
Abstract
Objective
To assess the intake of sugar-added beverages such as soft drinks and commercially available fruit juices in kindergarten children, and to examine its association with obesity indices, physical activity levels and dietary habits.
Methods
A total of 856 children aged 4–7 years living in Crete, Greece in 2004–5 were included in this cross-sectional study. Nutrient and food intake was assessed with the use of 3-day weighed food records. Body measurements were used in order to assess BMI and waist circumference, and moderate-to-vigorous physical activity was calculated with the use of a questionnaire.
Results
Approximately 59.8% of all children consumed sugar-added beverages on a daily basis. High intake of sugar-added beverages (> 250 g/day) was associated with low intakes of calcium (p < 0.001), vitamin A and E (p < 0.010), fruits and vegetables (p = 0.007), and milk and yogurt (p = 0.048). Compared to non or low consumers, high consumers of sugar-added beverages (> 250 g/day) had higher BMI levels and two times greater risk of being overweight and/or obese (OR:2.35, p = 0.023).
Conclusion
High intake of sugar-added beverages in kindergarten children is associated with poor eating habits and inadequate nutrient intake, as well as increased risk for develo** childhood obesity.
Similar content being viewed by others


Background
Increasing rates of childhood obesity, starting from preschool age, is a worldwide phenomenon [1–3]. In Greece it is estimated that the overall prevalence of overweight and obesity in school children aged 6–17 years old is 17.3% and 3.6% respectively [4], whereas for preschool children (1–5 years old) it is 14.2% and 7.5% respectively [5].
Increased intake of sugar-sweetened beverages, such as soft drinks and commercially available fruit juices, amongst a number of other factors such as fast food eating, breakfast skip**, inactivity, and increased TV viewing hours, is thought to contribute to weight gain and risk of obesity in childhood and adolescence [6–12]. These data are consistent with the findings in the adult population where increased intake of sweetened beverages is associated with weight gain and increased risk of chronic diseases such as diabetes [13, 14].
A number of studies have suggested a potential association between soft drink intake and prevalence of childhood obesity [15]. The data for Greece is, however, limited. The 2000–2001 World Health Organization Report stated that less than 20% of Greek adolescents were daily soft-drink consumers, placing Greece very low in the worldwide ranking of soft-drink consumption. However, the Greek Health-Behavior-in-Schoolaged-Children study indicated that more than half of 11–15 year olds consume soda drinks on a daily basis [16]. Only a few studies are available on Greek children's dietary habits including soft drink consumption, but none of these covered kindergarten children. General trends are indicated by the National Statistical Service of Greece, which reported a striking increase of soft-drink consumption per person per year from 17.2 L in 1972 to 44.6 L in 2005 http://www.statistics.gr, while overall consumption of soft drinks and other sweetened beverages was 60 L per capita in 2005.
The aim of the present study was to assess the intake of sugar-added beverages such as soft drinks and commercially available fruit juices in kindergarten children of Crete, and to examine its association with obesity indices, physical activity levels and dietary habits.
Methods
Study population
The study was conducted in 2004–5 in all public kindergartens of the county of Chania in Crete. The age range of kindergarten children recruited in this study was 4–7 years of age. The present study is part of a larger intervention study [17]. It involves the baseline measurements performed in kindergarten children in order to assess their nutritional and health status before entering a nutrition education intervention study.
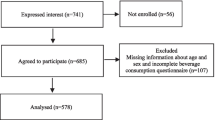
Out of 2630 kindergarten children, 1988 accepted to participate (77%). Another 233 children did not participate in the measurements either because they were not present at school or they were sick on the day of the examination. Finally, the 3-day weighed food records were returned for 856 (49%) children and were included in the analyses of the present study.
Parents gave written consent for the children's participation after having been fully informed both orally and in writing. The study was approved by the Greek Ministry of Education and the Ethics Committee of the University of Crete.
Dietary intake assessment
Three-day weighed food records were completed by the children's parents after they were given detailed oral and written instructions. Food records included two work days and one weekend day. Brands of products as well as methods of preparation were also recorded. Nutrient and food groups' intake was assessed as the mean of the 3-day weighed food records. The food group of sugar-added beverages included soft drinks and commercially available fruit juices with added sugar (excluding isotonic drinks).
The dietary software "Greek Diet", used to calculate dietary intakes, was initially created in 1990 by the Preventive Medicine and Nutrition Clinic of the University of Crete and later, in 1998, was upgraded using the USDA Nutrient Database for Standard Reference (release 11, 1996; USDA Agricultural Research Service, Washington, DC, USA). An extensive description of the database is given elsewhere [18].
Physical activity questionnaire
A physical activity questionnaire, completed by the parents, was used to assess moderate-to-vigorous physical activity (MVPA). MVPA was defined as continuous vigorous activity causing sweating and heavy breathing for periods longer than 15 minutes, but with occasional breaks in intensity, rather than the strict aerobic definition of 20 continuous minutes appropriate to older children and adults [19]. Parents were questioned about the frequency, intensity and duration of any regular physical activity of their child (average minutes per week) as well as registration in any after-school physical activity-related classes. Information on sedentary behavior such as TV viewing or computer use was also recorded. The questionnaire used has been validated by heart rate monitoring [20].
Body measurements
Length and height of children were measured to the nearest 0.1 cm using a short stadiometer for children > 6 years of age, and in the supine position for children < 6 years of age. Weight in light clothes was measured to the nearest 0.1 kg on a portable electronic scale (Seca model 770). Waist circumference (WC) was measured at the level of umbilicus at minimal respiration to the nearest 0.1 cm.
Defining adiposity status
BMI was calculated as body weight (kg) divided by height (m) squared. Subjects were classified as overweight and obese, according to the cut-offs for childhood overweight and obesity adopted by the International Obesity Task Force [21]. With regard to WC, children were categorized according to the 90th percentiles of Cretan children for their gender and age [22]. Children above the 90th percentile of WC were classified as overweight and obese.
Statistical analysis
The SPSS, version 15.0, statistical program was used for all analyses.
To assess for potential selection bias, we compared the basic characteristics between the children who returned the 3-day weighed food records and those who did not (856 vs 879). There was no significant difference in the distribution of gender (χ2 test, p = 0.227), age (student t-test, p = 0.387) and BMI (student t-test, p = 0.147) between responders and non-responders.
Chi-square (χ2) test was used for detecting differences in main characteristics between two genders. Intake of sugar-added beverages was divided into four categories: a. no consumption, b. < 150 grams/day, c. 151–250 grams/day and d. > 250 grams/day. Analysis of Covariance (linear trend) was used to estimate increase in nutrient intake, food consumption, body measurements and MVPA levels within the four groups (heterogeneity was tested by Levene's test).
Logistic regression analysis was used for estimating the risk (Odds Ratios-OR) of being overweight and/or obese (International Obesity Task Force criteria for BMI and > 90th sex-age percentiles for WC) in relation to sugar-added beverage consumption. The reference category was children that were non-consumers. Gender, age, BMI, energy intake and birth weight were used as covariates.
Results
Table 1 shows that overall 19% (n = 160) and 10.8% (n = 91) of the children were overweight and obese, respectively. Boys had significantly higher energy intake than girls (p < 0.05), whereas no other differences were found with regard to BMI, MVPA and intake of sugar-added beverages between the genders. Overall, 59.8% of all children were regular consumers of sugar-added beverages.
Table 2 shows that those in the highest category of sugar-added beverage intake also had higher intake of total energy, carbohydrate and vitamin C (p for trend < 0.001) than non- or low-consumers. Furthermore, high consumers of sugar-added beverages consumed significantly less calcium, vitamin A and E (p for trend < 0.010), fruit and vegetables (p for trend = 0.007), milk and yogurt (p for trend = 0.048), and olive oil (p for trend = 0.008). Intake of sugar-added beverages was positively associated with intake of sugar not contained in beverages and sweet and/or savory snacks (p for trend = 0.003 and 0.041, respectively). Table 2 also shows that high consumers of sugar-added beverages had higher levels of BMI (p for trend = 0.003), whereas MVPA did not differ between all types of consumers and non-consumers.
Children consuming > 250 g of sugar-added beverages per day had two times higher risk of being obese according to their BMI (OR = 2.35, p = 0.023) and WC (OR = 2.07, p = 0.028), when compared to non-consumers with BMI and WC within the normal ranges (Figures 1 and 2).

Risk (odds ratio) for Body Mass Index of kindergarten children of Crete in relation to consumption of sugar-added beverages. Logistic regression analysis. Gender, age, energy intake and birth weight were used as covariates. BMI cut-offs for overweight and obesity were determined by International Obesity Task Force criteria.

Risk (odds ratio) for Waist circumference of kindergarten children of Crete in relation to consumption of sugar-added beverages. Logistic regression analysis. Gender, age, energy intake and birth weight were used as covariates. The 90th percentiles of waist circumference were estimated by gender-age categories.
Discussion
In the present study almost 30% of kindergarten children were overweight and/or obese, whereas 60% of the children were daily consumers of sugar-added beverages.
In agreement with other studies [14, 23, 24], the present study indicates that intakes of milk and yogurt, calcium and vitamin A decrease as sugar-added beverages become a favorite choice of children on a daily basis (> 250 g/d). This finding points to a significant risk factor for impaired calcification of growing bones, since high phosphate levels of soda drinks could affect calcium metabolism. The importance of adequate calcium intake from an early age is underlined by the fact that it can prevent bone loss and osteoporosis in adult life [25–30].
Low fruit and vegetable consumption in high consumers of sugar-added beverages led to low intake of vitamin A and E. Such an effect could have adverse health effects in the long-term, since fruit and vegetable consumption is inversely associated with some types of cancer, diabetes and heart diseases [31–33]. More importantly 'healthy' dietary habits established in early childhood contribute to similar habits later in life and influence adult health [34, 35].
High vitamin C intake of high sugar-added beverages consumers could be explained by the fact that commercially available sweetened fruit juices are usually enriched with vitamins.
Risk of overweight and obesity in high consumers of sugar-added beverages was twice as high as in low- or non-consumers. Increased total energy intake and similar levels of MVPA could explain the increased risk of obesity in high-consumers as compared to non- or low-consumers. Analysis of the National Health and Nutrition Examination Survey data [36] regarding preschool children showed higher daily energy intake for those consuming sweetened fruit juices and sugar-added soft drinks, and a positive association between soft drink intake and overweight [12]. In this context, other studies have shown that soft drink consumption is related with short stature and obesity in preschool children [8], as well as weight gain [7] and increased risk of obesity in school children [37]. In particular, risk of obesity was found to increase by 60 % for each serving of sweetened beverages in adolescents [37], whereas overweight preschool children consuming soft drinks were more likely to retain their increased weight [38]. Moreover, James et al. showed that after 1 year of a school based education program on nutrition children reduced their intake of soft drinks and prevalence of overweight declined [39].
Conclusion
In conclusion, the present study indicates that high intake of sugar added beverages is associated with unfavourable nutritional status as well as high levels of obesity in kindergarten children of Crete. It seems that in Greece there is limited awareness of the potential risks to children's health that could be related to the unrestricted intake of sugar-added beverages. Policies on banning sugar-added beverages being purchased at schools as well as implementing nutrition education programmes, which have been adopted elsewhere in Europe, could be beneficial in the battle against rising prevalence of childhood overweight and obesity in Crete.
References
de Onis M, Blossner M: Prevalence and trends of overweight among preschool children in develo** countries. Am J Clin Nutr. 2000, 72 (4): 1032-1039.
Ogden CL, Flegal KM, Carroll MD, Johnson CL: Prevalence and trends in overweight among US children and adolescents, 1999-2000. JAMA. 2002, 288 (14): 1728-1732. 10.1001/jama.288.14.1728.
Reilly JJ, Dorosty AR, Emmett PM: Prevalence of overweight and obesity in British children: cohort study. BMJ. 1999, 319 (7216): 1039-
Georgiadis G, Nassis GP: Prevalence of overweight and obesity in a national representative sample of Greek children and adolescents. Eur J Clin Nutr. 2007, 61 (9): 1072-1074. 10.1038/sj.ejcn.1602619.
Manios Y, Costarelli V, Kolotourou M, Kondakis K, Tzavara C, Moschonis G: Prevalence of obesity in preschool Greek children, in relation to parental characteristics and region of residence. BMC Public Health. 2007, 7: 178-10.1186/1471-2458-7-178.
Ariza AJ, Chen EH, Binns HJ, Christoffel KK: Risk factors for overweight in five- to six-year-old Hispanic-American children: a pilot study. J Urban Health. 2004, 81 (1): 150-161.
Berkey CS, Rockett HR, Field AE, Gillman MW, Colditz GA: Sugar-added beverages and adolescent weight change. Obes Res. 2004, 12 (5): 778-788. 10.1038/oby.2004.94.
Dennison BA, Rockwell HL, Baker SL: Excess fruit juice consumption by preschool-aged children is associated with short stature and obesity. Pediatrics. 1997, 99 (1): 15-22.
Giammattei J, Blix G, Marshak HH, Wollitzer AO, Pettitt DJ: Television watching and soft drink consumption: associations with obesity in 11- to 13-year-old schoolchildren. Arch Pediatr Adolesc Med. 2003, 157 (9): 882-886. 10.1001/archpedi.157.9.882.
Gillis LJ, Bar-Or O: Food away from home, sugar-sweetened drink consumption and juvenile obesity. J Am Coll Nutr. 2003, 22 (6): 539-545.
Nicklas TA, Yang SJ, Baranowski T, Zakeri I, Berenson G: Eating patterns and obesity in children. The Bogalusa Heart Study. Am J Prev Med. 2003, 25 (1): 9-16. 10.1016/S0749-3797(03)00098-9.
Troiano RP, Briefel RR, Carroll MD, Bialostosky K: Energy and fat intakes of children and adolescents in the united states: data from the national health and nutrition examination surveys. Am J Clin Nutr. 2000, 72 (5 Suppl): 1343S-1353S.
Schulze MB, Manson JE, Ludwig DS, Colditz GA, Stampfer MJ, Willett WC, Hu FB: Sugar-sweetened beverages, weight gain, and incidence of type 2 diabetes in young and middle-aged women. JAMA. 2004, 292 (8): 927-934. 10.1001/jama.292.8.927.
Vartanian LR, Schwartz MB, Brownell KD: Effects of soft drink consumption on nutrition and health: a systematic review and meta-analysis. Am J Public Health. 2007, 97 (4): 667-675. 10.2105/AJPH.2005.083782.
Rajeshwari R, Yang SJ, Nicklas TA, Berenson GS: Secular trends in children's sweetened-beverage consumption (1973 to 1994): the Bogalusa Heart Study. J Am Diet Assoc. 2005, 105 (2): 208-214. 10.1016/j.jada.2004.11.026.
Yannakoulia M, Karayiannis D, Terzidou M, Kokkevi A, Sidossis LS: Nutrition-related habits of Greek adolescents. Eur J Clin Nutr. 2004, 58 (4): 580-586. 10.1038/sj.ejcn.1601849.
Vardavas CI, Tzatzarakis MN, Tsatsakis AM, Athanasopoulos D, Balomenaki E, Linardakis MK, Kafatos AG: Biomarkers of passive smoking among Greek preschool children. Eur J Pediatr. 2006, 165 (12): 891-896. 10.1007/s00431-006-0196-y.
Kafatos A, Verhagen H, Moschandreas J, Apostolaki I, Van Westerop JJ: Mediterranean diet of Crete: foods and nutrient content. J Am Diet Assoc. 2000, 100 (12): 1487-1493. 10.1016/S0002-8223(00)00416-8.
Baranowski T, Hooks P, Tsong Y, Cieslik C, Nader PR: Aerobic physical activity among third- to sixth-grade children. J Dev Behav Pediatr. 1987, 8 (4): 203-206. 10.1097/00004703-198708000-00003.
Manios Y, Kafatos A, George. M: Physical Activity of 6-year-old children:Validation of two proxy Reports. Pediatric Exercise Science. 1998, 10: 176-188.
Cole TJ, Bellizzi MC, Flegal KM, Dietz WH: Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. 2000, 320 (7244): 1240-1243. 10.1136/bmj.320.7244.1240.
Linardakis M, Vardavas CI, Kafatos A: Waist circumference percentiles of children of Crete aged 3 to 16 years. Paediatriki (in Greek). 2007, 70: 300-307.
Bowman SA: Beverage choices of young females: changes and impact on nutrient intakes. J Am Diet Assoc. 2002, 102 (9): 1234-1239. 10.1016/S0002-8223(02)90273-7.
Harnack L, Stang J, Story M: Soft drink consumption among US children and adolescents: nutritional consequences. J Am Diet Assoc. 1999, 99 (4): 436-441. 10.1016/S0002-8223(99)00106-6.
Ilich JZ, Skugor M, Hangartner T, Baoshe A, Matkovic V: Relation of nutrition, body composition and physical activity to skeletal development: a cross-sectional study in preadolescent females. J Am Coll Nutr. 1998, 17 (2): 136-147.
Teegarden D, Lyle RM, Proulx WR, Johnston CC, Weaver CM: Previous milk consumption is associated with greater bone density in young women. Am J Clin Nutr. 1999, 69 (5): 1014-1017.
Matkovic V, Ilich JZ: Calcium requirements for growth: are current recommendations adequate?. Nutr Rev. 1993, 51 (6): 171-180.
Prentice A: The relative contribution of diet and genotype to bone development. Proc Nutr Soc. 2001, 60 (1): 45-52.
Stewart TL, Ralston SH: Role of genetic factors in the pathogenesis of osteoporosis. J Endocrinol. 2000, 166 (2): 235-245. 10.1677/joe.0.1660235.
Gennari C: Calcium and vitamin D nutrition and bone disease of the elderly. Public Health Nutr. 2001, 4 (2B): 547-559. 10.1079/PHN2001140.
Block G, Patterson B, Subar A: Fruit, vegetables, and cancer prevention: a review of the epidemiological evidence. Nutr Cancer. 1992, 18 (1): 1-29.
Feskens EJ, Virtanen SM, Rasanen L, Tuomilehto J, Stengard J, Pekkanen J, Nissinen A, Kromhout D: Dietary factors determining diabetes and impaired glucose tolerance. A 20-year follow-up of the Finnish and Dutch cohorts of the Seven Countries Study. Diabetes Care. 1995, 18 (8): 1104-1112. 10.2337/diacare.18.8.1104.
Bazzano LA, Serdula MK, Liu S: Dietary intake of fruits and vegetables and risk of cardiovascular disease. Curr Atheroscler Rep. 2003, 5 (6): 492-499. 10.1007/s11883-003-0040-z.
Mikkila V, Rasanen L, Raitakari OT, Pietinen P, Viikari J: Longitudinal changes in diet from childhood into adulthood with respect to risk of cardiovascular diseases: The Cardiovascular Risk in Young Finns Study. Eur J Clin Nutr. 2004, 58 (7): 1038-1045. 10.1038/sj.ejcn.1601929.
Ness AR, Maynard M, Frankel S, Smith GD, Frobisher C, Leary SD, Emmett PM, Gunnell D: Diet in childhood and adult cardiovascular and all cause mortality: the Boyd Orr cohort. Heart. 2005, 91 (7): 894-898. 10.1136/hrt.2004.043489.
O'Connor TM, Yang SJ, Nicklas TA: Beverage intake among preschool children and its effect on weight status. Pediatrics. 2006, 118 (4): e1010-8. 10.1542/peds.2005-2348.
Ludwig DS, Peterson KE, Gortmaker SL: Relation between consumption of sugar-sweetened drinks and childhood obesity: a prospective, observational analysis. Lancet. 2001, 357 (9255): 505-508. 10.1016/S0140-6736(00)04041-1.
Welsh JA, Cogswell ME, Rogers S, Rockett H, Mei Z, Grummer-Strawn LM: Overweight among low-income preschool children associated with the consumption of sweet drinks: Missouri, 1999-2002. Pediatrics. 2005, 115 (2): e223-9. 10.1542/peds.2004-1148.
James J, Thomas P, Cavan D, Kerr D: Preventing childhood obesity by reducing consumption of carbonated drinks: cluster randomised controlled trial. BMJ. 2004, 328 (7450): 1237-10.1136/bmj.38077.458438.EE.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/8/279/prepub
Acknowledgements
The authors would like to thank the prefecture and municipality of Chania for their funding. They would also like to express their gratitude to the Chania General Hospital & Pediatric Clinic and especially Mr. Demetres Athanasopoulos and Mrs. Eua Mpalomenaki, the Medical-Social Center, the office of primary education of the prefecture of Chania end especially Mrs. Dora Niounaki, for their assistance. Special thanks go to Dr Caroline Codrington who reviewed and edited the manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
ML performed all statistical analysis and wrote the section of statistics. KS wrote the manuscript. MSP and MS performed the computing of data and did part of the bibliographic research, AK conceived of the study, is the head supervisor and reviewed the paper. All authors read and approved the final manuscript.
Manolis Linardakis, Katerina Sarri, Maria-Styliani Pateraki, Manolis Sbokos and Anthony Kafatos contributed equally to this work.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Linardakis, M., Sarri, K., Pateraki, MS. et al. Sugar-added beverages consumption among kindergarten children of Crete: effects on nutritional status and risk of obesity. BMC Public Health 8, 279 (2008). https://doi.org/10.1186/1471-2458-8-279
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2458-8-279