
Abstract
The two primary manifestations of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in children are acute coronavirus disease 2019 (COVID-19) pneumonia and multisystem inflammatory syndrome (MIS-C). While most pediatric cases of acute COVID-19 disease are mild or asymptomatic, some children are at risk for develo** severe pneumonia. In MIS-C, children present a few weeks after SARS-CoV-2 exposure with a febrile illness that can rapidly progress to shock and multiorgan dysfunction. In both diseases, the clinical and laboratory findings can be nonspecific and present a diagnostic challenge. Thoracic imaging is commonly obtained to assist with initial workup, assessment of disease progression, and guidance of therapy. This paper reviews the radiologic findings of acute COVID-19 pneumonia and MIS-C, highlights the key distinctions between the entities, and summarizes our understanding of the role of imaging in managing SARS-CoV-2-related illness in children.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Coronavirus disease 2019 (COVID-19), the disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was initially reported in late 2019. It subsequently spread rapidly throughout the world in early 2020 and was officially declared a pandemic by the World Health Organization (WHO) on March 11, 2020 [1]. People at highest risk for serious complications and fatality from acute COVID-19 include older adults and those with underlying medical conditions including obesity, diabetes, hypertension, cardiovascular disease and chronic respiratory disease [39, 40]. In children with a complicated disease course requiring imaging to guide therapy, chest radiograph and chest CT are the mainstay modalities being used [41]. Of note, a handful of papers have also reported chest US findings of children with severe COVID-19 infection; however, only a small number of cases have been described, and this technique has not been widely adopted [42].
Classically, chest radiograph is the primary diagnostic imaging tool used to assess for pneumonia in a child presenting with fever and cough. However, there is a paucity of reliable data regarding chest radiograph findings in children with COVID-19 pneumonia because of its low prevalence [39]. There is also high variability in the incidence of abnormal exams and patterns of opacities described in the literature, which further limits our understanding of the radiographic findings [12, 43,44,45,46,47,48,49,50,51,52,53,54]. This could reflect institutional differences in frequency of image utilization, differences in severity of illness among various pediatric study populations (disease severity is not ubiquitously well-documented), and radiologist intra- and interobserver variability (a known challenge in interpretation of pediatric chest radiographs) [50, 55, 56].
A wide variety of findings have been reported on chest radiographs in pediatric COVID-19; however, the most common abnormalities include consolidation, ground-glass opacity and peribronchial thickening [43,44,45,46,47,48,49,50,51,52,53,54]. The opacities can be unilateral or bilateral, focal (singular) or non-focal (multiple, patchy, diffuse), and peripheral or central [43,44,45,46,47,48,49,50,51,52,53] (Figs. 1, 2 and 3). Some studies note a predilection for the lung bases, with equal distribution in the right and left lung [12, 39, 43, 47, 56]. These findings are overall nonspecific, and there is overlap of the classic patterns of viral infection (symmetrical perihilar opacity and peribronchial thickening) and bacterial infection (focal or multifocal dense consolidation) [48, 57]. Of note, pleural effusions and lymphadenopathy are uncommon in pediatric COVID-19 pneumonia [43, 44, 47].

Ground-glass opacities on radiography in acute coronavirus disease 2019 (COVID-19) pneumonia. A 12-year-old obese boy presented with fever, cough and hypoxia. Anteroposterior chest radiograph demonstrates ill-defined ground-glass opacities in both the mid and lower lung fields, with superimposed patchy perihilar consolidation

Radiography of consolidation in acute coronavirus disease 2019 (COVID-19) pneumonia in a 20-year-old man. He presented with fever, cough and dyspnea. Anteroposterior chest radiograph demonstrates multiple confluent regions of consolidation throughout both lungs

Dense consolidation on radiography in acute coronavirus disease 2019 (COVID-19) pneumonia in a 14-year-old boy. The boy had a history of seizure disorder. He presented with fever and respiratory distress. Anteroposterior chest radiograph demonstrates diffuse ground-glass opacification of the lungs, with bilateral perihilar and retrocardiac dense consolidation
The number of studies in the literature describing chest CT in acute COVID-19 pneumonia is significantly greater than for chest radiography. Unfortunately, because of the low incidence of disease in children, these studies focus on small populations, and as with chest radiography there is considerable variability in reported chest CT patterns. Therefore, the role of chest CT in pediatric COVID-19 has not been fully established. Just as with most other pulmonary processes, it is likely that in COVID-19 pneumonia, chest CT is more sensitive in detecting abnormalities that might not be visible on chest radiograph [46]. However, these findings can be subtle and nonspecific, and their presence does not necessarily affect patient management [20, 46]. In adults, typical findings include bilateral multifocal peripheral ground-glass opacities, with or without consolidation, which can be rounded and can demonstrate “crazy paving” (ground-glass opacity with intralobular lines) [58]. “Halo sign” (central dense consolidation with surrounding ground-glass opacity) and “reverse halo sign,” also known as “atoll sign” (central ground-glass opacity with surrounding dense consolidation), have also been reported [58,59,60,61,62]. The primary findings of ground-glass opacity and consolidation are also seen in children, but studies comparing pediatric and adult CT have shown that the opacities in children are less severe with regard to number, size and extent [63,64,65,66].
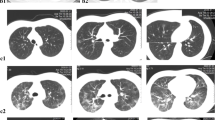
The most common CT abnormalities described in pediatric COVID-19 pneumonia are multiple ground-glass opacities, with or without consolidation, which can be subpleural/peripheral or central in location [45,46,47,48, 51, 54, 56, 63,64,65,66,67,68,69,70,71,72] (Figs. 4 and 5). A “halo sign” has also been reported, and this seems to be more common in children than in adults [54, 64, 65, 68, 69, 72] (Fig. 6). Interstitial-type opacities and small airway-type findings, such as bronchial wall thickening, septal thickening and tree-in-bud nodules, have been described as highly frequent in some studies, but uncommon in other studies [45, 51, 54, 64, 66,67,68]. As with chest radiography, pleural effusions are not usually seen, and when present are typically small in size [45, 51, 56, 67]. An increased risk for pulmonary embolism in COVID-19-infected adults has been well described, but thus far it appears to be uncommon in children [45, 68, 73, 74].

CT findings in acute coronavirus disease 2019 (COVID-19) pneumonia. A 19-year-old obese man presented with fever, cough and hypoxia. Axial chest CT image in lung window demonstrates ground-glass opacities (white arrows), consolidative opacities (black arrows) and subpleural nodular opacities (arrowheads)

CT findings in a 13-year-old boy with acute coronavirus disease 2019 (COVID-19) pneumonia who presented with fever, dyspnea and chest pain. Coronal chest CT image in lung window demonstrates multiple peripheral and central ground-glass opacities throughout both lungs

Halo sign in a 15-year-old asymptomatic boy with osteosarcoma. He underwent surveillance imaging and was subsequently found to have coronavirus disease 2019 (COVID-19) infection by reverse transcriptase polymerase chain reaction (RT-PCR). Axial chest CT image in lung window shows a right lower lobe subpleural nodule with surrounding ground-glass opacity, or halo sign (arrow). The finding resolved on a follow-up scan
Because of the uncertainty of test availability and reliability during the early peak of the pandemic in adults, it was thought that imaging might be a useful tool in primary diagnosis of acute COVID-19. However, despite the presence of a positive RT-PCR test, imaging in children is often normal [20, 75]. When abnormalities are present, there is great diversity and nonspecificity of findings [20, 56, 68, 69, 76, 77]. Moreover, the majority of pediatric studies available in the literature do not adjust for the clinical severity of disease, nor do they take into account possible coexisting infections [20, 56, 76]. These issues limit the meaningfulness of radiographic interpretations in pediatric COVID-19 disease. In a few studies, some data support a link between the severity of pulmonary opacities on imaging and indicators of clinical severity, such as degree of respiratory distress, need for hospital admission and intensive care stay, presence of underlying conditions, and patient fatalities [45, 47, 50, 51, 53, 71, 72]. Thus, while imaging might not play a primary diagnostic role in acute pediatric COVID-19, it remains an integral part of patient care, mainly to assess disease progression or anticipate a change in management, especially in children with critical illness and chronic comorbidities [20, 41, 43, 45, 48].
Imaging findings in multisystem inflammatory syndrome in children
Imaging is not required for diagnosis of MIS-C because the criteria are based on clinical symptoms, laboratory values, history of SARS-CoV-2 infection and exclusion of other conditions [27, 28]. However, radiologic studies are frequently obtained in children with MIS-C because of their rapid clinical deterioration, and imaging abnormalities are important to recognize because they are associated with fulminant illness including shock [29]. Chest radiographs are often obtained in children with MIS-C who are undergoing cardiac workup or being admitted to the intensive care unit. Additionally, because of the high prevalence of gastrointestinal symptoms in this syndrome, abdominal imaging including plain radiograph, US or CT is often obtained, even before the diagnosis of MIS-C is recognized. As the following sections demonstrate, a variety of organ systems can manifest with imaging abnormalities in MIS-C, which reflects the systemic inflammatory response that characterizes this disease.
Intrathoracic imaging findings
Pulmonary
Primary pulmonary involvement is not a leading feature of MIS-C, and therefore at initial presentation, chest imaging might be normal [30, 43]. Within the first few days as the illness evolves, the most common radiographic findings are bilateral symmetrical hazy airspace opacities with perihilar or basilar/lower lobe predominance, as well as increased interstitial markings and peribronchial cuffing/thickening, bilateral small pleural effusions and enlargement of the cardiac silhouette [14, 37, 38, 43, 78,79,80] (Figs. 7 and 8). The underlying etiology of these findings is unclear; however, the appearance is reminiscent of interstitial pulmonary edema or acute respiratory distress syndrome (ARDS), indicating that it could originate from a cardiogenic process, systemic inflammatory process, or aggressive fluid resuscitation and third spacing [14, 37, 76, 80]. Of note, chest radiographs in MIS-C can be abnormal even in children without respiratory symptoms, suggesting that the findings reflect cardiac dysfunction or fluid overload rather than pulmonary inflammation [38, 78,79,80].

Multisystem inflammatory syndrome in children (MIS-C) in an 11-year-old girl who presented with fever, abdominal pain and headache. a, b Posteroanterior (a) and lateral (b) chest radiographs demonstrate a mildly enlarged cardiac silhouette and interstitial edema with basilar-predominant hazy interstitial markings. There are small pleural effusions with blunting of the costophrenic angles and fluid tracking into the fissures (arrowheads)

Multisystem inflammatory syndrome in children (MIS-C) in a 9-year-old girl who presented with fever and abdominal pain. Anteroposterior chest radiograph shows a mildly enlarged cardiac silhouette, interstitial edema with increased interstitial markings and hazy pulmonary opacity, worst at the bases, and bilateral small pleural effusions (arrowheads)
Chest CT is rarely needed in children with MIS-C, although it is sometimes obtained as part of a sepsis workup pathway or if there is clinical concern for pulmonary embolism [37, 38]. Compared to acute COVID-19 pneumonia, there is a paucity of descriptions of MIS-C on CT in the literature; however, existing reports generally mimic the chest radiograph findings. The most common abnormalities include bibasilar consolidation, ground-glass opacities, interstitial opacities including septal thickening and bronchial wall thickening, bilateral small pleural effusions, mild hilar lymphadenopathy, and cardiomegaly [38, 78, 81] (Figs. 9 and 10). Pulmonary nodules have been reported in a few instances and are of uncertain significance [38, 78].

Chest CT findings in a 10-year-old girl with multisystem inflammatory syndrome in children (MIS-C) who presented with fever and chest and abdominal pain. Axial contrast-enhanced chest CT image in soft-tissue window demonstrates cardiomegaly, small pericardial effusion (arrow) and bilateral small pleural effusions (arrowheads)

Chest CT findings in an 18-year-old woman with multisystem inflammatory syndrome in children (MIS-C) who presented with fever and hypoxia. Axial chest CT in lung window demonstrates pulmonary edema with ground-glass opacities, interlobular septal thickening (arrows) and small pleural effusions (arrowheads)
Cardiac
Cardiac imaging is indicated in MIS-C to document baseline systolic function during the initial phase of illness, and for serial follow-up [82]. On echocardiography, children typically demonstrate myocardial dysfunction with depressed ejection fraction [35, 36, 83,84,85,86]. Pericardial effusion and mitral regurgitation have also been described [35, 36, 38, 83,84,85,86,87]. Coronary artery ectasia or aneurysm has been reported in some case series on echocardiogram and cardiac CT angiography, but this is not a universal finding [38, 78, 86,87,88,89].
Cardiac MRI is also suggested for characterizing myocardial disease in children with MIS-C with significant left ventricular dysfunction (ejection fraction <50%) [82]. Limited data are available; however, most studies report a myocarditis-type picture, demonstrated as diffuse myocardial edema or a non-ischemic gadolinium enhancement pattern, without evidence of necrosis or fibrosis [78, 85, 90,91,92]. Fortunately, both the clinical and imaging findings of heart failure in MIS-C appear to be transient, with quick recovery of systolic function and normalization of myocardial signal on MRI [88, 91, 93].
Vascular
It is well established that adults with COVID-19 are vulnerable to vascular complications including multiorgan thromboembolic disease, and based on this assumption, some expert multidisciplinary groups have recommended thromboprophylaxis in children with COVID-19 or MIS-C [94,95,96]. However, there is a lack of consensus on this topic, including whether imaging should be obtained in pursuit of deep venous thrombosis and pulmonary embolism. The greater pro-inflammatory cytokine response and higher plasma D-dimer levels seen in MIS-C suggest that these children are more vulnerable to thromboembolic phenomenon compared to those with acute COVID-19 [74, 97]. It appears from some reports that the incidence of deep venous thrombosis and pulmonary embolism in pediatric SARS-CoV-2-related illnesses is higher than baseline; however, at some institutions, no cases of pulmonary embolism have been documented [21, 37, 38, 74, 98,99,100]. In MIS-C, the known cases of pulmonary embolism have been small and segmental in location, but few papers include information on embolism size or location [37, 93]. There is data to suggest that the existing cases of pediatric SARS-CoV-2-associated thromboembolism are linked to underlying risk factors, such as indwelling central lines, malignancy and ECMO [74, 94, 96, 98, 99].
Extrathoracic imaging findings
Abdominal
Gastrointestinal symptoms are among the most common presenting findings of MIS-C, often mimicking acute appendicitis, and leading to imaging of the abdomen before the diagnosis of MIS-C is considered [38, 88, 101,102,103]. On US and CT, children with MIS-C frequently demonstrate nonspecific inflammatory changes in the right lower quadrant, including lymphadenopathy, mesenteric edema (hyperechogenicity, thickening, stranding) and bowel wall thickening especially at the terminal ileum and cecum [37, 38, 78,79,80, 103,104,105] (Figs. 11, 12 and 13). Some researchers have suggested that the localized right lower quadrant findings in a mesenteric adenitis pattern is due to the abundant lymphoid tissue in the terminal ileum (Peyer patches), which is vulnerable to vasculitis and necrotizing lymphadenitis caused by the systemic hyperinflammatory illness [38, 78, 102, 105]. The appendix can appear radiologically normal or abnormal, and imaging cannot always clearly distinguish between MIS-C and acute appendicitis [38, 79, 101, 104, 106,107,108]. Therefore, these findings must be considered in light of multiorgan involvement and laboratory data that would support a diagnosis of MIS-C.

Abdominal US findings in a 9-year-old girl with multisystem inflammatory syndrome in children (MIS-C) who presented with fever and abdominal pain. a Transverse US image of the right lower quadrant shows multiple enlarged lymph nodes (N), with thickening and increased echogenicity of the surrounding mesenteric fat (*). P psoas muscle. b Sagittal US image of the right lower quadrant shows thick-walled bowel (arrowheads)

Abdominal CT findings in a 13-year-old boy with multisystem inflammatory syndrome in children (MIS-C) who presented with fever, abdominal pain and tachycardia. Coronal contrast-enhanced abdominal CT image demonstrates multiple enlarged right lower quadrant lymph nodes (arrows) and stranding of the surrounding mesenteric fat (arrowheads). A small amount of pelvic ascites is also present (*)

Mural thickening in a 16-year-old boy with multisystem inflammatory syndrome in children (MIS-C) who presented with right lower quadrant abdominal pain. Coronal contrast-enhanced abdominal CT image demonstrates mural thickening of the terminal ileum (arrowheads), cecum and ascending colon (arrows)
Other common abdominal imaging findings of MIS-C include small-volume simple ascites, gallbladder wall thickening and pericholecystic fluid, gallbladder sludge and urinary bladder wall thickening [37, 79, 104] (Figs. 12 and 14). Hepatosplenomegaly, periportal edema, hyperechogenic kidneys, and splenic hypoechoic lesions or infarcts have also been reported [37, 38, 79, 104].

US findings in a 6-year-old boy with multisystem inflammatory syndrome in children (MIS-C) who presented with fever and abdominal pain. Sagittal US image of the right upper quadrant shows edematous thickening of the gallbladder (GB) wall and a small amount of pericholecystic fluid (arrow)
Neurologic
Brain imaging in MIS-C is usually normal, but recently there have been increasing reports of MRI signal abnormalities, specifically involving the splenium of the corpus callosum, on T2-weighted sequences, fluid-attenuated inversion recovery (FLAIR) sequences and diffusion-weighted imaging [14, 78, 79, 109,110,111,112,113]. Splenial lesions have also been reported in children with COVID-19 infection who present with only neurologic symptoms and no respiratory symptoms [114]. Other neuroimaging findings reported in MIS-C include cerebral infarcts, encephalomyelitis or acute disseminated encephalomyelitis (ADEM)-like lesions, leptomeningeal enhancement, venous sinus thrombosis, papilledema and Guillain–Barré syndrome-like findings [14, 38, 78,79,80, 90, 112, 113].
Miscellaneous
Neck pain has been reported in more than one-quarter of children with MIS-C, along with other otolaryngologic symptoms such as neck swelling, dysphagia, trismus, stridor and drooling [115,116,117]. Cervical imaging with US or contrast-enhanced CT might be requested to assess for signs of inflammation. The most common abnormalities are retropharyngeal edema and cervical lymphadenopathy [14, 22, 80, 81, 115, 118] (Fig. 15).

Neck findings in a 7-year-old girl with multisystem inflammatory syndrome in children (MIS-C) who presented with fever, neck swelling, rash and conjunctivitis. Axial contrast-enhanced neck CT image demonstrates retropharyngeal edema (arrow) and cervical lymphadenopathy (arrowheads)
Conclusion
While the vast majority of children with COVID-19 disease experience minimal to no symptoms, in rare cases a pediatric patient presents with severe illness after known SARS-CoV-2 exposure, and the differential diagnosis includes both severe COVID-19 pneumonia and MIS-C. Either of these conditions can present with fever and respiratory distress progressing to shock. Therefore, it is important for pediatricians and radiologists to understand the differences in their clinical and radiologic profiles so they can make a prompt diagnosis. The key distinctions between these entities are summarized in Table 1 [14, 22, 34, 43, 93, 119, 120]. With regard to thoracic imaging, children with MIS-C demonstrate a diffuse pattern of hazy pulmonary opacity with interstitial edema and small pleural effusions secondary to heart failure, whereas children with acute COVID-19 infection demonstrate heterogeneous patterns of ground glass, consolidation and nodules. Imaging findings of intrabdominal inflammation are also distinct and highly prevalent in MIS-C. Recognition of these various features allows for early diagnosis and appropriately targeted management of SARS-CoV-2-associated critical illness in children.
References
World Health Organization (2020) WHO director-general's opening remarks at the media briefing on COVID-19. https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19%2D%2D-11-march-2020. Accessed 24 Oct 2021
Cao Y, Liu X, **ong L, Cai K (2020) Imaging and clinical features of patients with 2019 novel coronavirus SARS-CoV-2: a systematic review and meta-analysis. J Med Virol 92:1449–1459
Wu Z, McGoogan JM (2020) Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72,314 cases from the Chinese Center for Disease Control and Prevention. JAMA 323:1239–1242
Centers for Disease Control and Prevention (2021) Underlying medical conditions associated with high risk for severe COVID-19: information for healthcare providers. https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/underlyingconditions.html. Accessed 26 Oct 2021
Centers for Disease Control and Prevention (2021) Science brief: evidence used to update the list of underlying medical conditions that increase a person's risk of severe illness from COVID-19. https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/underlying-evidence-table.html. Accessed 26 Oct 2021
Carsetti R, Quintarelli C, Quinti I et al (2020) The immune system of children: the key to understanding SARS-CoV-2 susceptibility? Lancet Child Adolesc Health 4:414–416
Jiang L, Tang K, Levin M et al (2020) COVID-19 and multisystem inflammatory syndrome in children and adolescents. Lancet Infect Dis 20:e276–e288
Dong Y, Mo X, Hu Y et al (2020) Epidemiology of COVID-19 among children in China. Pediatrics 145:e20200702
Zimmermann P, Curtis N (2020) Coronavirus infections in children including COVID-19: an overview of the epidemiology, clinical features, diagnosis, treatment and prevention options in children. Pediatr Infect Dis J 39:355–368
Badal S, Thapa Bajgain K, Badal S et al (2021) Prevalence, clinical characteristics, and outcomes of pediatric COVID-19: a systematic review and meta-analysis. J Clin Virol 135:104715
Rothan HA, Byrareddy SN (2020) The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J Autoimmun 109:102433
Blumfield E, Levin TL (2020) COVID-19 in pediatric patients: a case series from the Bronx, NY. Pediatr Radiol 50:1369–1374
Ludvigsson JF (2020) Systematic review of COVID-19 in children shows milder cases and a better prognosis than adults. Acta Paediatr 109:1088–1095
Rostad BS, Shah JH, Rostad CA et al (2021) Chest radiograph features of multisystem inflammatory syndrome in children (MIS-C) compared to pediatric COVID-19. Pediatr Radiol 51:231–238
She J, Liu L, Liu W (2020) COVID-19 epidemic: disease characteristics in children. J Med Virol 92:747–754
Castagnoli R, Votto M, Licari A et al (2020) Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in children and adolescents: a systematic review. JAMA Pediatr 174:882–889
Yasuhara J, Kuno T, Takagi H, Sumitomo N (2020) Clinical characteristics of COVID-19 in children: a systematic review. Pediatr Pulmonol 55:2565–2575
Tsankov BK, Allaire JM, Irvine MA et al (2021) Severe COVID-19 infection and pediatric comorbidities: a systematic review and meta-analysis. Int J Infect Dis 103:246–256
Derespina KR, Kaushik S, Plichta A et al (2020) Clinical manifestations and outcomes of critically ill children and adolescents with coronavirus disease 2019 in new York City. J Pediatr 226:55–63.e2
Shelmerdine SC, Lovrenski J, Caro-Dominguez P et al (2020) Coronavirus disease 2019 (COVID-19) in children: a systematic review of imaging findings. Pediatr Radiol 50:1217–1230
Dufort EM, Koumans EH, Chow EJ et al (2020) Multisystem inflammatory syndrome in children in New York State. N Engl J Med 383:347–358
Feldstein LR, Rose EB, Horwitz SM et al (2020) Multisystem inflammatory syndrome in U.S. children and adolescents. N Engl J Med 383:334–346
Viner RM, Whittaker E (2020) Kawasaki-like disease: emerging complication during the COVID-19 pandemic. Lancet 395:1741–1743
Riphagen S, Gomez X, Gonzalez-Martinez C et al (2020) Hyperinflammatory shock in children during COVID-19 pandemic. Lancet 395:1607–1608
Verdoni L, Mazza A, Gervasoni A et al (2020) An outbreak of severe Kawasaki-like disease at the Italian epicentre of the SARS-CoV-2 epidemic: an observational cohort study. Lancet 395:1771–1778
Soma VL, Shust GF, Ratner AJ (2021) Multisystem inflammatory syndrome in children. Curr Opin Pediatr 33:152–158
Centers for Disease Control and Prevention Health Alert Network (2020) Multisystem inflammatory syndrome in children (MIS-C) Associated with coronavirus disease 2019 (COVID-19). https://emergency.cdc.gov/han/2020/han00432.asp. Accessed 26 Oct 2021
World Health Organization (2020) Multisystem inflammatory syndrome in children and adolescents temporally related to COVID-19. https://www.who.int/news-room/commentaries/detail/multisystem-inflammatory-syndrome-in-children-and-adolescents-with-covid-19. Accessed 26 Oct 2021
Bautista-Rodriguez C, Sanchez-de-Toledo J, Clark BC et al (2021) Multisystem inflammatory syndrome in children: an international survey. Pediatrics 147:e2020024554
Radia T, Williams N, Agrawal P et al (2021) Multi-system inflammatory syndrome in children & adolescents (MIS-C): a systematic review of clinical features and presentation. Paediatr Respir Rev 38:51–57
Reiff DD, Mannion ML, Samuy N et al (2021) Distinguishing active pediatric COVID-19 pneumonia from MIS-C. Pediatr Rheumatol Online J 19:21
Rowley AH (2020) Understanding SARS-CoV-2-related multisystem inflammatory syndrome in children. Nat Rev Immunol 20:453–454
Toraih EA, Hussein MH, Elshazli RM et al (2021) Multisystem inflammatory syndrome in pediatric COVID-19 patients: a meta-analysis. World J Pediatr 17:141–151
Duarte-Neto AN, Caldini EG, Gomes-Gouvêa MS et al (2021) An autopsy study of the spectrum of severe COVID-19 in children: from SARS to different phenotypes of MIS-C. EClinicalMedicine 35:100850
Alsaied T, Tremoulet AH, Burns JC et al (2021) Review of cardiac involvement in multisystem inflammatory syndrome in children. Circulation 143:78–88
Kaushik S, Aydin SI, Derespina KR et al (2020) Multisystem inflammatory syndrome in children associated with severe acute respiratory syndrome coronavirus 2 infection (MIS-C): a multiinstitutional study from New York City. J Pediatr 224:24–29
Blumfield E, Levin TL, Kurian J et al (2021) Imaging findings in multisystem inflammatory syndrome in children (MIS-C) associated with coronavirus disease (COVID-19). AJR Am J Roentgenol 216:507–517
Hameed S, Elbaaly H, Reid CEL et al (2021) Spectrum of imaging findings at chest radiography, US, CT, and MRI in multisystem inflammatory syndrome in children associated with COVID-19. Radiology 298:E1–e10
Foust AM, Phillips GS, Chu WC et al (2020) International expert consensus statement on chest imaging in pediatric COVID-19 patient management: imaging findings, imaging study reporting, and imaging study recommendations. Radiol Cardiothorac Imaging 2:e200214
American College of Radiology (2020) ACR recommendations for the use of chest radiography and computed tomography (CT) for suspected COVID-19 infection. https://www.acr.org/Advocacy-and-Economics/ACR-Position-Statements/Recommendations-for-Chest-Radiography-and-CT-for-Suspected-COVID19-Infection. Accessed 26 Oct 2021
Foust AM, McAdam AJ, Chu WC et al (2020) Practical guide for pediatric pulmonologists on imaging management of pediatric patients with COVID-19. Pediatr Pulmonol 55:2213–2224
Caroselli C, Blaivas M, Falzetti S (2021) Diagnostic imaging in newborns, children and adolescents infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2): is there a realistic alternative to lung high-resolution computed tomography (HRCT) and chest X-rays? A systematic review of the literature. Ultrasound Med Biol 47:3034–3040
Biko DM, Ramirez-Suarez KI, Barrera CA et al (2021) Imaging of children with COVID-19: experience from a tertiary children's hospital in the United States. Pediatr Radiol 51:239–247
Oterino Serrano C, Alonso E, Andres M et al (2020) Pediatric chest X-ray in COVID-19 infection. Eur J Radiol 131:109236
Caro-Dominguez P, Shelmerdine SC, Toso S et al (2020) Thoracic imaging of coronavirus disease 2019 (COVID-19) in children: a series of 91 cases. Pediatr Radiol 50:1354–1368
Das KM, Alkoteesh JA, Al Kaabi J et al (2021) Comparison of chest radiography and chest CT for evaluation of pediatric COVID-19 pneumonia: does CT add diagnostic value? Pediatr Pulmonol 56:1409–1418
Palabiyik F, Kokurcan SO, Hatipoglu N et al (2020) Imaging of COVID-19 pneumonia in children. Br J Radiol 93:20200647
Li VR, Sura A, Pickering T (2021) Evaluating current chest imaging practices of pediatric patients with COVID-19: a retrospective analysis. Clin Imaging 80:300–303
Bayramoglu Z, Canipek E, Comert RG et al (2021) Imaging features of pediatric COVID-19 on chest radiography and chest CT: a retrospective, single-center study. Acad Radiol 28:18–27
Ugas-Charcape CF, Ucar ME, Almanza-Aranda J et al (2021) Pulmonary imaging in coronavirus disease 2019 (COVID-19): a series of 140 Latin American children. Pediatr Radiol 51:1597–1607
Romberg EK, Menashe SJ, Kronman MP et al (2021) Pediatric radiologic manifestations of COVID-19. Clin Imaging 75:165–170
Aguirre Pascual E, Coca Robinot D, Gallego Herrero C et al (2021) Pediatric chest X-rays during the COVID-19 pandemic. Radiologia 63:106–114
Erat T, Guler S (2021) Use of radiological tests in COVID-19 positive child cases: is chest computed tomography necessary? Int J Clin Pract 75:e14259
Bayramoglu Z, Canıpek E, Comert RG et al (2021) Imaging features of pediatric COVID-19 on chest radiography and chest CT: a retrospective, single-center study. Acad Radiol 28:18–27
Neuman MI, Lee EY, Bixby S et al (2012) Variability in the interpretation of chest radiographs for the diagnosis of pneumonia in children. J Hosp Med 7:294–298
Nino G, Zember J, Sanchez-Jacob R et al (2021) Pediatric lung imaging features of COVID-19: a systematic review and meta-analysis. Pediatr Pulmonol 56:252–263
Eslamy HK, Newman B (2011) Pneumonia in normal and immunocompromised children: an overview and update. Radiol Clin N Am 49:895–920
Simpson S, Kay FU, Abbara S et al (2020) Radiological Society of North America expert consensus document on reporting chest CT findings related to COVID-19: endorsed by the Society of Thoracic Radiology, the American College of Radiology, and RSNA. Radiol Cardiothorac Imaging 2:e200152
Bernheim A, Mei X, Huang M et al (2020) Chest CT findings in coronavirus disease-19 (COVID-19): relationship to duration of infection. Radiology 295:200463
Salehi S, Abedi A, Balakrishnan S, Gholamrezanezhad A (2020) Coronavirus disease 2019 (COVID-19): a systematic review of imaging findings in 919 patients. AJR Am J Roentgenol 215:87–93
Li Y, **a L (2020) Coronavirus disease 2019 (COVID-19): role of chest CT in diagnosis and management. AJR Am J Roentgenol 214:1280–1286
Wu J, Pan J, Teng D et al (2020) Interpretation of CT signs of 2019 novel coronavirus (COVID-19) pneumonia. Eur Radiol 30:5455–5462
Chen Z, Fan H, Cai J et al (2020) High-resolution computed tomography manifestations of COVID-19 infections in patients of different ages. Eur J Radiol 126:108972
**a W, Shao J, Guo Y et al (2020) Clinical and CT features in pediatric patients with COVID-19 infection: different points from adults. Pediatr Pulmonol 55:1169–1174
Zang ST, Han X, Cui Q et al (2021) Imaging characteristics of coronavirus disease 2019 (COVID-19) in pediatric cases: a systematic review and meta-analysis. Transl Pediatr 10:1–16
Chen A, Huang JX, Liao Y et al (2020) Differences in clinical and imaging presentation of pediatric patients with COVID-19 in comparison with adults. Radiol Cardiothorac Imaging 2:e200117
Duan YN, Zhu YQ, Tang LL, Qin J (2020) CT features of novel coronavirus pneumonia (COVID-19) in children. Eur Radiol 30:4427–4433
Simoni P, Bazzocchi A, Boitsios G et al (2020) Chest computed tomography (CT) features in children with reverse transcription-polymerase chain reaction (RT-PCR)-confirmed COVID-19: a systematic review. J Med Imaging Radiat Oncol 64:649–659
Steinberger S, Lin B, Bernheim A et al (2020) CT features of coronavirus disease (COVID-19) in 30 pediatric patients. AJR Am J Roentgenol 215:1303–1311
Li Y, Cao J, Zhang X et al (2020) Chest CT imaging characteristics of COVID-19 pneumonia in preschool children: a retrospective study. BMC Pediatr 20:227
Hoseinyazdi M, Esmaeilian S, Jahankhah R et al (2021) Clinical, laboratory, and chest CT features of severe versus non-severe pediatric patients with COVID-19 infection among different age groups. BMC Infect Dis 21:560
Peng X, Guo Y, **ao H et al (2021) Overview of chest involvement at computed tomography in children with coronavirus disease 2019 (COVID-19). Pediatr Radiol 51:222–230
Suh YJ, Hong H, Ohana M et al (2021) Pulmonary embolism and deep vein thrombosis in COVID-19: a systematic review and meta-analysis. Radiology 298:E70–E80
Whitworth H, Sartain SE, Kumar R et al (2021) Rate of thrombosis in children and adolescents hospitalized with COVID-19 or MIS-C. Blood 138:190–198
Hu Z, Song C, Xu C et al (2020) Clinical characteristics of 24 asymptomatic infections with COVID-19 screened among close contacts in Nan**g, China. Sci China Life Sci 63:706–711
Trout AT, Westra SJ (2021) Imaging in support of the clinical diagnoses of COVID-19 and multisystem inflammatory syndrome in children. Pediatr Radiol 51:693–694
Merkus P, Klein WM (2020) The value of chest CT as a COVID-19 screening tool in children. Eur Respir J 55:2001241
Caro-Domínguez P, Navallas M, Riaza-Martin L et al (2021) Imaging findings of multisystem inflammatory syndrome in children associated with COVID-19. Pediatr Radiol 51:1608–1620
Palabiyik F, Akcay N, Sevketoglu E et al (2021) Imaging of multisystem inflammatory disease in children (MIS-C) associated with COVID-19. Acad Radiol 28:1200–1208
Fenlon EP III, Chen S, Ruzal-Shapiro CB et al (2021) Extracardiac imaging findings in COVID-19-associated multisystem inflammatory syndrome in children. Pediatr Radiol 51:831–839
Yurttutan N, Kızıldağ B, Güllü UU (2021) Radiologic manifestations of multisystem inflammatory syndrome in children. AJR Am J Roentgenol 217:W8
Henderson LA, Canna SW, Friedman KG et al (2021) American College of Rheumatology clinical guidance for multisystem inflammatory syndrome in children associated with SARS-CoV-2 and hyperinflammation in pediatric COVID-19: version 2. Arthritis Rheumatol 73:e13–e29
Ahmed M, Advani S, Moreira A et al (2020) Multisystem inflammatory syndrome in children: a systematic review. EClinicalMedicine 26:100527
Matsubara D, Kauffman HL, Wang Y et al (2020) Echocardiographic findings in pediatric multisystem inflammatory syndrome associated with COVID-19 in the United States. J Am Coll Cardiol 76:1947–1961
Theocharis P, Wong J, Pushparajah K et al (2020) Multimodality cardiac evaluation in children and young adults with multisystem inflammation associated with COVID-19. Eur Heart J Cardiovasc Imaging 22:896–903
Valverde I, Singh Y, Sanchez-de-Toledo J et al (2021) Acute cardiovascular manifestations in 286 children with multisystem inflammatory syndrome associated with COVID-19 infection in Europe. Circulation 143:21–32
Sperotto F, Friedman KG, Son MBF et al (2021) Cardiac manifestations in SARS-CoV-2-associated multisystem inflammatory syndrome in children: a comprehensive review and proposed clinical approach. Eur J Pediatr 180:307–322
Belhadjer Z, Méot M, Bajolle F et al (2020) Acute heart failure in multisystem inflammatory syndrome in children in the context of global SARS-CoV-2 pandemic. Circulation 142:429–436
Ramcharan T, Nolan O, Lai CY et al (2020) Paediatric inflammatory multisystem syndrome: temporally associated with SARS-CoV-2 (PIMS-TS): cardiac features, management and short-term outcomes at a UK tertiary paediatric hospital. Pediatr Cardiol 41:1391–1401
Mavrogeni SI, Kolovou G, Tsirimpis V et al (2021) The importance of heart and brain imaging in children and adolescents with multisystem inflammatory syndrome in children (MIS-C). Rheumatol Int 41:1037–1044
Blondiaux E, Parisot P, Redheuil A et al (2020) Cardiac MRI in children with multisystem inflammatory syndrome associated with COVID-19. Radiology 297:E283–e288
Sirico D, Basso A, Reffo E et al (2021) Early echocardiographic and cardiac MRI findings in multisystem inflammatory syndrome in children. J Clin Med 10:3360
Winant AJ, Blumfield E, Liszewski MC et al (2020) Thoracic imaging findings of multisystem inflammatory syndrome in children associated with COVID-19: what radiologists need to know now. Radiol Cardiothorac Imaging 2:e200346
Goldenberg NA, Sochet A, Albisetti M et al (2020) Consensus-based clinical recommendations and research priorities for anticoagulant thromboprophylaxis in children hospitalized for COVID-19-related illness. J Thromb Haemost 18:3099–3105
Kanmaniraja D, Kurian J, Holder J et al (2021) Review of COVID-19, part 1: abdominal manifestations in adults and multisystem inflammatory syndrome in children. Clin Imaging 80:88–110
Loi M, Branchford B, Kim J et al (2020) COVID-19 anticoagulation recommendations in children. Pediatr Blood Cancer 67:e28485
Del Borrello G, Giraudo I, Bondone C et al (2021) SARS-CoV-2-associated coagulopathy and thromboembolism prophylaxis in children: a single-center observational study. J Thromb Haemost 19:522–530
Zaffanello M, Piacentini G, Nosetti L et al (2021) Thrombotic risk in children with COVID-19 infection: a systematic review of the literature. Thromb Res 205:92–98
Chima M, Williams D, Thomas NJ, Krawiec C (2021) COVID-19-associated pulmonary embolism in pediatric patients. Hosp Pediatr 11:e90–e94
Tran VL, Parsons S, Varela CR (2021) The trilogy of SARS-CoV-2 in pediatrics (part 3): thrombosis, anticoagulant, and antiplatelet considerations. J Pediatr Pharmacol Ther 26:565–576
Tullie L, Ford K, Bisharat M et al (2020) Gastrointestinal features in children with COVID-19: an observation of varied presentation in eight children. Lancet Child Adolesc Health 4:e19–e20
Jackson RJ, Chavarria HD, Hacking SM (2020) A case of multisystem inflammatory syndrome in children mimicking acute appendicitis in a COVID-19 pandemic area. Cureus 12:e10722
Miller J, Cantor A, Zachariah P et al (2020) Gastrointestinal symptoms as a major presentation component of a novel multisystem inflammatory syndrome in children that is related to coronavirus disease 2019: a single center experience of 44 cases. Gastroenterology 159:1571–1574.e1572
Morparia K, Park MJ, Kalyanaraman M et al (2021) Abdominal imaging findings in critically ill children with multisystem inflammatory syndrome associated with COVID-19. Pediatr Infect Dis J 40:e82–e83
Sahn B, Eze OP, Edelman MC et al (2021) Features of intestinal disease associated with COVID-related multisystem inflammatory syndrome in children. J Pediatr Gastroenterol Nutr 72:384–387
Manz N, Höfele-Behrendt C, Bielicki J et al (2021) MIS-C-implications for the pediatric surgeon: an algorithm for differential diagnostic considerations. Children 8:712
Hofto ME, Schmit EO, Sharma M, Samuy N (2021) Acute appendicitis associated with multisystem inflammatory syndrome in children. Cureus 13:e15893
Yock-Corrales A, Lenzi J, Ulloa-Gutiérrez R et al (2021) Acute abdomen and appendicitis in 1,010 pediatric patients with COVID-19 or MIS-C: a multinational experience from Latin America. Pediatr Infect Dis J 40:e364–e369
Lin J, Lawson EC, Verma S et al (2020) Cytotoxic lesion of the corpus callosum in an adolescent with multisystem inflammatory syndrome and SARS-CoV-2 infection. AJNR Am J Neuroradiol 41:2017–2019
Bektaş G, Akçay N, Boydağ K, Şevketoğlu E (2021) Reversible splenial lesion syndrome associated with SARS-CoV-2 infection in two children. Brain Dev 43:230–233
Nepal G, Shrestha GS, Rehrig JH et al (2021) Neurological manifestations of COVID-19 associated multi-system inflammatory syndrome in children: a systematic review and meta-analysis. J Nepal Health Res Counc 19:10–18
Siracusa L, Cascio A, Giordano S et al (2021) Neurological complications in pediatric patients with SARS-CoV-2 infection: a systematic review of the literature. Ital J Pediatr 47:123
LaRovere KL, Riggs BJ, Poussaint TY et al (2021) Neurologic involvement in children and adolescents hospitalized in the United States for COVID-19 or multisystem inflammatory syndrome. JAMA Neurol 78:536–547
Abdel-Mannan O, Eyre M, Löbel U et al (2020) Neurologic and radiographic findings associated with COVID-19 infection in children. JAMA Neurol 77:1440–1445
Jenkins E, Sherry W, Smith AGC et al (2021) Retropharyngeal edema and neck pain in multisystem inflammatory syndrome in children (MIS-c). J Pediatric Infect Dis Soc 10:922–925
Cheong RCT, Jephson C, Frauenfelder C et al (2021) Otolaryngologic manifestations in pediatric inflammatory multisystem syndrome temporally associated with COVID-19. JAMA Otolaryngol Head Neck Surg 147:482–484
Carlin RF, Fischer AM, Pitkowsky Z et al (2021) Discriminating multisystem inflammatory syndrome in children requiring treatment from common febrile conditions in outpatient settings. J Pediatr 229:26–32.e22
Daube A, Rickert S, Madan RP et al (2021) Multisystem inflammatory syndrome in children (MIS-C) and retropharyngeal edema: a case series. Int J Pediatr Otorhinolaryngol 144:110667
Rubens JH, Akindele NP, Tschudy MM, Sick-Samuels AC (2021) Acute COVID-19 and multisystem inflammatory syndrome in children. BMJ 372:n385
Diorio C, Henrickson SE, Vella LA et al (2020) Multisystem inflammatory syndrome in children and COVID-19 are distinct presentations of SARS-CoV-2. J Clin Invest 130:5967–5975
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kurian, J., Blumfield, E., Levin, T.L. et al. Imaging findings in acute pediatric coronavirus disease 2019 (COVID-19) pneumonia and multisystem inflammatory syndrome in children (MIS-C). Pediatr Radiol 52, 1985–1997 (2022). https://doi.org/10.1007/s00247-022-05393-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-022-05393-9