
Abstract
Background
It is not known if the endogenous surfactant pool available early in life is associated with the RDS clinical course in preterm neonates treated with CPAP. We aim to clarify the clinical factors affecting surfactant pool in preterm neonates and study its association with CPAP failure.
Methods
Prospective, pragmatic, blind, cohort study. Gastric aspirates were obtained (within the first 6 h of life and before the first feeding) from 125 preterm neonates with RDS. Surfactant pool was measured by postnatal automated lamellar body count based on impedancemetry, without any pre-analytical treatment. A formal respiratory care protocol based on European guidelines was applied. Clinical data and perinatal risk factors influencing RDS severity or lamellar body count were real-time recorded. Investigators performing lamellar body count were blind to the clinical data and LBC was not used in clinical practice.
Results
Multivariate analysis showed gestational age to be the only factor significantly associated with lamellar body count (standardized β:0.233;p = 0.023). Lamellar body count was significantly higher in neonates with CPAP success (43.500 [23.750–93.750]bodies/μL), than in those failing CPAP (20.500 [12.250–49.750] bodies/μL;p = 0.0003).LBC had a moderate reliability to detect CPAP failure (AUC: 0.703 (0.615–0.781);p < 0.0001; best cut-off: ≤30,000 bodies/μL). Upon adjustment for possible confounders, neither lamellar body count, nor its interaction factor with gestational age resulted associated with CPAP failure.
Conclusions
Early postnatal lamellar body count on gastric aspirates in CPAP-treated preterm neonates with RDS is significantly influenced only by gestational age. Lamellar bodies are not associated with CPAP failure. Thus, the endogenous surfactant pool available early in life only has a moderate reliability to predict CPAP failure.
Similar content being viewed by others


Background
Antenatal corticosteroid prophylaxis and early application of continuous positive airway pressure (CPAP) are considered the gold standard for, respectively, the prevention and treatment of respiratory distress syndrome (RDS) in preterm neonates [1, 2]. Surfactant replacement is recommended when CPAP fails [3, 4] and, if performed within the first 3 h of life, reduces death and/or bronchopulmonary dysplasia [5]. Surfactant is commonly administered based on inspired oxygen fraction (FiO2) [3], however, the suggested FiO2 thresholds are arbitrary, they can be reached beyond the optimal 3 h-time window and they lack of any physiopathological background. Moreover, contemporaneous measurement of oxygen saturation or PaO2 might be needed to accurately describe oxygenation. The CPAP level may also influence oxygenation, through its effect on the lung aeration. In fact, both recent pediatric and neonatal acute respiratory distress syndrome (ARDS) definitions include these variables in appropriate indexes [6, 7].
The available endogenous surfactant also influences lung aeration and, therefore, assessing the surfactant pool available early in life could be interesting to better understand the clinical picture and eventually guide surfactant replacement. Lamellar bodies are intracellular, easily measurable, surfactant storage granules released from type II-pneumocytes [8, 9]. Once in the alveolar space, lamellar bodies are subjected to the breathing cycle and form the surfactant layer adsorbed at the gas/liquid interface [9, 10]. Thus, lamellar body count (LBC) is an estimation of the available endogenous surfactant. LBC correlates with lung aeration evaluated by a semi-quantitative lung ultrasound score [11, 12]. LBC can be realized on amniotic fluid and is used as prenatal lung maturity test, as it has a good reliability to predict the RDS occurrence [13, 14], but is also doable postnatally (at the delivery or using gastric aspirates obtained before the first feeding) [15,16,17].
Despite this physiopathological background, the link between the available surfactant pool and the CPAP failure has never been investigated. Our purposes are: 1) to clarify what are the clinical factors affecting early postnatal LBC in CPAP-treated preterm neonates with RDS; and 2) to investigate reliability of postnatal LBC and its association to CPAP failure.
Methods
Patients
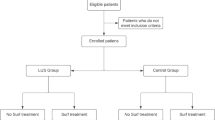
We designed a pragmatic, observational, blind, prospective cohort study. The study was conducted during 2014–2015 in an academic tertiary referral neonatal intensive care unit (NICU). All inborn preterm neonates (< 37 weeks’ gestation) with RDS treated with nasal CPAP were eligible for the study. In detail, RDS was diagnosed when the following criteria [6] were met: 1) occurrence of respiratory distress within the first 24 h of life; 2) presence of typical lung ultrasound or chest X-rays findings; [18, 19] 3) complete, sustained and prompt oxygenation improvement after surfactant replacement or significant improvement under CPAP which prevented surfactant administration; 4) no other respiratory disorders, as detailed below.
Exclusion criteria were: 1) chromosomal abnormalities or complex congenital malformations; 2) congenital lung diseases; 3) need for surgery in the first week of life;
4) early onset severe sepsis/septic shock, as defined elsewhere; [20] 5) transient tachypnea of the neonate, defined as mild (Silverman score ≤ 3) respiratory distress occurring in a neonate of more than 34 weeks’ gestation presenting with typical lung ultrasound or chest X-rays findings and resolving within the first 72 h of life; [6, 18, 19] 6) meconium aspiration syndrome, defined as the presence of meconium-stained amniotic fluid and airway secretions, occurrence of respiratory failure early from birth and typical lung imaging; [21] 7) blood aspiration syndrome, defined as respiratory distress and blood-stained amniotic fluid and airway secretions, onset of respiratory failure early from birth and typical lung imaging; [22] 8) pulmonary haemorrhage, defined as respiratory distress suddenly occurring together with bright blood-stained airway secretions, presence of left-to-right ductal shunting and typical lung imaging; [40]. Thus, we used a quick assay to estimate surfactant pool, in a homogeneous population of preterm babies with RDS without any other respiratory disorders and subjected to good perinatal care and a formal, modern, respiratory care protocol. This is representative of the usual neonatal care in developed countries. We cannot evaluate the effect of maternal diabetes or hypothyroidism, as few or no cases presented with these disorders. Nonetheless, we have been able to evaluate all other major clinical factors influencing endogenous surfactant pool and clinical picture of RDS in preterm neonates. It would have been interesting to deeply study the reliability of LBC in different classes of gestational age and, particularly, in extremely preterm neonates who are more likely to need a “guided” surfactant therapy. However, we did not have a large enough population and a preliminary subgroup analysis did not seem to show any difference. This analysis could have been biased and may need to be repeated in larger populations. However, the availability of more accurate tools (such as semiquantitative lung ultrasound and the surfactant adsorption or microbubble tests) reduces the interest in this regard [11, 12, 38, 41]. Finally, ours is a relatively small population but comparable to those of other studies in the field [14].
Conclusion
Early life LBC on gastric aspirates in CPAP-treated preterm neonates with RDS is significantly influenced by gestational age. LBC is not associated with CPAP failure. Thus, the endogenous surfactant pool available early in life only has a moderate reliability to predict CPAP failure. Further studies are needed to better clarify the biological factors associated to CPAP failure in similar populations.
Abbreviations
- aRR:
-
Adjusted relative risks
- AUC:
-
Area under the curve
- CPAP:
-
Continuous positive airway pressure
- FiO2 :
-
Inspired oxygen fraction
- LBC:
-
Lamellar body count
- NICU:
-
Neonatal intensive care unit
- RDS:
-
Respiratory distress syndrome
- ROC:
-
Receiver operating characteristic
- SGA:
-
Small for gestational age
References
Roberts D, Brown J, Medley N, Dalziel SR. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Pregnancy and Childbirth Group, editor. Cochrane Database Syst Rev [Internet]. 2017 [cited 2018 May 25]; Available from: http://doi.wiley.com/https://doi.org/10.1002/14651858.CD004454.pub3
Subramaniam P, Ho JJ, Davis PG. Prophylactic nasal continuous positive airway pressure for preventing morbidity and mortality in very preterm infants. Cochrane Neonatal Group, editor. Cochrane Database Syst Rev [Internet]. 2016 [cited 2018 May 25]; Available from: http://doi.wiley.com/https://doi.org/10.1002/14651858.CD001243.pub3
Sweet DG, Carnielli V, Greisen G, Hallman M, Ozek E, Plavka R, et al. European consensus guidelines on the Management of Respiratory Distress Syndrome - 2016 update. Neonatology. 2017;111:107–25.
American Academy of Pediatrics. Committe on Fetus and Newborn. Respiratory support in preterm infants at birth. Pediatrics. 2014;133:171–4.
Bahadue FL, Soll R. Early versus delayed selective surfactant treatment for neonatal respiratory distress syndrome. Cochrane Database Syst Rev. 2012 Nov 14;11:CD001456. https://doi.org/10.1002/14651858.CD001456.pub2.
De Luca D, van Kaam AH, Tingay DG, Courtney SE, Danhaive O, Carnielli VP, et al. The Montreux definition of neonatal ARDS: biological and clinical background behind the description of a new entity. Lancet Respir Med. 2017;5:657–66.
Khemani RG, Smith LS, Zimmerman JJ, Erickson S. Pediatric acute respiratory distress syndrome: definition, incidence, and epidemiology. Pediatr Crit Care Med. 2015;16:S23–40.
Dietl P, Haller T. Exocytosis of lung surfactant: from the secretory vesicle to the air-liquid Interface. Annu Rev Physiol. 2005;67:595–621.
Dubin SB. Characterization of amniotic fluid lamellar bodies by resistive-pulse counting: relationship to measures of fetal lung maturity. Clin Chem. 1989;35:612–6.
Danhaive O, Chapin C, Horneman H, Cogo PE, Ballard PL. Surface film formation in vitro by infant and therapeutic surfactants: role of surfactant protein B. Pediatr Res. 2015;77:340–6.
Autilio C, Echaide M, Benachi A, Marfaing-Koka A, Capoluongo ED, Pérez-Gil J, et al. A noninvasive surfactant adsorption test predicting the need for surfactant therapy in preterm infants treated with continuous positive airway pressure. J Pediatr. 2017;182:66–73.e1.
Brat R, Yousef N, Klifa R, Reynaud S, Shankar Aguilera S, De Luca D. Lung ultrasonography score to evaluate oxygenation and surfactant need in neonates treated with continuous positive airway pressure. JAMA Pediatr. 2015;169:e151797.
Neerhof MG, Dohnal JC, Ashwood ER, Lee IS, Anceschi MM. Lamellar body counts: a consensus on protocol. Obstet Gynecol. 2001;97:318–20.
Besnard AE, Wirjosoekarto SAM, Broeze KA, Opmeer BC, Mol BWJ. Lecithin/sphingomyelin ratio and lamellar body count for fetal lung maturity: a meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2013;169:177–83.
Wijnberger LDE, de Kleine M, Voorbij HAM, Arabin B, Engel H, Bruinse HW, et al. Comparison of vaginal and transabdominal collection of amniotic fluid for fetal lung maturity tests. J Matern Fetal Neonatal Med. 2010;23:613–6.
Machado LU, Fiori HH, Baldisserotto M, Ramos Garcia PC, Vieira ACG, Fiori RM. Surfactant deficiency in transient tachypnea of the newborn. J Pediatr. 2011;159:750–4.
Verder H, Ebbesen F, Brandt J, Dahl M, Esberg G, Eschen C, et al. Lamellar body counts on gastric aspirates for prediction of respiratory distress syndrome. Acta Paediatr Oslo Nor 1992. 2011;100:175–80.
Raimondi F, Yousef N, Migliaro F, Capasso L, De Luca D. Point-of-care lung ultrasound in neonatology: classification into descriptive and functional applications. Pediatr Res. 2018. https://doi.org/10.1038/s41390-018-0114-9. [Epub ahead of print].
Arthur R. The neonatal chest X-ray. Paediatr Respir Rev. 2001;2:311–23.
Goldstein B, Giroir B, Randolph A. International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics*. Pediatr Crit Care Med. 2005;6:2–8.
Piastra M, Yousef N, Brat R, Manzoni P, Mokhtari M, De Luca D. Lung ultrasound findings in meconium aspiration syndrome. Early Hum Dev. 2014;90:S41–3.
Celik IH, Demirel G, Canpolat FE, Erdeve O, Dilmen U. Surfactant therapy for maternal blood aspiration: an unusual cause of neonatal respiratory distress syndrome. Indian J Pediatr. 2012;79:1358–9.
Ren X-L, Fu W, Liu J, Liu Y, **a R-M. Lung ultrasonography to diagnose pulmonary hemorrhage of the newborn. J Matern-Fetal Neonatal Med. 2017;30:2601–6.
Fenton TR. A new growth chart for preterm babies: Babson and Benda’s chart updated with recent data and a new format. BMC Pediatr. 2003;3:13.
Been JV, Vanterpool SF, de Rooij JDE, Rours GIJG, Kornelisse RF, van Dongen MCJM, et al. A clinical prediction rule for histological Chorioamnionitis in preterm newborns. Baud O, editor. PLoS One 2012;7:e46217.
Zecca E, De Luca D, Marras M, Caruso A, Bernardini T, Romagnoli C. Intrahepatic cholestasis of pregnancy and neonatal respiratory distress syndrome. Pediatrics 2006;117:1669–72.
Hadar E, Hod M. Establishing consensus criteria for the diagnosis of diabetes in pregnancy following the HAPO study. Ann N Y Acad Sci. 2010;1205:88–93.
Preventive Services Task Force US, Bibbins-Domingo K, Grossman DC, Curry SJ, Barry MJ, Davidson KW, et al. Screening for preeclampsia: US Preventive Services Task Force recommendation statement. JAMA. 2017;317:1661–7.
Perlman JM, Wyllie J, Kattwinkel J, Wyckoff MH, Aziz K, Guinsburg R, et al. Part 7: neonatal resuscitation: 2015 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations (reprint). Pediatrics. 2015;136:S120–66.
Pandit PB, Courtney SE, Pyon KH, Saslow JG, Habib RH. Work of breathing during constant- and variable-flow nasal continuous positive airway pressure in preterm neonates. Pediatrics. 2001;108:682–5.
Gizzi C, Klifa R, Pattumelli M, Massenzi L, Taveira M, Shankar-Aguilera S, et al. Continuous positive airway pressure and the burden of Care for Transient Tachypnea of the neonate: retrospective cohort study. Am J Perinatol. 2015;32:939–43.
Dell’Orto V, Bourgeois-Nicolaos N, Rouard C, Romain O, Shankar-Aguilera S, Doucet-Populaire F, et al. Cell count analysis from Nonbronchoscopic Bronchoalveolar lavage in preterm infants. J Pediatr. 2018;200:30-37.e2. https://doi.org/10.1016/j.jpeds.2018.04.074.
Tsuda H, Hirakawa A, Kotani T, Sumigama S, Mano Y, Nakano T, et al. Risk assessment for neonatal RDS/TTN using gestational age and the amniotic lamellar body count in twin pregnancies. Clin Chim Acta. 2015;451:301–4.
Cavicchioli P, Zimmermann LJ, Cogo PE, Badon T, Giordano G, Torresin M, et al. Endogenous surfactant turnover in preterm infants with respiratory distress syndrome studied with stable isotope lipids. Am J Respir Crit Care Med. 2001;163:55–60.
Jobe A, Jacobs H, Ikegami M. Lack of correlation of severity of lung disease with the phosphatidylcholine concentration in fetal lung fluid from premature lambs at 133-136 days gestational age. J Dev Physiol. 1984;6:417–21.
Jobe AH, Ikegami M, Jacobs HC, Jones SJ. Surfactant pool sizes and severity of respiratory distress syndrome in prematurely delivered lambs. Am Rev Respir Dis. 1983;127:751–5.
Wiingreen R, Greisen G, Ebbesen F, Petersen JP, Zachariassen G, Henriksen TB, et al. Surfactant need by gestation for very preterm babies initiated on early nasal CPAP: a Danish observational multicentre study of 6,628 infants born 2000-2013. Neonatology. 2017;111:331–6.
De Martino L, Yousef N, Ben-Ammar R, Raimondi F, Shankar-Aguilera S, De Luca D. Lung ultrasound score predicts surfactant need in extremely preterm neonates. Pediatrics. 2018;142(3). pii: e20180463. https://doi.org/10.1542/peds.2018-0463.
Makri V, Hospes B, Stoll-Becker S, Borkhardt A, Gortner L. Polymorphisms of surfactant protein B encoding gene: modifiers of the course of neonatal respiratory distress syndrome? Eur J Pediatr. 2002;161:604–8.
De Luca D, Harrison DA, Peters MJ. ‘Lum** or splitting’ in paediatric acute respiratory distress syndrome (PARDS). Intensive Care Med. 2018;44:1548–50.
Bhatia R, Morley CJ, Argus B, Tingay DG, Donath S, Davis PG. The stable microbubble test for determining continuous positive airway pressure (CPAP) success in very preterm infants receiving nasal CPAP from birth. Neonatology. 2013;104:188–93.
Acknowledgments
Not applicable
Funding
None
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
RR and RC, prepared the databases and collected all the data, coordinated the sample transfer, drafted the initial manuscript, they contributed equally to and reviewed and revised the manuscript. EL, AB and AMK designed the data and sample collection procedures, analysed samples and reviewed and revised the manuscript. DDL conceptualized and designed the study, coordinated and supervised it, performed the statistical analysis, and critically reviewed the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study is a part of a project on surfactant and respiratory support in neonates approved by the Ethical Committee at the South Paris University Hospital (n.CPP13–046) and consent to participation was obtained from parents or guardian upon NICU admission.
Consent for publication
Not applicable
Competing interests
DDL has received grants for research and educational projects from Chiesi Pharmaceuticals spa and ABBVIE inc. He also received travel grants from ABBVIE inc. He served as consultant and lecturer for both Chiesi Pharmaceuticals spa and ABBVIE inc. Finally, he has been the Chair of the external advisory board for Chiesi Pharmaceuticals spa and a member of the ABBVIE inc. These companies produce two surfactants, but they had no role in design, preparation, review, approval of the manuscript or decision to submit it for publication. The other authors have no conflicts of interest to disclose.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Raschetti, R., Centorrino, R., Letamendia, E. et al. Estimation of early life endogenous surfactant pool and CPAP failure in preterm neonates with RDS. Respir Res 20, 75 (2019). https://doi.org/10.1186/s12931-019-1040-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12931-019-1040-z