
Abstract
Background
To test the null hypothesis that there is no difference in the apical root resorption seen after orthodontic treatment with the conventional brackets and the self-ligating brackets.
Methods
Pre-treatment and post-treatment periapical radio-graphs of 70 patients, (35 treated with the Damon3 0.022” bracket and 35 with the 0.022” 3 M bracket) were studied. The long cone paralleling technique was used for all the radio-graphs. Any image distortion between the pre-treatment and post-treatment radio-graph was calculated and compensated for by using the crown length measurements, on the assumption that the crown length remains unaltered during the treatment period. Quantitative measurements of crown and root lengths for the maxillary and the mandibular central and lateral incisors were compared. Means and standard deviations for the percentage root resorption per tooth group were calculated. A paired t-test and non paired t-test analysis was performed to determine whether there was an appliance, treatment time, or initial age effect on the amount of root resorption seen after treatment.
Result
No statistically significant difference in root resorption between the two appliance systems was found. The patient’s degree of root resorption were graded as grade 1 and grade 2 in the self-ligating group which is more than the conventional group.
Conclusions
There was no significant difference in root resorption between self-ligating brackets and conventional brackets in severe crowding incisors subjects.
Similar content being viewed by others


Background
External apical root resorption during orthodontic treatment, referred to as ‘surface root resorption’ by Andreasen [1], is considered an unwanted consequence of orthodontic treatment that can cause biological changes in the cementum and periodontal ligament, resulting in root resorption [2, 3]. The teeth more susceptible to EARR are the maxillary and mandibular incisors, and especially the maxillary lateral incisors [4–7].
External apical root resorption (EARR) presents with a multi-factorial etiology, individual predisposition being one of the factors [8–10]. Since the greatest cause of root resorption in the population refers to orthodontic movement, a correlation exists between severity of the malocclusion and the degree of consequent root resorption [9–11]. This occurs as a result of the mechanical resources demanded and is due to long-lasting treatment [5]. In addition, characteristics that are inherent to orthodontic treatment, such as type of brackets, the mechanics used, and the type and magnitude of the forces applied [9, 10, 12], are also relevant.
Few studies have dealt with the effects of mechano-therapy on EARR. Standard edgewise, straight-wire, and Begg appliances, as well as various mechano-therapeutic approaches have been investigated [13–17]. The contributing role of continuous tooth movement across various paths, an undesirable effect known as “tooth jiggling,” and the application of inter-maxillary elastics in the development of EARR have been highlighted [18]. An interesting recent study also indicated that more EARR occurred with nickel-titanium wires and with stainless steel arch-wires [19].
The introduction of self-ligating brackets provoked the investigation of arch-wire ligation on EARR. One of the first reports on the subject was by Blake et al. [20], who tested the hypothesis that an active self-ligating bracket with an active clip might induce more EARR; their findings, however, did not confirm that hypothesis. The introduction of passive self-ligating systems, with no active spring and alignment performed by wires engaged in a passive tube, with more play, jiggling, and less friction, raises again the question of their effect on EARR. In the orthodontic literature, few studies have explored the effect on EARR of passive self-ligating systems.
Therefore, the hypothesis we tested was that the differences in the mode of wire ligation between conventional and passive self-ligating brackets affect the rate of root resorption. Our purpose was to compare the extent of root resorption of the maxillary and mandibular incisors in severe anterior crowding class I patients between self-ligating and conventional pre-adjusted brackets.
Methods
This study was designed as a longitudinal retrospective study. The study was approved by the Ethics Committee of Wenzhou medical college (182/April 2012). Inclusion criteria were: patients presented Angle Class I malocclusion, with anterior crowding more than 6 mm. Only patients that had undergone four premolar extractions were selected. Exclusion criteria were: subjects with root resorption, Class II elastics, endodontic treatment, a history of trauma impacted canines, previous orthodontic treatment or with signs of EARR observed at the first examination, or dental anomalies of a number of teeth before treatment were excluded. Those with incomplete orthodontic records and poor quality radio-graphs were also not included.
Based on a retrospective power analysis, a total of 66 patients were required to demonstrate a clinically meaningful difference of 0.85 mm in root resorption between the appliance systems with 0.05 significance level and a power of 80 %.
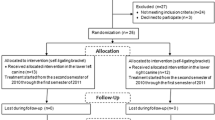
For this retrospective study, 359 participants were screened in the Department of orthodontic, hospital of stomatology, Wenzhou Medical University. 289 participants were excluded because they did not meet the inclusion criteria. At last, 70 patients were enrolled in this study, for further details see Fig. 1. They were divided into two groups: Group I (n = 35; 18 female and 17 male subjects using passive self-ligating brackets with a 0.022 × 0.028 in. slot (Damon 3, OMRCO, USA) and Group II (n = 35; 19 female and 16 male subjects using conventional pre-adjusted brackets with a 0.022 × 0.028 in. slot (3 M Unitek, California, USA).

Flow diagram of participants through each stage of the trial
Orthodontic mechanics was used a wire sequence characterized by an initial 0.012 in. nitinol or a 0.014 in. nitinol, followed by 0.016, 0.018, 0.019 × 0.025 in. nitinol, and 0.019 × 0.025 in. stainless steel arch-wires (3 M Unitek, California, USA). Slide mechanics to closed space. Trans-palatal arch or nance arch were used to enhance anchorage.
Standardized periapical radio-graphs were obtained by a single operator with the long-cone paralleling technique (SIEMENS, SIDEXIS XG, Germany) . The radio-graphs were developed with SIDEXIS automatic dental film processor . The measures were performed to the nearest 0.01 mm, using the image analysis system (SIEMENS, SIDEXIS XG, Germany). Lengths of the maxillary and mandibular incisors were measured on intra-oral periapical films before and after active treatment. Root length was measured from the CEJ to the apex. All measurements were obtained by perpendicularly projecting these points on the long axis of the tooth, which followed as accurately as possible the root canal. The most distinct CEJ landmark, either mesial or distal, was used, but once decided, the same side was used both for the pre- and post-treatment radio-graphs.
Any image distortion between the pre-treatment and post-treatment radio-graphic exposures was calculated using the crown length registrations. This method was described by Linge and Linge [4]. A correction factor was calculated to relate the pre-treatment and post-treatment radio-graphs.
Where: C1 = Crown length on pre-treatment radio-graph.
C2 = Crown length on post-treatment radio-graph.
The apical root resorption per tooth was calculated as follow:
Where: R 1 = Root length before treatment.
R 2 = Root length after treatment.
It was decided to express the root resorption seen as the percentage shortening per tooth. This percent value is a better comparative value since the differences in the root lengths of various teeth, make comparisons of root resorption values in millimeters more difficult.
Root resorption evaluation was blindly performed by one author on the final periapical radio-graphs and initial radio-graphs. The method of Malmgren [21] was used to evaluate the severity of apical root resorption, ranking it into 5° (Fig. 2). Four scores, corresponding to each anterior incisor, for each patient were obtained, a total of 280 scores per group.

Scoring system
Error study
Twenty randomly selected patients, 10 from each group, had the amount of any root resorption re-evaluated and their radio-graphs were retraced and remeasured by the same examiner after one month. For root resorption evaluation, intra-examiner agreement was calculated with Kappa statistics and Dahlberg formula (casual errors).
Statistical analyses
Chi-square was used to show the distribution of the teeth among the scores of root resorption according to the method of Malmgren [22].
A paired t-test was employed to compare the degree of root resorption in each group between T1 and T2 periods, and a non-paired t-test was used for comparison between both groups. In all statistical tests, the significance level was set at 5 %. Statistical calculations were made with Statistic software SPSS1.0 (version 20.0, IBM Inc, USA).
Results
Kappa statistics showed almost perfect agreement between the first and second root resorption intra-examiner evaluation. There were no statistically significant systematic errors and the casual errors were within acceptable limits (P =0.656 and Dahlberg = 0.27).
The groups were matched regarding the initial ages, treatment time. No statistically significant difference was found in the comparison of the initial ages and treatment time between the two groups (Table 1).
A statistically significant difference occurred in all teeth in the comparison between T1 and T2 for patients of Group I (Table 2).
The same occurred for Group II, in which all of the teeth had statistically significant root resorption, (Table 3).
Although the length of root resorption in Group 1 less decrease than Group 2, there was no statistically significant difference was found in the comparison of the degree of root resorption between the two groups (Table 4).
The distribution of teeth in the groups, scored according to Malmgren et al. [22], showed that Group 1 had 67.14 % of the teeth classified with scores of 0 and 1 and the remaining 32.86 % had root resorption scores of 2, 3, and 4. Group 2 had 55.71 % of the teeth with scores of 0 and 1 and 44.29 % with scores of 2, 3, and 4 (Table 5).
Discussion
Apical root resorption is a frequent undesirable side effect in orthodontic treatment. However, innovations in techniques and orthodontic materials have been developed to reduce this problem [22]. Because self-ligating brackets have the advantage of having less friction, we wanted to test the hypothesis that an association exists between self-ligating and conventional pre-adjusted brackets in amount of resorption.
Periapical radio-graphs were used to assess OIRR in the present study. This technique is in kee** with previous studies [7, 23]. It is accepted that periapical views may be insensitive to very minor changes in root lengths and may be less accurate than CBCT in studying the severity of OIRR. However,owing to the higher radiation dose applied, especially to children and adolescents when using cone beam computed tomography (CBCT) imaging, this technique requires a clear indication and benefit for the patient strictly adhering to ALARA (as low as reasonably achievable) principles in medicine [24]. It is, therefore, reasonable to infer that the use of repeated periapical films resulted in a valid assessment of incisor length in the present investigation.
Subjective methods, such as that of Malmgren et al. [21], are predominantly used in root resorption studies performed after tooth movement, presenting a primary advantage. Therefore, the subjective method used in the present seems to be reliable, showing almost perfect intra-examiner agreement and confirming the precision of the evaluation. Additionally, there were no significant systematic errors and the casual errors were within acceptable levels.
Factors related to orthodontic treatment are primarily responsible for the prevalence of root resorption [20, 25–26]. However, studies differ significantly regarding design, methodology, control group, and treatment characteristics. A small sample size is common problems that can lead to questionable results [27]. Such as Vanessa Leite [28] find that EARR has occurred in all teeth evaluated, the bracket design (self-ligating or conventional) did not demonstrate any influence on the results observed. Nevertheless, the sample only includes 19. Additionally, several studies do not distinguish the variables related to patients and treatments [26]. Although most correlated resorption with different types of techniques [20], they did not identify specific crowding. In this retrospective study, root resorption was investigated in a homogeneous sample, treated with self-ligating and conventional pre-adjusted brackets in severe anterior crowding of Class I patients.
Regarding the amount of root resorption, an average of 0.3 mm in self-ligating group and an average of 0.35 mm in conventional bracket group were found—a value close to that in the literature of 0.25 mm [21]. Although it occurred in all teeth, this degree of EARR is small and clinically irrelevant [29].
The main explanation may be due to treatment duration and light forces. Treatment duration had a positive association with the amount of EARR and has been attributed to persistent bone turnover associated with extended tooth movement. In this study, the mean treatment times were similar between the groups, it is reasonable to assume that the factors affecting treatment duration were similar and did not contribute to the difference in root resorption.
Therefore the contributory factor is not only treatment duration, but also another factor that may explain the smaller resorptions in this study to be the use of self-ligating brackets, which offer less force in relation to level displacement of teeth, thus affecting the magnitude of the EARR. Light forces have long been recommended to reduce adverse tissue reactions (root resorption) [30, 31].
Concerning the type of appliance, no statistically significant difference was found in the root resorption between conventional and Damon 3 bracket, although a trend indicating more EARR for conventional bracket was evident, but it did not reach significance. However, in the general bio-medical literature, significance levels slightly higher than the self-ligating brackets might receive critical importance depending on the severity of the health hazard imposed on the sample [32–34]. Thus, although our results should not give rise to statements on the relative capacity of specific appliance type to cause resorption, more research is needed before a definitive conclusion can be drawn on this subject.
In a relevant study comparing conventional and self-ligating brackets, no difference was found in the amount of root resorption [20]. These data are in accordance with the results of this research in which no statistically significant differences were detected between the two groups. Other studies reported the same findings [35, 36]. This implies that, although the Damon 3 bracket delivers a constant light force, this force is not of sufficient magnitude to decrease the root resorption observed after orthodontic treatment.
The results of the present study have to be interpreted with caution because of its limitations. First, this study was designed as a longitudinal retrospective study. Generally speaking, it is very difficult to avoid confounding factors. But, we can reduce the effects of bias by making strict inclusion criteria. The baseline levels of two groups are in consistency. And malocclusion type might affect the results, therefore, in this study only patients with Angle Class I were included so as to minimize the impact of confounding factors on the experimental results. Another problem related to longitudinal retrospective studies might be the information bias. We have gone through repeated trials, and surveyors and final statistics do not know the group of data. Therefore, this study is relatively real, which may reflect the actual results accurately. Second, our investigation was only assessed EARR on the incisors. Although these teeth show a higher prevalence of EARR, conclusions on EARR involvement in orthodontic tooth movement with different appliances would require examination of the entire dentition.
According to the results of this study, self-ligating brackets induced less apical root shortening measured in periapical radio-graphs than conventional pre-adjusted brackets. However, there is no statistically significant difference was found in the comparison of the degree of root resorption between the two groups. Because of self-ligatingbrackets are more expensive than conventional pre-adjusted brackets and Other advantages of this system are fewer appointments, such as improved oral hygiene, better acceptance by patients, and better treatment results, therefore choose types of brackets still depend on orthodontics experience and patients.
Conclusion
-
There are no significant differences in the amount of apical root resorption between passive self-ligating and conventional preadjusted in severe anterior crowding Class I patients.
References
Andreasen J. Review of root resorption systems and models. Etiology of root resorption and the homeostatic mechanisms of the periodontal ligament. In: Davidovitch Z, editor. Biological mechanisms of tooth eruption and root resorption. Philadelphia: W B Saunders; 1988. p. 9–22.
Brezniak N, Wasserstein A. Root resorption after orthodontic treatment: Part 1. Literature review. Am J Orthod Dentofacial Orthop. 1993;103:62–6.
Faltin RM, Faltin K, Sander FG, Arana-Chavez VE. Ultra-structure of cementum and periodontal ligament after continuous intrusion in humans: a transmission electron microscopy study. Eur J Orthod. 2001;23:35–49.
Linge BO, Linge L. Apical root resorption in upper and anterior teeth. Eur J Orthod. 1983;5:173–83.
Linge L, Linge BO. Patient characteristics and treatment variables associated with apical root resorption during orthodontic treatment. Am J Orthod Dentofacial Orthop. 1991;99:35–43.
Mirabella AD, Årtun J. Prevalence and severity of apical root resorption in upper anterior teeth in adult orthodontic patients. Eur J Orthod. 1995;17:93–9.
Sameshima GT, Sinclair PM. Predicting and preventing root resorption: part I. Diagnostic factors. Am J Orthod Dentofacial Orthop. 2001;119:505–10.
Weltman B. Root resorption associated with orthodontic tooth movement: a systematic review. Am J Orthod Dentofacial Orthop. 2010;137:462–76.
Levander E, Malmgren O. Evaluation of the risks of root resorption during orthodontic treatment: a study of upper incisors. Eur J Orthod. 1988;10:30–8.
Mirabella D, Artun J. Risk factors for apical root resorption of maxillary anterior teeth in adult orthodontic patients. Am J Orthod Dentofacial Orthop. 1995;108:48–55.
Hartsfield Jr JK, Everett ET, Al-Qawasmi RA. Genetic factors in external apical root resorption and orthodontic treatment. Crit Rev Oral Biol Med. 2004;15:115–22.
Artun J, Smale I, Behbehani F, Doppel D, Van’t Hof M, Kuijpers-Jagtman AM. Apical root resorption six and 12 months after initiation of fixed orthodontic appliance therapy. Angle Orthod. 2005;29:919–26.
Janson GR, De Luca CG, Martins DR, Henriques JF, De Freitas MR. A radiographic comparison of apical root resorption after orthodontic treatment with 3 different fixed appliance techniques. Am J Orthod Dentofacial Orthop. 1999;118:262–73.
Alexander SA. Levels of root resorption associated with continuous arch and sectional arch mechanics. Am J Orthod Dentofacial Orthop. 1996;110:321–4.
Mavragani M, Vergari A, Selliseth NJ, Boe OE, Wisth PJ. A radiographic comparison of apical root resorption after orthodontic treatment with a standard edgewise and a straight-wire edgewise technique. Eur J Orthod. 2000;22:665–74.
Mullenhauer B. Towards paradigmless orthodontics. Am J Orthod Dentofacial Orthop. 1987;92:437–44.
Beck BW, Harris EF. Apical root resorption in orthodontically treated subjects: analysis of edgewise and light wire mechanics. Am J Orthod Dentofacial Orthop. 1994;105:350–61.
Linge L. Apical root resorption induced by orthodontic treatment. Clinical manifestations and etiologic considerations. In: Davidovitch Z, editor. The biological mechanisms of tooth eruption, resorption and replacement by implants. Birmingham, Ala: EBSCO Media; 1988. p. 527–35.
Weiland F. Constant versus dissipating forces in orthodontics: the effect on initial tooth movement and root resorption. Eur J Orthod. 2003;25:335–42.
Blake M, Woodside DJ, Pharoah MJ. A radiographic comparison of apical root resorption after orthodontic treatment with the edgewise and speed appliances. Am J Orthod Dentofacial Orthop. 1995;108:76–84.
Malmgren O, Goldson L, Hill C, Orwin A, Petrini L, Lundberg M. Root resorption after orthodontic treatment of traumatized teeth. Am J Orthod Dentofacial Orthop. 1982;82:487–91.
Janson GR, Canto GL, Martins DR, Henriques JFC, Freitas MR. A radiographic comparison of apical root resorption after orthodontic treatment with 3 different fixed appliance techniques. Am J Orthod Dentofacial Orthop. 1999;118:262–73.
Copeland S, Green LJ. Root resorption in maxillary central incisors following active orthodontic treatment. Am J Orthod Dentofacial Orthop. 1986;89:51–5.
Claus EB, Calvocoressi L, Bondy ML, Schildkraut JM, Wiemels JL, Wrensch M. Dental x-rays and risk of meningioma. Cancer. 2012;118:4530–7.
McFadden WM, Engström C, Engström H, Anholm JM. A study of the relationship between incisor intrusion and root shortening. Am J Orthod Dentofacial Orthop. 1989;96:390–6.
Baumrind S, Korn EL, Boyd RL. Apical root resorption in orthodontically treated adults. Am J Orthod Dentofacial Orthop. 1996;110:311–20.
Martins DR, Tibola D, Janson G, Maria RT. Effects of intrusion combined with anterior retraction on apical root resorption. Eur J Orthod. 2012;34:170–5.
Leite V, Conti AC, Navarro R, Almeida M, Oltramari-Navarro P, Almeida R. Comparison of root resorption between self-ligating and conventional preadjusted brackets using cone-beam computed tomography. Angle Orthod. 2012;82:1078–82.
Smale I, Artun J, Behbehani F, Doppel D, Van’t Hof M, Kuijpers-Jagtman AM. Apical root resorption 6 months after initiation of fixed orthodontic appliance therapy. Am J Orthod Dentofacial Orthop. 2005;128:57–67.
Reitan K. Initial tissue behavior during apical root resorption. Angle Orthod. 1974;44:68–82.
King GJ, Fischlschweiger W. The effect of force magnitude on extractable bone resorption activity and cementum cratering in orthodontic tooth movement. J Dent Res. 1982;61:773–9.
Walker AM. Reporting the results of epidemiologic studies. Am J Public Health. 1986;76:556–8.
Anscombe FJ. The summarizing of clinical experiments by significance levels. Stat Med. 1990;9:703–8.
Cohen J. The earth is round (p 0.05). Am Psychol. 1994;47:997–1003.
Scott P, Di Biase AT, Sherriff M, Cobourne M. Alignment efficiency of Damon 3 self-ligating and conventional orthodontic bracket systems: a randomized clinical trial. Am J Orthod Dentofacial Orthop. 2008;134:470.e1–8.
Pandis N. External apical root resorption in patients treated with conventional and self-ligating brackets. Am J Orthod Dentofacial Orthop. 2008;134:646–51.
Acknowledgement
We thank Prof.Song Kanming who revising it critically for important intellectual content.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
WC and YZ designed the study, gathered the information, performed the statistical analysis and wrote the first draft of the manuscript. AH check the language. All authors read and approved the final manuscript.
Authors' information
Not applicable.
Availability of data and materials
Not applicable.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Chen, W., Haq, A.A.A. & Zhou, Y. Root resorption of self-ligating and conventional preadjusted brackets in severe anterior crowding Class I patients: a longitudinal retrospective study. BMC Oral Health 15, 115 (2015). https://doi.org/10.1186/s12903-015-0100-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-015-0100-0