
Abstract
Background
Spirulina maxima is a filamentous cyanobacterium used as food supplement because of its high nutrient contents. It has been experimentally proven, in vivo and in vitro that posses several pharmacological properties. The purpose of this study was to evaluate the effects of Spirulina maxima orally supplied (4.5 g/day, for 6 weeks) to a sample of 36 subjects (16 men and 20 women, with ages between 18–65 years) on serum lipids, glucose, aminotransferases and on blood pressure. The volunteers did not modify their dietary habits or lifestyle during the whole experimental period. From each subject, a sample of blood was drawn in fasting state of 12 hours to determi the plasma concentrations of glucose, triacylglycerols (TAG), total cholesterol (TC), cholesterol associated to high density lipoprotein (HDL-C) and aspartate aminotransferase (AST). Anthropometric measurements including systolic (SYST-P) and diastolic (DIAST-P) blood pressure, height, weight and Body Mass Index (BMI) were also recorded.
Results
Comparing initial and final data, the results showed that there were no significant changes in the values of glucose and AST, but significant differences in TAG, TC, and HDL-C, were observed: TAG 233.7 ± 177.8 vs. 167.7 ± 100.7 mg/dL (p < 0.001), TC 181.7 ± 37.5 vs. 163.5 ± 34.4 mg/dL (p < 0.001), C-HDL 43.5 ± 14.4 vs. 50 ± 18.8 mg/dL (p < 0.01). The univariated analysis showed that the changes in the HDL-C and TC concentrations were dependent on TAG concentration (p = 0.247 and p = 0.108, respectively); nevertheless the calculated values for cholesterol associated to low density lipoprotein (LDL-C) were significantly reduced by the Spirulina maxima treatment but independently of the TAG changes. In addition, significant differences were found comparing initial and final SYST-P and DIAST-P blood pressure in both male and female: SYST-P male 121 ± 9 vs. 111 ± 8 mm Hg (p < 0.01), DIAST-P male 85 ± 6.5 vs. 77 ± 9 mm Hg (p < 0.01); SYST-P female 120 ± 9.5 vs. 109 ± 11 mm Hg (p < 0.002), DIAST-P female 85 ± 11 vs. 79 ± 7.5 mm Hg (p < 0.03).
Conclusion
The Spirulina maxima showed a hypolipemic effect, especially on the TAG and the LDL-C concentrations but indirectly on TC and HDL-C values. It also reduces systolic and diastolic blood pressure.
Similar content being viewed by others


Background
Chronic-degenerative diseases are a growingly health problem all over the world [1]. In Mexico, coronary heart disease and diabetes mellitus are the first and second leading causes of death between general population according to Statistics, Geography and Informatics' National Institute (INEGI) [2]. This has been related with recognized environmental factors as a high caloric diet intake, leak of exercise, tobacco and alcohol consumption and genetic predisposition [3–7]. It is well known that the modification on lipid concentration is a useful approach to decrease cardiovascular mortality through prevention on development of atherosclerotic disease [8–13].
Spirulina maxima, a filamentous and unicellular alga is a cyanobacterium belonging to the Oscillatoraceae family that usually grows in the alkaline waters of Africa, Asia, North and South America [14]. Spirulina has been used as food additive because of its high content of proteins as well as essential nutrients like carotenoids, vitamins and minerals [15–17]. In addition, previous studies have demonstrated its several biological activities such as inhibit viral replication [15, 18, 19], prevent anemia [20], decrease genotoxicity induced by drugs [21], prevent fatty liver disease [22–25] and has hypoglycemic [26] and hypolipemic properties [27–30]. It has also been studied its effects on vasomotor responses on aortic rings proposing its antihypertensive activities in experimental models [31–33]. At this point, only few studies have evaluated these effects on human population.
The purpose of this study was to evaluate the effects of Spirulina maxima, orally administered, on serum lipids and blood pressure in a Mexican population after six weeks of treatment, as a possible alternative treatment for dyslipidemia and hypertension.
Results
No changes were observed on AST and glucose values throughout the experimental period (35 ± 18 UI/L and 85 ± 13 mg/dL respectively, results not shown). On the other hand, as shown in Table 1, the initial concentration of lipids did not differ significantly between male (n = 16) and female (n = 20), suggesting their possible association as a single group. Because of the initial triacylglycerol concentrations were 254 ± 173 and 217 ± 184 mg/dL, for male and female groups, respectively, the values suggest a hypertriacylglycerolemic tendency in the studied sample. The other lipid values were in the optimal or limit ranges. In addition, both initial systolic and diastolic blood pressures did not differ significantly between male and female.
At the end of the experimental period there were significant differences in blood lipids after the Spirulina treatment (Table 2). Plasma TAG and TC concentrations were the most diminished (p = 0.001, Mann-Whitney and Student's-t tests) but LDL-C concentrations were also decreased (p = 0.01, Student's-t test), and HDL-C values were increased (p = 0.01, paired Mann-Whitney test). However, the univariate analysis showed that the changes on HDL-C and TC concentrations were dependent on TAG concentration (p = 0.247 and p = 0.108, respectively); while LDL-C concentration was independent of TAG values (p = 0.044). As mentioned before, there were no differences between initial and final AST or glucose concentration. Respect on blood pressure (Table 2) it was shown a significant difference between initial and final systolic and diastolic blood pressure records (p < 0.001 SYST-P; p < 0.05 DIAST-P, Tukey's comparison test). Furthermore, a significant decrease on systolic blood pressure was observed since the fourth week of Spirulina consumption (initial SYST-P 121 ± 9 vs. fourth week SYST-P 114 ± 10 mmHg, p < 0.05; vs. fifth week SYST-P 112 ± 8 mmHg, p < 0.01).
Dyslipidemia Prevalences
On the other hand, when the effects of Spirulina on dyslipidemia prevalences were assessed, the results (Table 3) show that the initial hypercholesterolemia prevalence (TC ≥ 200 mg/dL) was of 27.8%, but it was diminished after the treatment to 13.9%. The most important changes were observed if the higher values of cholesterol (TC ≥ 240 mg/dL) were used for the analysis of hypercholesterolemia, the initial prevalence was 8.3%; and after the Spirulina treatment was 0.0%. Initial hypoalphalipoproteinemia prevalence was 27.7% (10/36, cases); and at the end of treatment, prevalence was only 22.0% (8/36 cases). The initial prevalence of hypertriacylglycerolemia in the sample was 41.7% versus a final prevalence of 22.2%. Furthermore, significant differences were found between male and female groups (initial hypertriacylglycerolemia prevalence 62.5% vs. 25.8%, p = 0.026; final prevalence 43.8% vs. 5%, p = 0.008, respectively).
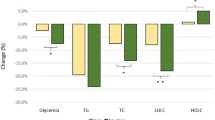
Dyslipidemia prevalences were analyzed in age terciles, with middle age groups of 29.3 ± 5.4 (18–38 years), 43.8 ± 2.7 (39–46 years) and 55.9 ± 5.9 (49–65 years). The results showed that according to the initial values, all of the groups showed hypertriacylglycerolemia cases with predominance (6/36) in the last group (49 to 65 years) whereas most hypercholesterolemic (6 or 3/36, CT >200 or 240 mg/dL, respectively) and hyperbetalipoproteinemic cases (5/36) belong to age group of 39–46 years. After the Spirulina treatment, the results showed that the eldest age group (49–65 years) was most responsive to the treatment (p < 0.001). The average change in TAG and TC values after treatment was -20% (-44 to -4, confidence intervals 95%) and -8% (-24 to -2, confidence intervals 95%), respectively. An increase tendency 27% on HDL-C concentration for all groups (5 to 50, confidence intervals of 95%) was observed.
High Blood pressure prevalence
According JNC 7 blood pressure reference values, high blood pressure prevalence was assessed in total sample before and after treatment with Spirulina (Table 4). The results show that the initial Hypertension type 2 prevalence was 14% (5/36 cases), but it was diminished after the treatment to 3% (1/36 case), whereas Hypertension type 1 prevalence diminished from 31% (11/36 cases) to 11% (4/36 cases). Furthermore, an increase on pre-hypertension prevalence from 44% (16/36 cases) to 50% (18/36 cases) and normal blood pressure prevalence from 11% (4/36 cases) to 36% (13/36 cases) were found.
Prevalences were analyzed by gender (Table 5). The results showed an initial high prevalence of Stage 1 of Hypertension in both male and female population (30% and 31%, respectively) that was decreased after treatment in both (6% and 15%, respectively) and in the case of stage 2 of hypertension, prevalence in men was decreased from 6% to 0% and in female was reduced from 20% to 5%. The most significant decrement in blood pressure was observed in the youngest group (18 – 38 years; p < 0.001), with an average change in SYST-P and DIAST-P of -8% (-17 to -3, confidence intervals 95%) and -6% (-12 to -1, confidence intervals 95%), respectively.
Discussion
Previous studies have demonstrated the hypolipemic activity of Spirulina maxima in rats with and without toxic substances [27–30]. Using a single intraperitoneal dose of 2 mL/kg carbon tetrachloride (CCl4) as an hepatotoxic in order to induce non alcoholic steatohepatitis, it was demostrated that 5% Spirulina maxima in diet decrease serum AST, liver TAG and TC in rats. The same pattern was observed in the liver free fatty acids (with an important decrease on unsaturated fatty acids) and thiobarbituric acid reactive substances [24]. These results suggest that Spirulina has hepatoprotective properties through decreasing on liver lipid profile and lipoperoxidation products. At this way, it has been demonstrated that Spirulina maxima prevents the development of fatty liver induced by simvastatin, ethanol and hypercholesterolemic diet in mice [29].
As previously mentionated, the purpose of this study was to evaluate the effects of Spirulina on human lipid metabolism and blood pressure levels. Parikh P et al., studied the effect of Spirulina supplementation at 2 g/day doses for two months on blood glucose levels, glycosylated hemoglobin and lipid profile of twenty-five diabetic type 2 subjects [26]. They found a lowering of fasting and postprandial blood glucose levels and in the HbA1c level; this findings contrast with our results, where glucose levels kept stable during all studied period. Respect on lipid profile, the same report demonstrates a reduction on TAG, TC and in the atherogenic indices TC/HDL-C and LDL-C/HDL-C. Samuels R et al., also observed these effects in patients with hyperlipidemic nephrotic syndrome after supplementation with 1 g/day in the same period [34].
In our study, TAG, TC and LDL-C showed a significant reduction with an increase on HDL-C concentration after a study period of six weeks. However, changes on TC and HDL-C were dependent in TAG concentration, meanwhile LDL-C values decreased after treatment in an independent way. Before treatment, a high prevalence of hypercholesterolemia (27.8%, > 200 mg/dL), hypertriacylglycerolemia (41.7%) and hypoalphalipoproteinemia (27.7%) was found; this observation contrast with a Mexican nationwide previous study where hypertriacylglycerolemia was the second most common dyslipidemia (24.3%) after hypoalphalipoproteinemia (46.2% for men and 28.7% for women) [35]; however, the prevalence of hypercholesterolemia was similar to that reported in a more recent study (26.5%) [36]. At this point, after treatment it was observed a significant decrease in all prevalence parameters studied with a major effect observed in the oldest age group (49–65 years). This is very important because a lot of chronic-degenerative disorders related with dyslipidemia, incrementing their prevalence in this age group [1, 13, 37, 38], could be attenuated with Spirulina consumption.
With regard to blood pressure, only 11% of studied population had normal levels before treatment, whereas 44% prehypertension, 31% hypertension stage 1 and 14% a stage 2. The hypertension prevalence on Mexican people has shown a clear increasing trend, 13.4% on 2000 survey to 22.7% on 2006 survey, indicating that the present prevalence (45%) could not represent the nationwide values [36]. According the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) criteria [39], patients with prehypertension or hypertension in any stage, have to include in their treatment a balanced diet and exercise. Several natural products have been used to help in the treatment of hypertensive patients. Lima-Landman et al., in normal and hypertensive rats demonstrated that an aqueous extract of dried leaves from Cecropia glaziovii Sneth had an antihypertensive effect [40]. Ojewole J et al., showed that Persea americana Mill aqueous leaf extract (25–800 mg/mL) caused bradycardia, vasorelaxation and hypotension in mammalian experimental models in response to a possibly increased synthesis and release of nitiric oxide [41]. After supplementation with Spirulina it was observed 14% hypertension prevalence, 36% patients reached a normal blood pressure whereas patients with hypertension stage 1 or 2 decreased their levels to prehypertension (50%). These changes were observed in men and women, and that youngest group was more blood pressure responsive to Spirulina than the other age groups (data not shown).
The action mechanisms of Spirulina on lipid metabolism and blood pressure are not well understood yet. Nagakoa S et al., found that a concentrate of Spirulina platensis inhibited jejunal cholesterol absorption and ileal bile acid reabsorption, proposing that C-phycocyanin it's the molecule responsible for this effect [42]. Li-Kun H et al., isolated an active component designed as glycolipid H-b2 and they found that this glycolipid inhibits pancreatic lipase activity in a dose-dependent manner, lowering rat plasma TAG levels [43]. Furthermore, they found that phycocyanin inhibits pancreatic lipase at the same way. These effects could explain the hypocholesterolemic and hypotriacylglycerolemic effects seen on Spirulina maxima, treated patients, but no studies have been conduced at the moment.
On other hand, a diet supplemented with Spirulina maxima has showed to prevent synthesis and release of vasoconstricting metabolites of arachidonic acid induced by fructose and attenuates tension development in response to phenylephrine [33]. Other reports, using an ethanolic extract, demonstrated an increased nitric oxide endothelium synthesis/release, a well known vasodilatation metabolite [31]. At this point, it's well known that blood pressure could be increased in patients that develop vasoconstriction in response to certain metabolites or due to atherosclerotic process [44]. Hypotension observed on patients could be explained on these effects. Hsiao G et al., have proposed that C-phycocyanin inhibits platelet aggregation through inhibition of calcium mobilization and mediation of free radicals released by platelet [45]. These could be supported by a well recognized effect of Spirulina mediating several steps on inflammation process that finally reduces atherotrombotic plaque formation. Guan Y et al., have also proposed that high potassium, and low sodium contents of Spirulina, have positive effects on blood pressure [46]. We found that supplementation with Spìrulina decreases LDL-C and increases HDL-C with a probably beneficial effect on atherotrombotic indices. Finally, our results also supported vasodilatation theory, as seen in a major effect of Spirulina in diastolic blood pressure mainly determinated by peripherical vessel resistance.
Actually, statins are recognized as the first-line therapy for cholesterol lowering. In a study conduced by Berne in type 2 diabetic patients, prescription of rosuvastatin (10 mg/day) by 4 weeks decreased significatively LDL-C levels in a mean percentage of 47.6%, TC in 33.6%, TAG in 19.2% and increased HDL-C in 4.4%, and demonstrated more response on lipid profile in comparison with atorvastatin at the same dose [47]. Rangineni V et al., using dried Eclipta alba leaf powder (3 g/day) in mild hypertensive subjects, observed a reduction on LDL-C, TC and TAG with mean percentages of 24%, 17% and 14%, respectively [48]. As mentionated before, treatment with Spirulina maxima, decreased significatively LDL-C, TC and TAG in a mean percentage of 17%, 8% and 20%, respectively, and increased HDL-C in 27%. These results support that Spirulina maxima could be used as an effective supplement on hypertriacilglycerolemic patients.
Respect of blood pressure, dried extract of Hibiscus sabdariffa, a widely used herbal medicinal product administrated for 4 weeks, decreased systolic and diastolic blood pressure in 11.58% and 12.21%, respectively [49]. At this way, Eclipta alba dried leaf powder reduced mean arterial pressure by 15% [48]. After treatment with Spirulina maxima, systolic and diastolic blood pressure decreased in a mean percentage of 8% and 6%, these results suggest that Spirulina maxima could be used as a supplement on blood pressure lowering therapy; however, these findings deserve more research in view that our study was performed in an open sample, non-representative and small population.
Finally, security on the use of Spirulina was demonstrated with no AST levels elevation trough evaluation period. There were no reports of adverse effects on population studied. Only idiosyncratic adaptative effects as: headache, flatulence, metheorism and increase of intestinal transit (not diarrhea) were reported on the first week of treatment. This is according with other reports where security of oral administration was studied [50–52].
Conclusion
The present results demonstrate that Spirulina maxima has hypolipemic effects, especially on the TAG concentration and the LDL-C but indirectly on TC and HDL-C values and positive effects on lowering blood pressure. We propose that because of these pharmacological properties, Spirulina could be used as a dietary supplement on dyslipidemic and hypertensive patients.
Materials and methods
Subjects
Sixty five adult volunteers of both genders were invited to participate in the experiment. All of them met the following inclusion criteria: Mexico City inhabitant, age ≥ 18 years old, engagement to complete the treatment, not known cardiovascular disease and not taking at the time of the study drugs known to affect lipid metabolism or blood pressure values, not even oral antidiabetic drugs or insulin. Individuals with Renal Failure or Hepatic Disease were excluded. Only thirty six participants concluded the evaluation period. The final participants were sixteen male and twenty female. The protocol and the aim of the study were fully explained to the subjects, who gave their written consent. The research was carried out in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the School of Medicine, UNAM, Mexico D.F.
Study design
It was determined an evaluation period of six weeks in order to observe changes on lipid levels before and after treatment with Spirulina maxima. During this time all volunteers were asked not to modify dietary habits or lifestyle to minimize the effects on lipids metabolism. At the beginning of the study and every week, blood samples were taken in the morning after a 12 h fasting and 15 min of rest, using blood collection tubes (BD Vacutainer) in order to observe initial and final levels on glucose, TAG, TC, HDL-C, and weekly AST levels to asses the non-hepatotoxical effect of treatment. Systolic and diastolic blood pressure, height and weight were also registered, and BMI was calculated. Spirulina maxima was orally consumed, 4.5 g/day (tablets of 0.5 g, 3 tablets each 8 hours approximately) for six weeks. The Spirulina used in this study was purchased from Spiral Spring, Mexico. The valuated composition of the tablet was: protein 57.35%, lipids 5.44 % (ether extract), ash 11.41 %, fiber 0.41 % and carbohydrates 25.33% on dry base analyses.
The prevalence of hyperlipidemia was registered both before and after the experimental period. Hypercholesterolemia was defined as TC levels more than 200 mg/dL or 240 mg/dL, according to Adult Treatment Panel (ATPIII or ATPII) recommendations [53, 54]. Hypoalphalipoproteinemia was defined as lower HDL-C values than 35 mg/dl, according to ATPII recommendations. Hypertriacylglycerolemia was defined as higher TAG values than 200 mg/dL, according to ATPII recommendations. Hyperbetalipoproteinemia was defined as higher LDL-C values than 130 mg/dL, according to ATPIII recommendations. Normal blood pressure was defined as values less than 120/80 mmHg for SYST-P and DIAST-P blood pressure, respectively. Prehypertension was defined as values of SYST-P blood pressure of 120–139 mmHg or DIAST-P blood pressure of 80–89 mmHg. Stage 1 of hypertension was defined as values of 140–159 mmHg for SYST-P blood pressure or 90–99 mmHg for DIAST-P blood pressure, meanwhile stage 2 was defined as higher values than 160/100 mmHg for SYST-P and DIAST-P blood pressure respectively, according criteria from The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) [39].
Anthropometric measurements
The height was measured using a rigid stadiometer. Weight of subjects, in light clothing, was measured in a calibrated balance scale. BMI was calculated as the weight (kg) divided by the height (m) squared (kg/m2). Blood pressure was measured using a sphygmomanometer by auscultatory method. Anthropometrical details of subjects are shown in Table 6.
Laboratory analyses
Blood for plasma analyses was drawn into 100 units sodium heparin (USP) freeze-dried sterile glass tubes (BD Vacutainer) and centrifuged at 4,000 × g for 5 minutes at 4°C. Total cholesterol and TAG concentrations were analyzed by using standard enzymatic procedures (Jas Diagnostics, Inc. Mexico) with a spectrophotometer (Genesys 10 UV, Thermo Electron Corporation, USA); HDL-C concentration was measured after precipitation of apo B-containing lipoproteins with precipitation reactive (Roche, Mexico); LDL-C concentration was determined by using the Friedewald's formula modified by De Long D et al. [55]; AST and glucose were measured with an enzymatic kit (Merck, Mexico) by spectrophotometry methods.
Statistical analysis
Frequency distribution for variables was determined by Kolmogorov-Smirnov test. Comparisons between groups were done using Student's t test, Mann-Whitney's test or Tukey's multiple comparison test, when appropriate. In order to evaluate dependency of TAG changes, univariated analysis was performed. Significant differences between prevalences were assessed with Chi-squared test using contingency tables. Statistical analyses were performed using SPSS for Windows software (version 10.0). Results are expressed as mean ± S.D.
References
Crews DE: Senescence, aging, and disease. J Physiol Anthropol. 2007, 26: 365-372. 10.2114/jpa2.26.365
Statistic, Geography and Informatics' National Institute (INEGI). http://www.inegi.gob.mx
Garcia-Garcia G, Aviles-Gomez R, Luquin-Arellano VH, Padilla-Ochoa R, Lepe-Murillo L, Ibarra-Hernandez M, Briseño-Renteria G: Cardiovascular risk factors in the Mexican population. Ren Fail. 2006, 28: 677-687. 10.1080/08860220600936096
Comuzzie AG, Mitchell BD, Cole S, Martin LJ, Hsueh WC, Rainwater DL, Almasy L, Stern MP, Hixson J, MacCluer JW, Blangero J: The genetics of obesity in Mexican Americans: the evidence from genome scanning effects in the San Antonio family heart study. Hum Biol. 2003, 75: 635-646. 10.1353/hub.2003.0073
Mitchell BD, Almasy LA, Rainwater DL, Schneider JL, Blangero J, Stern MP, MacCluer JW: Diabetes and hypertension in Mexican American families: relation to cardiovascular risk. Am J Epidemiol. 1999, 149: 1047-1056.
Mitchell BD, Kammerer CM, Blangero J, Mahaney MC, Rainwater DL, Dyke B, Hixson JE, Henkel RD, Sharp RM, Comuzzie AG, VandeBerg JL, Stern MP, MacCluer JW: Genetic and environmental contributions to cardiovascular risk factors in Mexican Americans. The San Antonio Family Heart Study. Circulation. 1999, 94: 2159-2170.
Gonzalez C, Stern MP, Gonzalez E, Rivera D, Simon J, Islas S, Haffner S: The Mexico City Diabetes Study: a population based approach to the study of genetic and environmental interactions in the pathogenesis of obesity and diabetes. Nutr Rev. 1999, 57: S71-S76.
Gille A, Bodor ET, Ahmed K, Offermanns S: Nicotinic Acid: pharmacological effects and mechanism of action. Annu Rev Pharmacol Toxicol. 2008.
Frisinghelli A, Mafrici A: Regression or reduction in progression of atherosclerosis, and avoidance of coronary events, with lovastatin in patients with or at high risk of cardiovascular disease: a review. Clin Drug Investig. 2007, 27: 591-604. 10.2165/00044011-200727090-00001
Singh IM, Shishehbor MH, Ansell BJ: High-density lipoprotein as a therapeutic target: a systematic review. JAMA. 2007, 298: 786-798. 10.1001/jama.298.7.786
Wiklund O, Håversen L, Pettersson C, Hultén LM: How can we prevent cardiovascular disease in diabetes. J Intern Med. 2007, 262: 199-207. 10.1111/j.1365-2796.2007.01828.x
Laclaustra M, Frangi AF, Casasnovas JA, Cia P: Association of endothelial function and vascular data with LDL-c and HDL-c in a homogeneous population of middle-aged, healthy military men: Evidence for a critical role of optimal lipid levels. Int J Cardiol. 2007.
Gadi R, Samaha FF: Dyslipidemia in type 2 diabetes mellitus. Curr Diab Rep. 2007, 7: 228-234. 10.1007/s11892-007-0036-0
Ciferri O: Spirulina, the edible microorganism. Microbiol Rev. 1983, 47: 551-578.
Khan Z, Bhadouria P, Bisen PS: Nutritional and therapeutic potential of Spirulina. Curr Pharm Biotechnol. 2005, 6: 373-379. 10.2174/138920105774370607
Belay A, Kato T, Ota Y: Spirulina (Arthrospira): potencial application as an animal feed supplement. J Appl Phycol. 1996, 8: 303-311. 10.1007/BF02178573.
Chamorro G, Salazar M, Favila L, Bourges H: Pharmacology and toxicology of Spirulina alga. Rev Invest Clin. 1996, 48 (5): 389-399.
Ayehunie S, Belay A, Baba TW, Ruprecht RM: Inhibition of HIV-1 replication by an aqueous extract of Spirulina platensis (Arthrospira platensis). J Acquir Immune Defic Syndr Hum Retrovirol. 1998, 18: 7-12.
Hayashi K, Hayashi T, Kojima I: A natural sulfated polysaccharide, calcium spirulan, isolated from Spirulina platensis: in vitro and ex vivo evaluation of anti-herpes simplex virus and anti-human immunodeficiency virus activities. AIDS Res Hum Retroviruses. 1996, 12: 1463-1471.
Kapoor R, Metha U: Supplementary effect of Spirulina on hematological status of rats during pregnancy and lactation. Plant Foods Hum Nutr. 1998, 52: 315-324. 10.1023/A:1008027408919
Premkumar K, Abraham SK, Santhiya ST, Ramesh A: Protective effect of Spirulina fusiformis on chemical-induced genotoxicity in mice. Fitoterapia. 2004, 75: 24-31. 10.1016/j.fitote.2003.07.008
Torres-Duran PV, Miranda-Zamora R, Paredes-Carbajal MC, Mascher D, Diaz-Zagoya JC, Juarez-Oropeza MA: Spirulina maxima prevents induction of fatty liver by carbon tetrachloride in the rat. Biochem Mol Bio Int. 1998, 44: 768-793.
Vadiraja HB, Gaikwad NW, Madyashta KM: Hepatoprotective effect of C-phycocyanin: protection for carbon tetrachloride and R-(+)-pulegone-mediated. Biochem Biophys Res Commun. 1998, 249: 428-431. 10.1006/bbrc.1998.9149
Torres-Duran PV, Paredes-Carbajal MC, Mascher D, Zamora-Gonzalez J, Diaz-Zagoya JC, Juarez-Oropeza MA: Protective effects of Arthrospira maxima on fatty acid composition in fatty liver. Arch Med Res. 2006, 37: 479-483. 10.1016/j.arcmed.2005.08.005
Kato T, Takemoto K: Effects of Spirulina on hypercholesterolemia and fatty liver in rats. Japan Nutr Foods Assoc J. 1984, 37: 321-
Parikh P, Mani U, Iver U: Role of Spirulina in the control of glicemia and lipidemia in type 2 Diabetes Mellitus. J Med Food. 2001, 4: 193-199. 10.1089/10966200152744463
Mazo VK, Gmoshinskñ IV, Zilova IS: Microalgae Spirulina in human nutrition. Vopr Pitan. 2004, 73: 45-53.
Nayaka N, Homma Y, Goto Y: Cholesterol lowering effect of Spirulina. Nutr Rep Int. 1988, 37: 1329-1337.
Ble-Castillo JL, Rodriguez-Hernandez A, Miranda-Zamora R, Juarez-Oropeza MA, Diaz-Zagoya JC: Arthrospira maxima prevents the acute fatty liver induced by the administration of simvastatin, ethanol and a hypercholesterolemic diet to mice. Life Sci. 2002, 70: 2665-2673. 10.1016/S0024-3205(02)01512-6
Iwata K, Inayama T, Kato T: Effects of Spirulina platensis on plasma lipoprotein lipase activity in fructose-induced hyperlipidemic rats. J Nutr Sci Vitaminol. 1990, 36: 165-171.
Mascher D, Paredes-Carbajal MC, Torres-Duran PV, Zamora-Gonzalez J, Diaz-Zagoya JC, Juarez-Oropeza MA: Ethanolic extract of Spirulina maxima alters the vasomotor reactivity of aortic rings from obese rats. Arch Med Res. 2006, 37: 50-57. 10.1016/j.arcmed.2005.04.004
Paredes-Carabajal MC, Torres-Duran PV, Diaz-Xagoya JC, Mascher D, Juarez-Oropeza MA: Effects of dietary Spirulina maxima on endothelium dependent vasomotor responses of rat aortic rings. Life Sci. 1997, 61: 211-219. 10.1016/S0024-3205(97)00715-7.
Paredes-Carbajal MC, Torres-Duran PV, Diaz-Zagoya JC, Mascher D, Juarez-Oropeza MA: Effects of dietary Spirulina maxima on vasomotor aorta ring from rats fed a fructose-rich diet. Nutr Res. 1997, 18: 1769-1782. 10.1016/S0271-5317(98)00140-7.
Samuels R, Mani UV, Nayak US: Hypocholesterolemic effect of Spirulina in patients with hyperlipidemic nephrotic syndrome. J Med Food. 2002, 5: 91-96. 10.1089/109662002760178177
Aguilar-Salinas CA, Olaniz G, Valles V, Rios-Torres JM, Gomez-Perez FJ, Rull JA, Rojas R, Franco A, Sepulveda J: High prevalence of low HDL cholesterol concentrations and mixed hyperlipidemia in a Mexican nationwide survey. J Lipid Res. 2001, 42: 1298-1307.
Olaiz-Fernandez G, Rivera-Dommarco J, Shamah-Levy T, Rojas R, Villalpando-Hernandez S, Hernandez-Avila M, Sepulveda-Amor J, : Mexican National Health and Nutrition Survey 2006. 2006, Cuernavaca, Mexico: National Public Health Institute.
Stern MP, Williams K, Hunt KJ: Impact of diabetes/metabolic syndrome in patients with established cardiovascular disease. Atheroscler Suppl. 2005, 6: 3-6. 10.1016/j.atherosclerosissup.2005.02.002
Hayden MR: Atherogenic dyslipidemia. J Cardiometab Syndr. 2006, 1: 166-167.
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jones DW, Materson BJ, Oparil S, Wright JT, Roccella EJ, : The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003, 289: 2560-2572. 10.1001/jama.289.19.2560
Lima-Landman MT, Borges AC, Cysneiros RM, De Lima TC, Souccar C, Lapa AJ: Antihypertensive effect of a standardized aqueous extract of Cecropia glaziovii Sneth in rats: an in vivo approach to the hypotensive mechanism. Phytomedicine. 2007, 14: 314-320. 10.1016/j.phymed.2007.03.003
Ojewole JA, Kamadyaapa DR, Gondwe MM, Moodley K, Musabayane CT: Cardiovascular effects of Persea Americana Mill (Lauraceae) (avocado) aqueous leaf extract in experimental animals. Cardiovasc J S Afr. 2007, 18: 69-76.
Nagaoka S, Shimizu K, Kaneko H, Shibayama F, Morikawa K, Kanamaru Y, Otsuka A, Hirashi T, Kato T: A novel protein C-phycocyanin plays a crucial role in the hypocholesterolemic action of Spirulina platensis concentrate in rats. J Nutr. 2005, 135: 2425-2430.
Li-Kun H, Dong-**a L, Lan X, **ao-Jie G, Yasumasa K, Isao S, Hiromichi O: Isolation of pancreatic lipase activity-inhibitory component of Spirulina platensis and it reduce postprandial triacylglycerolemia. Yakugaku Zasshi. 2006, 126: 43-49. 10.1248/yakushi.126.43
Schiffrin EL: A critical review of the role of endothelial factors in the pathogenesis of hypertension. J Cardiovasc Pharmacol. 2001, 38: S3-S6.
Hsiao G, Chou Po-Hsiu, Shen Ming-Yi, Chou Duen-Suey, Lin Chien-Huang, Sheu Joen-Rong: C-phycocyanin, a very potent and novel platetel aggregation inhibitor from Spirulina platensis. J Agric Food Chem. 2005, 53: 7734-7740. 10.1021/jf051352y
Guan Y, Zhao HY, Ding XF, Zhu YY: Analysis of the contents of elements in Spirulina from different producing areas. Guang Pu Xue Yu Guang Pu Fen **. 2007, 27: 1029-1031.
Berne C, Siewert-Delle A, : Comparison of rosuvastatin and atorvastatin for lipid lowering in patients with type 2 diabetes mellitus: results from the URANUS study. Cardiovasc Diabetol. 2005, 3: 4-7.
Rangineni V, Sharada D, Saxena S: Diuretic, hypotensive, and hypocholesterolemic effects of Eclipta alba in mild hypertensive subjects: a pilot study. J Med Food. 2007, 10: 143-148. 10.1089/jmf.2006.0000
Herrera-Arellano A, Miranda-Sanchez J, Avila-Castro P, Herrera-Alvarez S, Jimenez-Ferrer JE, Zamilpa A, Roman-Ramos R, Ponce-Monter H, Tortoriello J: Clinical effects produced by a standardized herbal medicinal product of Hibiscus sabdariffa on patients with hypertension. A randomized, double-blind, lisinopril-controlled clinical trial. Planta Med. 2007, 73: 6-12. 10.1055/s-2006-957065
Chamorro G, Salazar M, Salazar S: Estudio teratogenico de Spirulina en rata. Arch Latinoam Nutr. 1989, 29: 641-649.
Chamorro GA, Herrera G, Salazar M, Salazar S, Ulloa V: Subchronic toxicity study in rats fed Spirulina. J Pharm Belg. 1988, 24: 104-106.
Salazar M, Salazar S, Steele CE, Chamorro GA: Subchronic toxicity study in mice fed Spirulina maxima. J Ethnopharmacol. 1998, 62: 235-241. 10.1016/S0378-8741(98)00080-4
Rubinstein A: National Cholesterol Education Program, second report of the Expert Panel on detection, evaluation, and treatment of high blood cholesterol in adults. Circulation. 1995, 91: 908-909.
, : Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA. 2001, 285: 2486-2497. 10.1001/jama.285.19.2486
De Long DM, De Long ER, Wood PD, Lippel K, Rifkind BM: A comparison of methods for the estimation of plasma low- and very low-density lipoprotein cholesterol. The Lipid Research Clinics Prevalence Study. JAMA. 1986, 256: 2372-2377. 10.1001/jama.256.17.2372
Acknowledgements
This work was supported in part by a grant from PAPIIT-UNAM (IN218107, MAJO). We also thank Celia Virginia Sanchez Meza and Rebeca Milan for their technical assistance during the blood collection and anthropometric measurements. In recognition to Jose Zamora who's life was devoted to science and friendship.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
PVTD participated in the collection, design, analysis and interpretation of data and writing of the manuscript; AFH participated in the collection and analysis of data and performed the statistical analysis and writing of the manuscript; MAJO participated in the design, analysis and interpretation of data and writing of the manuscript. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Torres-Duran, P.V., Ferreira-Hermosillo, A. & Juarez-Oropeza, M.A. Antihyperlipemic and antihypertensive effects of Spirulina maxima in an open sample of mexican population: a preliminary report. Lipids Health Dis 6, 33 (2007). https://doi.org/10.1186/1476-511X-6-33
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1476-511X-6-33