
Abstract
Background
Recent advances in telecommunications technology have raised the possibility of telehealth intervention delivering cardiac telerehabilitation, which may provide the efficacy of health services in patients after percutaneous coronary intervention (PCI). This study aimed to investigate the effects of home-based cardiac telerehabilitation (HBCTR) in patients undergoing PCI.
Methods
We performed a comprehensive search of the following electronic databases: PubMed, Cochrane Central, Web of Science, Embase, CNKI, and WANFANG. For the prespecified outcomes, the primary outcomes were results of physical function (the six-minute walking test, 6MWT) and quality of life (QoL) of the participants. The secondary outcomes were results of (1) blood pressure; (2) full lipid profile (3) reliable assessment of anxiety and depression in patients.
Results
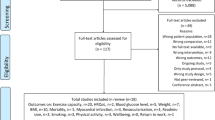
All studies were conducted between 2013 and 2022, and a total of 5 articles could be included in the quantitative meta-analysis. The results showed that there was a statistically significant difference between the HBCTR intervention group and the control group in 6WMT (MD 16.59, 95%CI 7.13 to 26.06, P = 0.0006), but there was no difference in QoL (SMD − 0.25, 95%CI − 1.63 to 1.13, P = 0.73). According to the fixed effects model, there was a statistically significant difference between the HBCTR group versus the control group (MD − 2.88, 95%CI − 5.19 to − 0.57, P = 0.01), but not in diastolic blood pressure. Likewise, significant improvements of triglycerides and in low-density lipoprotein cholesterol were observed in HBTCR groups, but no significant differences were observed regarding total cholesterol and high-density lipoprotein cholesterol.
Conclusion
This systematic review and meta-analysis have proven that the HBCTR is one of the promisingly effective cardiac rehabilitation strategies that improve cardiorespiratory fitness and reduce cardiovascular disease risk factors. With the continuous improvement of the telerehabilitation network, it is expected to serve in clinical.
Similar content being viewed by others


Introduction
Cardiovascular disease is the most predominant cause of death globally, with about estimated over 17 million people who died of cardiovascular disease in 2016, representing 31% of all deaths worldwide [1], among which coronary artery disease (CAD) remains one of the top killers [2]. CAD refers to the condition of vascular lumen stenosis or occlusion and vascular spasm based on coronary artery atherosclerosis, leading to myocardial ischemia, hypoxia, or necrosis [3]. CAD has become one of the causes of high morbidity and mortality and the leading cause of severe long-term disability in developed and some develo** countries.
Percutaneous coronary intervention (PCI) is the primary way to obtain revascularization in patients with CAD [4] due to advances in PCI technology and technique [5]. After PCI, knowledge of cardiac rehabilitation (CR) and timely management of complications [6] are essential health services for patients, associated with decreasing the rate of vascular restenosis and recurrent ischemia, to improve quality of life [7]. As such, CR was recommended for secondary prevention, established by the American Heart Association and American College of Cardiology after PCI [4]. CR is a complete, full-cycle, and effective medical management strategy. However, the development of CR also faces many opportunities and challenges, such as the continuity of CR throughout the life cycle of patients [8, 9]. In the in-hospital rehabilitation period, the care team supervises the patient's daily life and motor ability to recover. But many patients do not transition to outpatient CR centers and receive recommended prescriptions in time after discharge [10]. Therefore, there are still gaps in this continuous medical behavior, which may eventually lead to unsatisfactory treatment effects and prognosis for patients. Despite the obvious evidence-based benefits, the participation rate of CR remains poor [11]. The reasons why people have low adherence to the traditional facility-based CR are multi-faceted [12], such as private insurance, the travel distance to a healthcare site and possibly affiliated CR facility, demographic and clinical factors, and existing comorbidity [13]. Therefore, it is reported that the center-based CR programs were challenged by low participant rates, insufficient attendance, and high drop-out rates. As a result, there is an urgent need for effective strategies to increase patient engagement, and home-based cardiac rehabilitation (HBCR) is one of the most potent strategies [14]. It also confirmed that the benefits of HBCR in terms of exercise capacity, control of risk factors, quality of life, and cost-effectiveness is similar to center-based CR [15, 16].But how to adequately assess the patient's situation and get timely feedback is also a major issue.
Recent advances in telecommunications technology have raised the possibility of telehealth interventions delivered by CR, which is able to overcome barriers of time and distance [17], and increase the rate of utilization mainly due to avoidance of expensive medical costs [18]. Therefore, we pay attention to the fact that home-based cardiac telerehabilitation (HBCTR) for patients in the home environment can link doctors and patients, better continue in-hospital rehabilitation, and also provide rehabilitation guarantee for out-hospital rehabilitation. Previous research has shown that the sooner CR begins in patients with CAD, the greater the benefit for patients [19]. CR for patients with CAD is divided into three stages, including stage I (in-hospital rehabilitation), stage II (out-of-hospital early rehabilitation or outpatient rehabilitation), and stage III (long-term community/family rehabilitation) [20]. Each stage of rehabilitation should follow the principle of safety. Therefore, most patients eligible for HBCTR are at low to intermediate risk, or in the transition from acute to convalescent phase and convalescent phase [14]. Telehealth can be defined as providing health management through emerging mobile devices such as mobile computing, medical sensor, and communications technologies [21]. The use of telehealth has grown tremendously and covers a wide range of content, such as digital information collection, precision medicine, virtual diagnosis, and treatment. Compared to other telehealth interventions, HBCTR focuses on the rehabilitation and prognosis of heart disease patients, and the core components of management include exercise training, risk factor control, psychological counseling, drug guidance, and nutritional prescription [22, 23]. The based model established by HBCTR is: the doctors formulate the CR prescription and send it remotely, and the patients execute the prescription, report data and conduct follow-up feedback, after that doctors make the personalized modification of the rehabilitation prescription in the standardized medical behavior. The closed-loop mechanism improves the patient's self-efficacy and enhances cardiac rehabilitation compliance. Meanwhile, HBCTR appears to be a more feasible and effective innovative rehabilitation model than conventional in-hospital CR [24]. Moreover, Stefanakis et al. showed patients received HBCTR with a low rate of adverse events after being fully evaluated before receiving the intervention [25].
It has been reported that telerehabilitation has proved beneficial effect for many patients, such as stroke survivors [26], patients with knee osteoarthritis [67], a heart rate monitor with a chest strap and a web application uploaded recorded heart rate data via the Internet were used to guide the exercise process of home telerehabilitation. However, the results showed that there was no significant difference in physical fitness between home exercise training and central exercise training guided by remote monitoring. And our systematic review has some new strengths. We investigated the participants who were restricted after PCI. Post-PCI patients urgently need self-management to improve clinical outcomes, such as reducing depression and anxiety, reducing mortality and morbidity, and improving health-related quality of life (HRQoL) [68]. Compared with a former systematic review, exercise training is a core component in previous studies, but we performed this including some multidisciplinary interventions and multifaceted care, such as physical exercise, nutritional advice, and target-driven pharmacological therapies.
Limitations
There are some limitations to this study. The first limitation is the great variability and complexity of intervention models, such as different frequency and intensity forms. Moreover, the included studies used various models of telerehabilitation (different duration, frequency, length, and intensity). For example, there were a wide of telehealth intervention models, such as smartphone-based CR platforms, remote monitoring systems, wireless monitoring, and sports band with a smartphone. Therefore, future research needs to explore which model is best for these patients. Second, some results could not be quantitatively analyzed due to the relatively small sample size of the included studies. Third, we only focused on treatment efficacy and need to pay attention to operability and cost of services, which should be included in future studies. Therefore, more extensive randomized controlled trials are required in order to confirm the current evidence.
Conclusions
This systematic review and meta-analysis have proved that HBCTR can effectively improve patients' physical function after PCI. These results justify that the home-based telehealth intervention is one of the promisingly effective CR strategies that reduce cardiovascular disease risk factors. In order to further confirm HBCTR increasing uptake and make CR available, the sample size needs to be increased, and future research needs to explore which model is best for these patients.
Availability of data and materials
All data generated or analysed during this study are included in this published article.
Abbreviations
- CAD:
-
Coronary artery disease
- PCI:
-
Percutaneous coronary intervention
- CR:
-
Cardiac rehabilitation
- HBCR:
-
Home-based cardiac rehabilitation
- HBCTR:
-
Home-based cardiac telerehabilitation
- 6MWT:
-
The six-minute walking test
- QoL:
-
Quality of life
- TC:
-
Total cholesterol
- TGs:
-
Triglycerides
- LDL-C:
-
Low-density lipoprotein cholesterol
- HDL-C:
-
High-density lipoprotein cholesterol
- RCTs:
-
Relevant randomized controlled trials
- VO2 peak:
-
Peak oxygen consumption
- CPET:
-
Cardiopulmonary exercise test
References
Kang EH, Park EH, Shin A, Song JS, Kim SC. Cardiovascular risk associated with allopurinol vs. benzbromarone in patients with gout. Eur Heart J. 2021;42(44):4578–88.
Christensen RH, Wedell-Neergaard AS, Lehrskov LL, Legaard GE, Dorph E, Larsen MK, Launbo N, Fagerlind SR, Seide SK, Nymand S, et al. Effect of aerobic and resistance exercise on cardiac adipose tissues: secondary analyses from a randomized clinical trial. JAMA Cardiol. 2019;4(8):778–87.
Choi S, Kim K, Kim SM, Lee G, Jeong SM, Park SY, Kim YY, Son JS, Yun JM, Park SM. Association of obesity or weight change with coronary heart disease among young adults in South Korea. JAMA Intern Med. 2018;178(8):1060–8.
Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, Chambers CE, Ellis SG, Guyton RA, Hollenberg SM, et al. 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention: a report of the american college of cardiology foundation/American heart association task force on practice guidelines and the society for cardiovascular angiography and interventions. Circulation. 2011;124(23):e574-651.
Bhatt DL. Percutaneous coronary intervention in 2018. JAMA. 2018;319(20):2127–8.
Giannini F, Candilio L, Mitomo S, Ruparelia N, Chieffo A, Baldetti L, Ponticelli F, Latib A, Colombo A. A practical approach to the management of complications during percutaneous coronary intervention. JACC Cardiovasc Interv. 2018;11(18):1797–810.
Anderson L, Thompson DR, Oldridge N, Zwisler AD, Rees K, Martin N. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst Rev. 2016;1:Cd001800.
Keib CN, Reynolds NR, Ahijevych KL. Poor use of cardiac rehabilitation among older adults: a self-regulatory model for tailored interventions. Heart Lung. 2010;39(6):504–11.
Thomas RJ, King M, Lui K, Oldridge N, Piña IL, Spertus J. AACVPR/ACCF/AHA 2010 update: performance measures on cardiac rehabilitation for referral to cardiac rehabilitation/secondary prevention services endorsed by the American college of chest physicians, the American college of sports medicine, the American physical therapy association, the Canadian association of cardiac rehabilitation, the clinical exercise physiology association, the European association for cardiovascular prevention and rehabilitation, the inter-American heart foundation, the national association of clinical nurse specialists, the preventive cardiovascular nurses association, and the society of thoracic surgeons. J Am Coll Cardiol. 2010;56(14):1159–67.
Thomas RJ, Balady G, Banka G, Beckie TM, Chiu J, Gokak S, Ho PM, Keteyian SJ, King M, Lui K, et al. 2018 ACC/AHA clinical performance and quality measures for cardiac rehabilitation: a report of the American college of cardiology/American heart association task force on performance measures. Circ Cardiovasc Qual Outcomes. 2018;11(4):e000037.
Peters AE, Keeley EC. Trends and predictors of participation in cardiac rehabilitation following acute myocardial infarction: data from the behavioral risk factor surveillance system. J Am Heart Assoc. 2017;7(1).
Neubeck L, Freedman SB, Briffa T, Bauman A, Redfern J. Four-year follow-up of the choice of health options in prevention of cardiovascular events randomized controlled trial. Eur J Cardiovasc Prev Rehabil. 2011;18(2):278–86.
Sukul D, Seth M, Barnes GD, Dupree JM, Syrjamaki JD, Dixon SR, Madder RD, Lee D, Gurm HS. Cardiac rehabilitation use after percutaneous coronary intervention. J Am Coll Cardiol. 2019;73(24):3148–52.
Thomas RJ, Beatty AL, Beckie TM, Brewer LC, Brown TM, Forman DE, Franklin BA, Keteyian SJ, Kitzman DW, Regensteiner JG, et al. Home-based cardiac rehabilitation: a scientific statement from the American association of cardiovascular and pulmonary rehabilitation, the American heart association, and the American college of cardiology. Circulation. 2019;140(1):e69–89.
Taylor RS, Dalal H, Jolly K, Moxham T, Zawada A. Home-based versus centre-based cardiac rehabilitation. Cochrane Database Syst Rev 2010;(1):Cd007130.
Anderson L, Oldridge N, Thompson DR, Zwisler AD, Rees K, Martin N, Taylor RS. Exercise-based cardiac rehabilitation for coronary heart disease: cochrane systematic review and meta-analysis. J Am Coll Cardiol. 2016;67(1):1–12.
Clark RA, Conway A, Poulsen V, Keech W, Tirimacco R, Tideman P. Alternative models of cardiac rehabilitation: a systematic review. Eur J Prev Cardiol. 2015;22(1):35–74.
Thaker DA, Monypenny R, Olver I, Sabesan S. Cost savings from a telemedicine model of care in northern Queensland, Australia. Med J Aust. 2013;199(6):414–7.
Haykowsky M, Scott J, Esch B, Schopflocher D, Myers J, Paterson I, Warburton D, Jones L, Clark AM. A meta-analysis of the effects of exercise training on left ventricular remodeling following myocardial infarction: start early and go longer for greatest exercise benefits on remodeling. Trials. 2011;12:92.
King M, Bittner V, Josephson R, Lui K, Thomas RJ, Williams MA. Medical director responsibilities for outpatient cardiac rehabilitation/secondary prevention programs: 2012 update: a statement for health care professionals from the American Association of Cardiovascular and Pulmonary Rehabilitation and the American Heart Association. Circulation. 2012;126(21):2535–43.
Istepanian R, Jovanov E, Zhang YT. Introduction to the special section on M-Health: beyond seamless mobility and global wireless health-care connectivity. IEEE Trans Inf Technol Biomed. 2004;8(4):405–14.
Wongvibulsin S, Habeos EE, Huynh PP, Xun H, Shan R, Porosnicu Rodriguez KA, Wang J, Gandapur YK, Osuji N, Shah LM, et al. Digital health interventions for cardiac rehabilitation: systematic literature review. J Med Internet Res. 2021;23(2):e18773.
Zhang X, Luo Z, Yang M, Huang W, Yu P. Efficacy and safety of digital therapeutics-based cardiac rehabilitation in heart failure patients: a systematic review. ESC Heart Fail. 2022;9(6):3751–60.
Frederix I, Vanhees L, Dendale P, Goetschalckx K. A review of telerehabilitation for cardiac patients. J Telemed Telecare. 2015;21(1):45–53.
Stefanakis M, Batalik L, Antoniou V, Pepera G. Safety of home-based cardiac rehabilitation: a systematic review. Heart Lung. 2022;55:117–26.
Chen J, ** W, Zhang XX, Xu W, Liu XN, Ren CC. Telerehabilitation Approaches for stroke patients: systematic review and meta-analysis of randomized controlled trials. J Stroke Cerebrovasc Dis. 2015;24(12):2660–8.
**e SH, Wang Q, Wang LQ, Wang L, Song KP, He CQ. Effect of internet-based rehabilitation programs on improvement of pain and physical function in patients with knee osteoarthritis: systematic review and meta-analysis of randomized controlled trials. J Med Internet Res. 2021;23(1):e21542.
Jiang S, **ang J, Gao X, Guo K, Liu B. The comparison of telerehabilitation and face-to-face rehabilitation after total knee arthroplasty: a systematic review and meta-analysis. J Telemed Telecare. 2018;24(4):257–62.
Russell TG, Buttrum P, Wootton R, Jull GA. Internet-based outpatient telerehabilitation for patients following total knee arthroplasty: a randomized controlled trial. J Bone Joint Surg Am. 2011;93(2):113–20.
Brouwers RWM, Kraal JJ, Regis M, Spee RF, Kemps HMC. Effectiveness of cardiac telerehabilitation with relapse prevention: smartcare-CAD randomized controlled trial. J Am Coll Cardiol. 2021;77(21):2754–6.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535.
Dorje T, Zhao G, Tso K, Wang J, Chen Y, Tsokey L, Tan BK, Scheer A, Jacques A, Li Z, et al. Smartphone and social media-based cardiac rehabilitation and secondary prevention in China (SMART-CR/SP): a parallel-group, single-blind, randomised controlled trial. Lancet Digit Health. 2019;1(7):e363–74.
Fang J, Huang B, Xu D, Li J, Au WW. Innovative application of a home-based and remote sensing cardiac rehabilitation protocol in chinese patients after percutaneous coronary intervention. Telemed J E Health. 2019;25(4):288–93.
Lee YH, Hur SH, Sohn J, Lee HM, Park NH, Cho YK, Park HS, Yoon HJ, Kim H, Nam CW, et al. Impact of home-based exercise training with wireless monitoring on patients with acute coronary syndrome undergoing percutaneous coronary intervention. J Korean Med Sci. 2013;28(4):564–8.
Li Z, Hui Z, Zheng Y, Yu J, Zhang J. Efficacy of phase II remote home rehabilitation in patients with acute myocardial infarction after percutaneous coronary intervention. Contrast Media Mol Imaging. 2022;2022:4634769.
Widmer RJ, Allison TG, Lennon R, Lopez-Jimenez F, Lerman LO, Lerman A. Digital health intervention during cardiac rehabilitation: a randomized controlled trial. Am Heart J. 2017;188:65–72.
Lavie CJ, Milani RV. Cardiac rehabilitation and exercise training in secondary coronary heart disease prevention. Prog Cardiovasc Dis. 2011;53(6):397–403.
Balady GJ, Arena R, Sietsema K, Myers J, Coke L, Fletcher GF, Forman D, Franklin B, Guazzi M, Gulati M, et al. Clinician’s Guide to cardiopulmonary exercise testing in adults: a scientific statement from the American Heart Association. Circulation. 2010;122(2):191–225.
Antoniou V, Davos CH, Kapreli E, Batalik L, Panagiotakos DB, Pepera G: Effectiveness of home-based cardiac rehabilitation, using wearable sensors, as a multicomponent, cutting-edge intervention: a systematic review and meta-analysis. J Clin Med. 2022, 11(13).
Duscha BD, Piner LW, Patel MP, Craig KP, Brady M, McGarrah RW 3rd, Chen C, Kraus WE. Effects of a 12-week mHealth program on peak VO(2) and physical activity patterns after completing cardiac rehabilitation: a randomized controlled trial. Am Heart J. 2018;199:105–14.
Luo Q, Li C, Zhuang B, Li G, Luo L, Ni Y, Huang Z, Wang L, Song H, Yan W, et al. Establishment of exercise intensity for patients with chronic heart failure equivalent to anaerobic threshold based on 6-minute walking test. Ann Palliat Med. 2020;9(5):2766–75.
Forman DE, Fleg JL, Kitzman DW, Brawner CA, Swank AM, McKelvie RS, Clare RM, Ellis SJ, Dunlap ME, Bittner V. 6-min walk test provides prognostic utility comparable to cardiopulmonary exercise testing in ambulatory outpatients with systolic heart failure. J Am Coll Cardiol. 2012;60(25):2653–61.
Schopfer DW, Whooley MA, Allsup K, Pabst M, Shen H, Tarasovsky G, Duvernoy CS, Forman DE. Effects of home-based cardiac rehabilitation on time to enrollment and functional status in patients with ischemic heart disease. J Am Heart Assoc. 2020;9(19):e016456.
Ramachandran HJ, Jiang Y, Tam WWS, Yeo TJ, Wang W. Effectiveness of home-based cardiac telerehabilitation as an alternative to Phase 2 cardiac rehabilitation of coronary heart disease: a systematic review and meta-analysis. Eur J Prev Cardiol. 2022;29(7):1017–43.
Fiuza-Luces C, Santos-Lozano A, Joyner M, Carrera-Bastos P, Picazo O, Zugaza JL, Izquierdo M, Ruilope LM, Lucia A. Exercise benefits in cardiovascular disease: beyond attenuation of traditional risk factors. Nat Rev Cardiol. 2018;15(12):731–43.
Armstrong MJ, Sigal RJ, Arena R, Hauer TL, Austford LD, Aggarwal S, Stone JA, Martin BJ. Cardiac rehabilitation completion is associated with reduced mortality in patients with diabetes and coronary artery disease. Diabetologia. 2015;58(4):691–8.
Marzolini S, Blanchard C, Alter DA, Grace SL, Oh PI. Delays in referral and enrolment are associated with mitigated benefits of cardiac rehabilitation after coronary artery bypass surgery. Circ Cardiovasc Qual Outcomes. 2015;8(6):608–20.
Carney RM, Freedland KE. Depression and coronary heart disease. Nat Rev Cardiol. 2017;14(3):145–55.
Boersma E, Keil U, De Bacquer D, De Backer G, Pyörälä K, Poldermans D, Leprotti C, Pilotto L, de Swart E, Deckers JW, et al. Blood pressure is insufficiently controlled in European patients with established coronary heart disease. J Hypertens. 2003;21(10):1831–40.
Yoo JK, Fu Q. Impact of sex and age on metabolism, sympathetic activity, and hypertension. Faseb J. 2020;34(9):11337–46.
Shim CY, Ha JW, Park S, Choi EY, Choi D, Rim SJ, Chung N. Exaggerated blood pressure response to exercise is associated with augmented rise of angiotensin II during exercise. J Am Coll Cardiol. 2008;52(4):287–92.
Ikizler TA, Robinson-Cohen C, Ellis C, Headley SAE, Tuttle K, Wood RJ, Evans EE, Milch CM, Moody KA, Germain M, et al. Metabolic effects of diet and exercise in patients with moderate to severe CKD: a randomized clinical trial. J Am Soc Nephrol. 2018;29(1):250–9.
Messerli FH, Panjrath GS. The J-curve between blood pressure and coronary artery disease or essential hypertension: exactly how essential? J Am Coll Cardiol. 2009;54(20):1827–34.
Li Y, Wei FF, Thijs L, Boggia J, Asayama K, Hansen TW, Kikuya M, Björklund-Bodegård K, Ohkubo T, Jeppesen J, et al. Ambulatory hypertension subtypes and 24-hour systolic and diastolic blood pressure as distinct outcome predictors in 8341 untreated people recruited from 12 populations. Circulation. 2014;130(6):466–74.
Pfaeffli Dale L, Whittaker R, Jiang Y, Stewart R, Rolleston A, Maddison R. Text message and internet support for coronary heart disease self-management: results from the text4heart randomized controlled trial. J Med Internet Res. 2015;17(10):e237.
Dalli-Peydró E, Gisbert-Criado R, Amigó N, Sanz-Sevilla N, Cosín-Sales J. Cardiac telerehabilitation with long-term follow-up reduces GlycA and improves lipoprotein particle profile: a randomised controlled trial. Int J Cardiol. 2022;369:60–4.
Navarese EP, Robinson JG, Kowalewski M, Kolodziejczak M, Andreotti F, Bliden K, Tantry U, Kubica J, Raggi P, Gurbel PA. Association between baseline LDL-C level and total and cardiovascular mortality after LDL-C lowering: a systematic review and meta-analysis. JAMA. 2018;319(15):1566–79.
Sud M, Han L, Koh M, Abdel-Qadir H, Austin PC, Farkouh ME, Godoy LC, Lawler PR, Udell JA, Wijeysundera HC, et al. Low-density lipoprotein cholesterol and adverse cardiovascular events after percutaneous coronary intervention. J Am Coll Cardiol. 2020;76(12):1440–50.
McMahon SR, Ades PA, Thompson PD. The role of cardiac rehabilitation in patients with heart disease. Trends Cardiovasc Med. 2017;27(6):420–5.
Subedi N, Rawstorn JC, Gao L, Koorts H, Maddison R. Implementation of telerehabilitation interventions for the self-management of cardiovascular disease: systematic review. JMIR Mhealth Uhealth. 2020;8(11):e17957.
Koh KW, Wang W, Richards AM, Chan MY, Cheng KK. Effectiveness of advanced practice nurse-led telehealth on readmissions and health-related outcomes among patients with post-acute myocardial infarction: ALTRA Study Protocol. J Adv Nurs. 2016;72(6):1357–67.
Maddison R, Rawstorn JC, Stewart RAH, Benatar J, Whittaker R, Rolleston A, Jiang Y, Gao L, Moodie M, Warren I, et al. Effects and costs of real-time cardiac telerehabilitation: randomised controlled non-inferiority trial. Heart. 2019;105(2):122–9.
Su JJ, Paguio J, Baratedi WM, Abu-Odah H, Batalik L. Experience of coronary heart disease patients with a nurse-led eHealth cardiac rehabilitation: qualitative process evaluation of a randomized controlled trial. Heart Lung. 2023;57:214–21.
Neubeck L, Redfern J, Fernandez R, Briffa T, Bauman A, Freedman SB. Telehealth interventions for the secondary prevention of coronary heart disease: a systematic review. Eur J Cardiovasc Prev Rehabil. 2009;16(3):281–9.
Avila A, Claes J, Buys R, Azzawi M, Vanhees L, Cornelissen V. Home-based exercise with telemonitoring guidance in patients with coronary artery disease: Does it improve long-term physical fitness? Eur J Prev Cardiol. 2020;27(4):367–77.
Batalik L, Dosbaba F, Hartman M, Konecny V, Batalikova K, Spinar J. Long-term exercise effects after cardiac telerehabilitation in patients with coronary artery disease: 1-year follow-up results of the randomized study. Eur J Phys Rehabil Med. 2021;57(5):807–14.
Kraal JJ, Van den Akker-Van Marle ME, Abu-Hanna A, Stut W, Peek N, Kemps HM. Clinical and cost-effectiveness of home-based cardiac rehabilitation compared to conventional, centre-based cardiac rehabilitation: results of the FIT@Home study. Eur J Prev Cardiol. 2017;24(12):1260–73.
Sukul D, Seth M, Thompson MP, Keteyian SJ, Boyden TF, Syrjamaki JD, Yaser J, Likosky DS, Gurm HS. Hospital and operator variation in cardiac rehabilitation referral and participation after percutaneous coronary intervention: insights from blue cross blue shield of michigan cardiovascular consortium. Circ Cardiovasc Qual Outcomes. 2021;14(11):e008242.
Acknowledgements
No
Funding
This work was supported by National Key R&D Program of China (Grand No. 2020YFC2008500 and 2020YFC2008502) and National Natural Science Foundation of China (Grant No. 81572231 and 82172534) and 1·3·5 Project for Disciplines of Excellence, West China Hospital, Sichuan University (Grant No. ZYJC21038).
Author information
Authors and Affiliations
Contributions
Conceptualization: WZ and QW; Methodology: QW, CF and LX; Formal analysis and investigation: XS, CF and QW; Writing of original draft preparation: WZ; Writing of review and editing: QW, CF, LX, XS and SW; Funding acquisition: QW; Resources: CH; Supervision: QW. All authors read and approved the final manuscirpt.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The author(s) has/have no competing interests to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhong, W., Fu, C., Xu, L. et al. Effects of home-based cardiac telerehabilitation programs in patients undergoing percutaneous coronary intervention: a systematic review and meta-analysis. BMC Cardiovasc Disord 23, 101 (2023). https://doi.org/10.1186/s12872-023-03120-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-023-03120-2