.1007/s00508-022-02052-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00508-022-02052-9