
Abstract
Long intergenic noncoding RNAs (lincRNAs) are a class of independently transcribed molecules longer than 200 nucleotides that do not overlap known protein-coding genes. LincRNAs have diverse roles in gene expression and participate in a spectrum of biological processes. Dysregulation of lincRNA expression can abrogate cellular homeostasis, cell differentiation, and development and can also deregulate the immune and nervous systems. A growing body of literature indicates their important and multifaceted roles in the pathogenesis of several different diseases. Furthermore, certain lincRNAs can be considered potential therapeutic targets and valuable diagnostic or prognostic biomarkers capable of predicting the onset of a disease, its degree of activity, or the progression phase. In this review, we discuss possible mechanisms and molecular functions of lincRNAs in the pathogenesis of selected autoimmune and neurodegenerative disorders: multiple sclerosis, rheumatoid arthritis, systemic lupus erythematosus, Sjögren’s syndrome, Huntington’s disease, Parkinson’s disease, Alzheimer’s disease, and amyotrophic lateral sclerosis. This summary can provide new ideas for future research, diagnosis, and treatment of these highly prevalent and devastating diseases.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Only 2–3% of the mammalian genome is transcribed into protein-coding mRNAs, and ~ 80% of the human genome exhibits some type of biochemical activity, such as RNA transcription, binding of transcription factors, or chromatin structure and histone modifications, in at least one cell type. Transcripts derived from these noncoding regions do not possess any protein-coding capacity and are annotated as noncoding RNAs (ncRNAs) [1]. Noncoding transcripts longer than 200 nucleotides are called long noncoding RNAs (lncRNAs). Long intergenic noncoding RNAs (lincRNAs) account for almost half of lncRNAs, and their genes are located from several bases to more than 3 Mb away from the nearest protein-coding gene. Similar to mRNAs, they are transcribed by RNAP2 (RNA polymerase II) and can be spliced, capped, and polyadenylated. However, in comparison to mRNAs, lincRNAs are expressed at a tenfold lower level, enriched in the nucleus, and mainly expressed in a cell type-specific, tissue-specific, developmental stage-specific, or disease state-specific manner, with overrepresentation in the brain and testis [2]. In humans, lincRNAs have diverse roles in gene expression and participate in a spectrum of biological processes. Within the nucleus, lincRNAs occupy the chromatin fraction and are involved in epigenetic regulation. They can affect transcription by recruiting chromatin remodeling complexes and forming R-loop structures at promoter regions. They can act as decoys to sequester transcription factors from their genomic targets or as scaffolds to enable the formation of multiprotein complexes and the recruitment of RNAP2. LincRNA loci can function in trans, producing lincRNA transcripts that function at locations genetically unlinked and spatially distant from their site of production. Other lincRNA loci regulate gene expression in cis, exhibiting transcriptional enhancer-like activity toward neighboring genes. Within the cytoplasm, they play a role in the modulation of mRNA stability, translation, and posttranslational modifications, as well as the regulation of their RNA interacting partners, e.g., miRNAs [2,3,4,5,6,7].
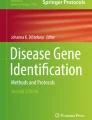
Dysregulation of lincRNA expression can abrogate cellular homeostasis, cell differentiation, and development and can also deregulate the immune and nervous systems. Therefore, overexpression, deficiency, or mutation of lincRNA genes has been implicated in genetically inherited disorders and tumorigenic mechanisms, including cell proliferation, migration and invasion, epithelial-to-mesenchymal transition, apoptosis, and cancer metastasis. Considering their involvement in pathological responses, lincRNAs have often been identified to act as miRNA sponges and thereby modulate the expression of both miRNAs and their targets (Fig. 1, Table S1). LincRNAs are strongly related to the progression of various disorders, with examples of individual lincRNAs involved in several different diseases (Fig. 2, Table 1, Table 2). In contrast, the level of a single lincRNA in one disease can vary depending on the type of sample analyzed (Table 1, Table 2). Certain lincRNAs can be considered potential therapeutic targets and valuable biomarkers capable of predicting the onset of a disease, its degree of activity, or the progression phase [2, 3, 5, 6].

LincRNAs acting as miRNA sponges in the pathogenesis of autoimmune and neurodegenerative diseases. Colors refer to the lincRNA/miRNA axes related to a particular disease. Repeating miRNAs are underlined

Network of lincRNAs and autoimmune and neurodegenerative diseases. Only lincRNAs involved in more than one disease were considered. Cellular pathways contributing to pathogenesis were shown
Knowledge about lincRNAs implicated in human disorders is increasing daily. LincRNAs can play both detrimental and protective pathophysiological roles. This dual nature can be manifested in their ability to directly or indirectly regulate cellular signal transduction pathways and mechanisms that govern basic cellular processes. In this review, we shed light on the implications of lincRNAs in selected autoimmune and neurodegenerative diseases. First, we focus on individual autoimmune and neurodegenerative disorders and exemplify differentially expressed lincRNAs, elucidating their impact on disease pathomechanisms (Table 1). Next, we summarize the activity of lincRNAs that are involved in multiply of these diseases, such as NEAT1, MALAT1, TUG1, MEG3, and XIST (Table 2).
Autoimmune Disorders
Autoimmune disorders are a group of heterogeneous diseases characterized by inappropriate immune responses to “self” antigens. Consequently, the immune system attacks normal molecules and healthy cells and tissues, causing damage to various organs and systems. LincRNAs may play a crucial role in the pathogenesis of these disorders, as they are important regulators of immune cell differentiation and activation in both the innate and adaptive immune systems. In this chapter, the involvement of lincRNAs in the pathogenesis of multiple sclerosis, systemic lupus erythematosus, rheumatoid arthritis, and Sjögren’s syndrome is described.
Multiple Sclerosis (MS)
MS is a chronic autoimmune inflammatory neurological disease of the CNS (central nervous system) that leads to sustained disability. The pathogenesis of MS involves genetic susceptibility and environmental factors. The progressive neurodegenerative process includes demyelination, chronic oxidative injury, and eventual axonal neuronal death in the spinal cord, optic nerves, and brain. The adaptive immune system is hyperactivated in the CNS and responsible for the destructive effects of MS. This hyperactivation includes the spontaneous activation of autoreactive proinflammatory T cells, CD4 + Th1 (T helper 1), and Th17 cells, resulting in the secretion of cytokines and stimulation of the inflammatory cascade. In the advanced stages of the disease, the role of B cells in driving inflammation appears to be prominent. Clinically, different MS subtypes have been described: relapsing remitting (RR), secondary progressive (SP), and primary progressive (PP). The pathophysiological mechanisms are associated with genes that play a regulatory role in the immune system [8].
To search for lincRNAs as biomarkers, in 2016, Santoro et al. screened 84 lncRNAs involved in autoimmunity and the human inflammatory response in serum from 12 patients with RRMS and 12 healthy controls and found lincRNAs that were upregulated in patients with RRMS and could play a role in neurodegenerative processes of MS, among others RN7SK RNA (the 7SK small nuclear RNA). RN7SK RNA is a part of the 7SK snRNP complex and represses the cellular kinase complex P-TEFb (positive transcription elongation factor b), which regulates the activity of CD4 + T lymphocytes. Upregulation of RN7SK RNA leads to disruption of CD4 + T cell differentiation and contributes to inflammation and activation of the autoimmune process [9]. Similarly, upregulation of LINC00293 and RP11-29G8.3 was reported in serum obtained from 16 SPMS and 12 PPMS Italian patients compared to 8 healthy controls [10]. Next, by in silico prediction, the authors identified the possible interactions of these lincRNAs with miRNAs and their putative targets possibly involved in MS. Among these interactions, miR-200a, miR-141, miR-24-3p, miR-15a, and miR-15b can be sequestered by RP11-29G8.3 (Table S1). Consequently, the levels of these miRNAs were decreased in blood samples from MS patients, causing the induction of their targets involved in the inflammatory response [10].
The lincRNA lnc-DC was also upregulated in serum obtained from 45 RRMS patients compared to 45 controls [11]. The lincRNA lnc‑DC is exclusively expressed in human DCs (dendritic cells) and is involved in their differentiation and maturation. In the cytoplasm, lnc‑DC directly binds to STAT3 (signal transducer and activator of transcription 3) and promotes its phosphorylation on tyrosine 705 [12]. Transcription factor STAT3 regulates many immune-associated genes and plays a role in Th17 cell differentiation. Lnc-DC overexpression could induce the overmaturation of dendritic cells via STAT3. These activated cells further migrate across the blood–brain barrier and stimulate the differentiation of memory T cells into proinflammatory Th1 and Th17 lymphocytes. In addition, macrophages and microglial cells are activated and produce other proinflammatory cytokines, oxygen radicals, and nitric oxide radicals responsible for demyelination and axonal loss [12]. Recently, a higher lnc-DC expression was confirmed in the PBMCs (peripheral blood mononuclear cells) of 50 female patients who were negative for the HLA-DRB1*15:01 allele, suggesting that lnc-DC expression is sex-specific among multiple sclerosis patients [13]. LincRNA expression regulation in MS by sex-determined factors and hormones was further suggested in case of PANDA (P21-associated ncRNA DNA damage activated). Overexpression of PANDA was observed in PB (peripheral blood) samples from 50 patients with RRMS compared to 50 healthy controls, with more prominent overexpression in male patients [14]. PANDA has an antiapoptotic effect and stabilizes the p53 protein after DNA damage induction [15].
By microarray analysis of PBMCs from 6 patients with RRMS compared to 5 healthy controls, scientists identified increased expression of linc-MAF-4 and correlated its level with the annual relapse rate in MS patients [16]. Linc-MAF-4 negatively regulates the transcription of MAF (V-maf musculoaponeurotic fibrosarcoma oncogene homolog), a Th2-associated transcription factor, by recruiting chromatin modifiers to sites within the genomic region of MAF. Downregulation of MAF leads to inhibition of T cell differentiation into Th2 cells. Linc-MAF-4 also promotes the activation of CD4 + helper T lymphocytes from patients with MS [16, 17].
Instead, by comparing PBMCs from 50 patients with RRMS with those from 25 healthy controls, Ghoveud et al. found downregulation of a memory B cell lineage-specific lincRNA, AL928742.12. Its level correlated with the depletion of its cis-regulated target, IGHA2 (immunoglobulin heavy constant alpha 2). IGHA2 encodes the constant region of heavy immunoglobulin chains and is involved in the differentiation of B lymphocytes during the humoral immune response [18]. Similarly, downregulation of the lincRNAs MEG9 (maternally expressed 9), HULC (hepatocellular carcinoma upregulated long noncoding RNA), and MIAT (myocardial infarction associated transcript, also called GOMAFU) was reported by Fenoglio et al. who studied PBMC samples from 27 patients with RRMS, 13 patients with PPMS, and 31 healthy controls in the Italian population [19]. MIAT can bind to the splicing factor SF1 (splicing factor 1), inhibiting splicing by preventing the formation of spliceosome complexes [20]. MIAT is expressed predominantly in the CNS, where it regulates the differentiation of neural stem cells into oligodendrocytes [21].
Another study carried out in circulating blood cells from 50 Iranian patients with RRMS, and 50 healthy controls showed downregulation of PVT1 (plasmacytoma variant translocation 1) with a moderate correlation between the level of expression of PVT1 and the duration of the disorder and no significant correlation with either the EDSS (expanded disability status scale) score or age at onset [22]. There are some features that put PVT1 in an interaction network with a major role in the pathogenesis of MS: (i) The PVT1 gene is located in a genomic region (8q24) that is a preferred site for chromosomal rearrangements in cancers and contains multiple risk loci for different diseases, including MS; (ii) PVT1 controls the release of IL-6 (interleukin 6); (iii) PVT1 functions as a molecular sponge for mir-200 family members, including miR-200a, which mediates the pathogenesis of MS through promoting the differentiation of Th17 cells and preventing the differentiation of Treg (regulatory T cells) cells (Table S1); and (iv) the main target of PVT1 is the MYC transcription factor, which is required for Th17 differentiation [22].
Two lincRNAs, LincR-Gng2-5’AS (transcribed in Th1 cells by the transcription factor STAT4) and LincR-Epas1-3’AS (transcribed in Th2 cells by STAT6), are located in genomic regions rich in genes encoding proteins that regulate the expression of cytokines and various immune factors [23]. A study conducted on serum from 42 RRMS and 18 SPMS Egyptian patients compared to 60 healthy controls showed upregulation of LincR-Gng2-5′AS in Th1 cells and downregulation of LincR-Epas1-3′AS in Th2 cells. This deregulation was more marked in patients with SPMS, and these two lincRNAs showed opposite correlations with the EDSS score (positive for LincR-Gng2-5′AS and negative for LincR-Epas1-3′AS) [24]. Changes in the expression of these two lincRNAs may play a role in the pathogenesis of MS for two reasons: (i) Both lincRNAs can regulate the expression of nearby genes that encode various immune regulators, and (ii) increased proinflammatory activity of Th1 cells and decreased anti-inflammatory activity of Th2 cells, which is correlated with the levels of both lincRNAs, have been observed in multiple sclerosis [23, 24].
Rheumatoid Arthritis (RA)
RA is characterized by chronic inflammation, and destruction of synovial joints and is caused primarily by the release of inflammatory cytokines, including TNF-α (tumor necrosis factor α), IL-1β, and IL-6. The major cellular contributors in RA are T and B lymphocytes, neutrophils, macrophages, and proliferating FLSs (fibroblast-like synoviocytes). The pathological changes include immune cell-mediated cartilage and subchondral bone damage, which can lead to joint deformities. FLSs play a critical role in the initiation of RA. Their abnormal activation, apoptosis resistance, and tumor-like transformation have been regarded as key steps in joint destruction [25].
Microarray analysis of lncRNAs in PBMCs and serum exosomes from 28 RA patients compared to healthy controls revealed lincRNA MEG9 that was significantly upregulated in both kinds of RA samples, whereas a decreased level of the lincRNA Jpx was observed in PBMC samples [26]. The lincRNA Jpx is known as a molecular switch for X-chromosome inactivation but also functions as an oncogene in cancer cells, inducing cell proliferation and cell migration [27]. In another study, Spurlock et al. detected a decreased level of lincRNA-p21 and an increased level of phosphorylated p65, a marker of activation of the proinflammatory transcription factor NF-κB (nuclear factor-kappa B), in the PBMC samples from 8 patients with RA compared to 9 healthy individuals. Interestingly, lincRNA‑p21 expression was induced in patients with RA treated with methotrexate, and this effect was further confirmed in cultured cells. LincRNA‑p21 binds to its target mRNAs and represses their translation by recruiting the translational repressor DDX6 (DEAD box protein 6). It potentially also represses proteins critical for NF‑κB transcriptional activity; therefore, lincRNA-p21 reduction may contribute to inflammation [28].
Analysis of synovial specimens (macrophages and fibroblasts) isolated from 26 patients with RA, 25 patients with osteoarthritis, and 2 patients with reactive arthritis compared with 15 control samples showed significant overexpression of the lincRNA H19 in the RA samples and osteoarthritis samples [29]. H19 RNA is abundantly expressed in endodermal and mesodermal-derived embryonic tissue, and after birth, its expression is repressed in all tissues except skeletal muscle. However, reexpression of H19 was observed in several different tumors; therefore, H19 RNA has been proposed as a marker of embryonal dedifferentiation of adult tissues and as a tumor marker. H19 upregulation mimics inflammatory/oxidative stress. Among the H19-regulated targets, genes encoding pathological stress factors, such as thioredoxin, MKK1 (MAP-kinase kinase 1), NF-κB, JNK2, TNF-α, and IL-6, have been identified, and these factors may contribute to inflammation in RA. Therefore, H19 upregulation mimics inflammatory and oxidative stress and/or dedifferentiation of adult synovial tissues, which could underlie the pathogenesis of RA [29].
Microarray analysis of 3 samples of FLSs from both healthy controls and patients with RA revealed significant downregulation of the lincRNA LERFS (lowly expressed in RA FLSs) in RA FLSs (FLSs isolated from RA patients). In vitro experiments in cultured FLSs and further in vivo experiments using mouse models showed that LERFS negatively regulates RA FLS migration, invasion, and proliferation through interaction with hnRNPQ (heterogeneous nuclear ribonucleoprotein Q) and that this LERFS-hnRNPQ complex controls mRNA metabolism and cell motility by modulating the stability or translation of the RhoA, Rac1, and CDC42 mRNAs [38]. The Wnt signaling pathway is also targeted by the lincRNA UCA1 (urothelial cancer associated 1). In RA FLSs, the level of UCA1 was decreased, which increased RA FLS viability via decreased expression of Caspase-3 and inhibition of apoptosis. Moreover, scientists have found an inverse correlation between the levels of UCA1 and Wnt6, which induces the Wnt signaling pathway in RA FLSs and thus promotes RA progression [39].
Zhang et al. established rat models of RA to determine the mechanisms of inflammation and apoptosis in synovial tissues and FLSs. They reported high expression of the lincRNA PVT1 and low expression of its target, SIRT6 (Sirtuin 6), in both tissues and FLSs of RA. PVT1 binds to the SIRT6 promoter to induce its methylation, which in turn inhibits SIRT6 transcription. SIRTs are regulators of many processes, including cell survival, gene transcription, and inflammation. Therefore, decreased SIRT6 activity in RA FLSs is thought to induce cell proliferation and inflammation and suppress apoptosis [40]. Recently, increased PVT1 expression was confirmed in STs from 30 patients with RA. Concurrently, the level of its target, miR-145-5p, was significantly decreased, resulting in enhanced cell proliferation and increased secretion of IL‐1β and IL‐6 in RA cells (Table S1) [41]. Higher expression of LINK-A was also recently observed in STs and FLSs from 5 patients with RA compared with 5 healthy controls and was positively correlated with the severity of synovitis in the patients. LINK-A was shown to regulate inflammation and invasion through the HIF-1α signaling pathway, inducing the expression and secretion of matrix metalloproteinases and proinflammatory cytokines, such as IL-1β, IL-6, and IL-8. LINK-A knockdown decreased the migration and invasion of RA FLSs [42].
Systemic Lupus Erythematosus (SLE)
SLE is a chronic systemic autoimmune disease with a high incidence in women of childbearing age. SLE is characterized by loss of immunological tolerance to self-nuclear antigens, production of multiple autoantibodies, excessive proinflammatory cytokine and chemokine production, and, ultimately, damage to tissues or organs, most commonly the skin, kidney, lung, nervous system, and circulatory system. Disruption of monocytes initiates the autoreactive cascade in SLE. Moreover, T cells, B cells, and dendritic cells are crucial cells for SLE pathogenesis. LN (lupus nephritis) is one of the most serious complications of SLE and one of the leading causes of morbidity and mortality in patients [43].
Wu et al. showed that the expression of linc0949 and linc0597 was significantly decreased in PBMCs from 102 patients with SLE compared to 76 healthy donors [44]. Further analysis associated linc0949 with the incidence of LN and revealed a correlation between the linc0949 level and disease activity, as assessed by both the SLEDAI (SLE disease activity index) score and the level of complement component C3, in patients with SLE. Furthermore, linc0949 expression was found to be decreased in patients with SLE with ongoing or cumulative organ damage. In three patients with severe disease flares, linc0949 expression increased significantly after treatment with immunosuppressive agents, suggesting its responsiveness to therapy and making it a good candidate as a biomarker for diagnosing and for guiding SLE therapy [44]. In another study conducted in two independent cohorts, plasma from healthy controls and SLE patients divided into those with lupus nephritis and those with SLE without nephritis was analyzed. The results revealed that the level of linc0597 was increased in all patients with SLE [45], in contrast to observations in PBMCs [44]. Furthermore, the level of lnc-DC was significantly higher in the patients with LN compared to patients with SLE without nephritis but was significantly decreased in all SLE patients compared with healthy controls. Therefore, linc0597 has been suggested as a biomarker to identify patients with SLE, while lnc-DC could be used to discriminate LN from SLE without nephritis [45]. Wu et al. examined plasma samples from patients with SLE and healthy controls as well [46]. The levels of linc0597, lnc0640, and lnc5150 were elevated in SLE patients, whereas that of lnc7074 was decreased. Furthermore, they showed that the expression levels of lnc0640, lnc5150, lnc6655, and lnc7074 were significantly higher in patients with LN than in those without LN, as previously shown for linc0597 and lnc-DC [45]. Therefore, the plasma levels of these six lincRNAs may reflect the renal pathology of SLE. Moreover, comparison of lincRNA expression levels in plasma from 30 patients with rheumatoid arthritis and 31 patients with primary Sjögren’s syndrome with plasma from SLE patients indicated that the combination of lnc7074, linc0597, lnc0640, and lnc5150 could distinguish SLE from the other two diseases. KEGG pathway analysis revealed that lnc0640 and lnc5150 may participate in the development of SLE through the MAPK (mitogen-activated protein kinase) signaling pathway, which regulates the immune response of T and B cells as well as the production of multiple SLE-related inflammatory factors, such as TNF-α, IL-1/6, and IFN. In addition, lnc0640, lnc6655, and lnc7074 could regulate the expression of their predicted target genes by acting as ceRNAs (competing endogenous RNAs) for the target miRNAs [46].
RNA-seq of renal biopsy samples from 22 patients with LN and 7 controls revealed an elevated level of the lincRNA RP11-2B6.2, with higher expression in LN patients with active lesions than in those with chronic lesions. RP11-2B6.2 has been shown to function as a positive regulator of the IFN-I (type I interferon) signaling pathway through epigenetic inhibition of its negative regulator, the SOCS1 (suppressor of cytokine signaling 1) gene. RP11-2B6.2 overactivates the IFN-I pathway, which in turn results in activated phosphorylation of JAK1 (Janus kinase 1), TYK2 (tyrosine kinase 2), and STAT1 [47]. The IFN-I signaling pathway is a crucial component of the innate and adaptive immune responses. Interferons exhibit antiviral activity as well as growth inhibitory and immunomodulatory effects by modulating the expression of ISGs (IFN-stimulated genes) [48, 49]. Type I IFNs are considered to play a pathogenic role in autoimmune diseases [50].
Recently, global comprehensive analyses using microarrays or high-throughput RNA sequencing have been performed, providing a new direction for the diagnosis and treatment of SLE by suggesting lincRNAs that might serve as biomarkers. In 2019, Ye et al. performed RNA-seq of PBMCs from 147 individuals with SLE and 117 healthy donors and identified 23 lincRNAs that were differentially expressed and may be related to SLE. They constructed a coexpression network between the lincRNAs and their predicted target genes, which further allowed verification of the possible biological functions of these 23 lincRNAs in metabolism, cellular signal transduction, the cell cycle, apoptosis, cell adhesion, or antigen presentation [51]. In another study, moDCs (monocyte-derived dendritic cells) from 15 female SLE patients were compared with those from 15 female healthy controls. A total of 150 differentially expressed lincRNAs were identified, for example, the highly upregulated lincRNA TSIX (XIST antisense transcript). Its expression was positively correlated with the SLEDAI score. Upregulated TSIX facilitates X chromosome inactivation by protecting the active X from ectopic silencing, consistent with the increased incidence and prevalence of SLE in women [52].
Among the accumulating recent reports, the implication of the lincRNAs H19 and MIAT in SLE was discovered, which both have been already connected to immunological disorders, RA and MS, respectively [19, 29]. In SLE, upregulation of H19 and MIAT induces dysregulation of the immune system by inhibiting IL-2 production and of the complement system by sponging miRNAs, respectively (Table S1) [53, 68]. Global ChIP-seq analysis identified HAR1 as a REST target and, consistent with this finding, showed that both HAR1F and HAR1R are significantly downregulated in the striatum of HD patients [69]. However, the role of these lincRNAs in neurodegenerative diseases is still obscure.
TUNA (Tcl1 upstream neuron-associated lncRNA) exhibits CNS-specific expression in vertebrates. This lincRNA forms a complex with RNA-binding proteins that is enriched at the promoters of the Sox2, Nanog, and Fgf4 genes. Functional studies performed on mouse embryonic stem cells revealed its essential roles in pluripotency and neural differentiation. Global transcriptome analysis of genes affected by TUNA knockdown showed extensive dysregulation of genes associated with neurodegenerative diseases. Via microarray gene expression profiling of 4 brain regions in 44 HD patients and 36 healthy individuals, the authors demonstrated that TUNA expression is decreased in HD cells and inversely correlated with pathological disease severity. Interestingly, this effect was observed only in the striatum (exhibiting high expression of TUNA and Sox2 in healthy brains), whereas TUNA expression in the motor cortex, prefrontal association cortex, and cerebellum was comparable between HD patients and controls [71].
High-throughput transcriptome profiling of 20 postmortem human HD brains and 49 control brains revealed that 6.8% of the differentially expressed genes were lincRNAs [72]. Reanalysis of microarray data from HD and healthy brains identified two lincRNAs with deregulated expression in HD with a currently unknown role in the etiology of the disease. LINC00341, expressed mainly in adipose tissue, was upregulated, while brain-specific LINC00342 showed downregulation in HD caudates [69]. In addition, using an RNA-seq approach, Colpo et al. identified LINC02470 to be downregulated in peripheral blood samples collected from 16 patients with a genetic diagnosis of HD in comparison to 8 healthy individuals [73].
Parkinson’s Disease (PD)
PD is a progressive neurodegenerative disorder that affects approximately 2–3% of elderly people. The underlying pathology involves the selective loss of dopaminergic neurons in the SN (substantia nigra) of the brain and the intracellular aggregation of α-synuclein (α-syn) in Lewy bodies, leading to motor dysfunction and cognitive decline. The vast majority of PD cases are sporadic, with both genetic and environmental factors playing a role. Only approximately 10% are familial, arising through mutations in mitochondria-associated genes, including SNCA (α-synuclein), LRRK2 (leucine-rich repeat kinase 2), Parkin (PARK2), PINK1 (phosphatase and tensin homolog induced putative kinase 1), PARK7 (protein deglycase DJ-1), and ATP13A2 (ATPase type 13A), pointing to the important role of mitochondrial dysfunction in the pathogenesis of PD [74]. LincRNAs are involved in different pathological pathways and mechanisms of PD, such as α-syn proteostasis, mitochondrial dysfunction, oxidative stress, apoptosis, and neuroinflammation.
Expression profiling of 20 PD brains and 10 control brains revealed the essential upregulation of lincRNA-p21 in PD [75]. Furthermore, Ding et al. reported an elevated level of lincRNA-p21 in SH-SY5Y cells treated with MPP+ (1-methyl-4-phenylpyridinium) to establish an in vitro model of PD. The high level of lincRNA-p21 resulted in decreased cell viability and increased cytotoxicity, apoptosis, oxidative stress, and neuroinflammation. Further research revealed a new lncRNA-miRNA-mRNA regulatory network in PD with lincRNA-p21 acting as a miR-625 sponge and thus indirectly derepressing the gene encoding the Ca2+ channel TRPM2 (Table S1). Activation of TRPM2 leads to cytotoxic influx of Ca2+ and, in turn, neuronal death [76]. Additionally, by functioning as a miR-1277-5p sponge, lincRNA-p21 positively regulates the expression of the miR-1277-5p target α-syn (Table S1) [77]. Another study revealed the role of lincRNA-p21 in sustained neuroinflammation mediated by excessive activation of microglia, which is one of the essential initiating factors in the onset and progression of PD. LincRNA-p21 promotes LPS (lipopolysaccharide)-induced microglial activation via a p53-dependent pathway by regulating the miR-181 family/PKC-δ (protein kinase C-delta) axis (Table S1) [78]. Recently, it was shown that upregulation of lincRNA-p21 regulates the degradation of TGIF1 (TG-interacting factor 1) through the (STAU1)-mediated mRNA decay (SMD) pathway in a cellular model of PD. TGIF1 was identified as a transcriptional regulator of α-syn in PD [79].
In turn, the lincRNA H19 has been reported to be downregulated in PD mice and in cellular models [98].
Upregulation of NEAT1, and further for IL-8, was confirmed in serum from RRMS and SPMS patients as well as in astrocytes, microglia, and neurons from human brains affected by MS [9, 99, 100]. NEAT1 has also been reported to stimulate the secretion of several chemokines and interleukins, which in turn affect monocyte-macrophage functions and T cell differentiation [101]. In another study, overexpression of NEAT1 in peripheral blood samples from patients with RRMS was shown to be inversely correlated with age at the time of MS onset and with the duration of MS disease in female patients, suggesting that the expression of lincRNAs can be regulated by sex-determined factors, hormones, and drugs [14]. Like in MS, microarray analysis of lncRNAs revealed NEAT1 that was significantly upregulated in PBMCs and serum exosomes from patients with rheumatoid arthritis [26]. In study performed on serum exosomes, Liu et al. explained the role of upregulated NEAT1 in the promotion of RA progression through regulation of the miR-144-3p/ROCK2/Wnt/β-catenin axis (Table S1). Serum-derived exosomes from RA patients promoted the proliferation, migration, and differentiation of CD4 + T cells into Th17 cells while inhibiting their apoptosis. NEAT1 acts as a molecular sponge of miR-144-3p and in turn promotes the expression of the miR-144-3p target ROCK2 (Rho-associated protein kinase 2). ROCK2 is involved in immune defenses and inflammation by activating the Wnt/β-catenin pathway, which plays a crucial role in inflammation in RA. Further experiments, including studies in a mouse model of RA, demonstrated that knocking down NEAT1 significantly alleviated the clinical symptoms [102]. NEAT1 expression was also found to be upregulated in STs from patients with RA [149].
In consistence, in patients with Huntington’s disease, TUG1 expression was found to be upregulated, potentially in response to p53 activation, which has also been reported in HD [69, 149]. Elevated levels of TUG1 were also detected in the serum of PD patients as well as in mouse and cellular models of PD [150, 151]. Loss-of-function studies revealed that TUG1 can promote apoptosis, oxidative stress, neuroinflammation, and pathological damage. Moreover, TUG1 was shown to interact with miR-152-3p and regulate its level, consistent with the decreased expression of this miRNA in PD models. MiR-152-3p regulates the expression of the proapoptotic phosphatase PTEN (phosphatase and tensin homolog), which was found to be upregulated in both cellular and mouse models of PD (Table S1) [151] and has already been linked to neurodegenerative processes in PD [152]. In addition, TUG1 was reported to be significantly upregulated in cellular and mouse models of Alzheimer’s disease, and further studies correlated elevated TUG1 levels with worsened memory and spatial learning abilities, increased pathological injury and apoptosis, and decreased antioxidant capacity of hippocampal neurons in AD mice [153]. Furthermore, TUG1 was found to act as a sponge for miR-15a, which targets ROCK1 mRNA, encoding a protein involved in the production of Aβ (Table S1). In line with that finding, the authors reported an elevated level of ROCK1 and a decreased level of miR-15a in AD mice and Aβ25-35-treated hippocampal neurons [153].
TUG1 level is also significantly upregulated in rheumatoid arthritis, as has been revealed by microarray analysis of lncRNAs in PBMCs and serum exosomes from patients [26]. Higher TUG1 expression was next confirmed in cultured primary normal human FLSs and RA FLSs and was linked to increased invasion, migration, and glucose metabolism and decreased apoptosis in RA. Furthermore, scientists have described the TUG1/miR-34a-5p/LDHA (lactate dehydrogenase A) axis, via which RA FLSs, which display an increased glucose consumption rate, can upregulate glucose metabolism due to increased expression of the glucose metabolism enzyme LDHA (Table S1) [154]. Likewise, TUG1 level was found to be upregulated in serum and peripheral blood obtained from patients with different subtypes of multiple sclerosis [9, 10, 14]. By further in silico prediction, TUG1 has been supposed to bind miR-20a-5p, which level was decreased in blood samples from MS patients resulting in the induction of inflammatory response (Table S1) [10]. Similar to NEAT1, the overexpression of TUG1 detected in peripheral blood samples was inversely correlated with age at the time of MS onset and with the duration of MS disease in female patients [14]. Intriguingly, studying PBMCs samples from 27 patients with RRMS, 13 patients with PPMS, and 31 healthy controls in the Italian population, Fenoglio et al. showed downregulation of TUG1 and identified a correlation between the TUG1 level and the EDSS score of the disease [19]. The decreased expression of TUG1 was further confirmed in samples from a Belgian cohort composed of 17 RRMS and 7 PPMS patients and 23 healthy controls [19]. The discrepancy between these studies and the findings in previous reports [9, 14] is explained by the different biological samples used for analysis, the different phases of the disease, and the pharmacological treatments administered. TUG1 expression was also found to be markedly lower in PBMCs from systemic lupus erythematosus patients and to be further decreased in SLE patients with LN, with the lower expression in monocytes than in either T or B cells. The decreased level of TUG1 was negatively correlated with the SLEDAI score, ESR (erythrocyte sedimentation rate), and disease duration, and was further suggested to be correlated with deregulation of the NF-κB signaling pathway, which ultimately leads to the development of SLE [155].
MEG3
MEG3 is an imprinted gene located in the DLK1-MEG3 locus present on chromosome 14q32.3 in humans, which encodes an alternatively spliced long noncoding RNA of ~ 1.7 kb that functions as tumor suppressor; its expression is lost in various human cancer cell lines [156]. In human body, MEG3 is expressed in several tissues, with the highest expression levels in the pituitary gland and different regions of the human brain. It has been documented that decreased level of MEG3 underlies the pathomechanism of several immunological and neurodegenerative diseases. MEG3 deregulation has previously been reported to occur during the development of CD4 + T cells in immune thrombocytopenic purpura, resulting in an immune imbalance of Treg and Th17 cells [157]. MEG3 has also been shown to regulate ischemic neuronal death in cerebral ischemic stroke [157, 158].
In multiple sclerosis, analyses of blood samples from RRMS patients revealed downregulated expression of MEG3 as well, and its level was negatively correlated with the EDSS score and with the level of its putative target, NLRC5, which stimulates the production of inflammatory cytokines [32, 158]. Increased level of NLRC5 and reduced level of MEG3 were also reported in complete Freund’s adjuvant (CFA)-induced synovial tissues and in FLSs from a rat model of RA [33]. Like in case of lincRNA FER1L4, hypermethylation of the MEG3 promoter led to a reduced level of MEG3 in RA. Hypermethylation of both the FER1L4 and MEG3 promoters can be inhibited by the methylation inhibitor 5-azadC (5-aza-2-deoxycytidine). Thus, the expression of NLRC5 was found to be significantly decreased after 5-azadC treatment [31, 33].
MEG3 contains an NRSE upstream of its TSS (transcription start site) and concordantly was found to be downregulated in brain tissues of HD patients [69]. Opposite results have been obtained in cell and mouse models of HD, in which MEG3 expression was significantly increased. In this study, simultaneous knockdown of MEG3 and exogenous expression of N-terminal HTT with 83 glutamines resulted in reduced formation of mHTT aggregates and decreased expression of the p53 transcription factor, which is known to be bound and stabilized by MEG3 [110]. Moreover, the documented role of MEG3 as the PRC2 interactor and its functions in the cAMP-dependent signaling pathway and cell proliferation strongly support its involvement in the massive transcriptional abnormalities observed in HD [68]. MEG3 expression was also found to be decreased in the plasma of PD patients and in a cellular model, and this downregulation is related to the aggravation of nonmotor symptoms, cognitive decline, and PD stage [159]. Scientists have found that MEG3 can affect the expression of LRRK2 and that MEG3 overexpression increases viability and suppresses apoptosis in SH-SY5Y cells treated with MPP + [160]. Moreover, Yi et al. reported a decreased level of MEG3 in hippocampal tissues in a rat model of AD established by microinjection of Aβ25‐35 into the right ventricle. MEG3 was found to be capable of improving cognitive impairment, mitigating neuronal damage, decreasing the expression of Aβ25‐35, and suppressing astrocyte activation in hippocampal tissues through activation of the PI3K/AKT signaling pathway, which keeps the Tau protein in the hypophosphorylated state [161].
XIST
XIST (X-inactive specific transcript) is a 15–17 kb long capped, spliced, and polyadenylated lincRNA which is retained in the nucleus and plays a crucial role for X-chromosome inactivation in female placental mammals [162].
The level of XIST expression was found to be downregulated in PBMC of patients with RR and PP subtypes of multiple sclerosis [19]. In contrary, the expression of XIST in cartilage tissues collected from 39 patients with rheumatoid arthritis was found to be upregulated, similarly to the level of STAT3 but in opposite to the level of let-7c-5p. Let-7c-5c acts as a tumor suppressor in human cancers by affecting the proliferation and apoptosis of cancer cells and inhibiting STAT3 expression, which was previously shown to be associated with the proliferation and differentiation of osteoblasts in a rat model of RA. Further analysis of this study in the rat model revealed that XIST sponges let-7c-5p, thereby upregulating STAT3 (Table S1). Both silencing of XIST or upregulation of let-7c-5p promoted the expression of osteogenic genes, inhibited inflammatory responses in osteoblasts, elevated the type I collagen protein level, and reduced the degree of cartilage tissue damage in RA rats [163].
Also in neurodegenerative disorders, HD, PD, and AD, scientists found elevated level of XIST, both in mouse and cellular models [110, 164, 165]. Although the role of this lincRNA in HD pathogenesis is still unknown [110], in PD cells XIST was shown to upregulate Sp1 (synphilin-1) by sponging miR-199a-3p (Table S1). Sp1 positively modulates the transcription and translation of LRRK2. Elevated expression of Sp1 was found to contribute to inhibition of cell proliferation and enhancement of apoptosis and to increase disease severity in a mouse model of PD [164]. In case of AD, Yue et al. demonstrated that XIST expression was positively correlated with the expression of Aβ1–42 and BACE1 but negatively correlated with that of miR-124, which is a known BACE1 regulator. Further studies confirmed that XIST exhibits a stimulatory effect on cell damage by regulating the miR‐124/BACE1 axis (Table S1) [165]. Increased expression of XIST was also confirmed in hippocampal neurons treated with Aβ25-35. In these cells, XIST was found to enhance Aβ25-35-induced toxicity, oxidative stress, and apoptosis by binding and downregulating the expression of neuroprotective miR-132, which has already been reported to be downregulated in human AD brains and involved in AD pathogenesis (Table S1) [166].
Conclusions
The last decade has resulted in an extensive body of literature concerning lincRNAs and their roles in the pathogenesis of human diseases. Whenever possible, studies were carried out on samples derived from patients compared to healthy controls matched for age and sex. These studies identified altered expression of lincRNAs that were further linked to disrupted molecular pathways and affected the expression of proteins with important biological functions. However, the consequences were not always clear. In fact, some important issues remain to be considered, such as the number of samples used for lincRNA analysis, which was sometimes limited, and the observation that the expression levels of lincRNAs are influenced by several factors. Therefore, the biological sample chosen for the analysis, the pharmacological treatment, the stage of the disease, and the age and sex of the patients can result in different observations, as seen for the TUG1 level in MS, which was found to be high in serum and PB but low in PBMC, and for LINC00507, which exhibited decreased expression in AD brains but an increased abundance in mouse and cellular models of AD (Table 1). Despite these inconsistencies, lincRNAs are undoubtedly important regulators of the differentiation and activation of nervous and immune cells, and their manipulation could have a beneficial therapeutic effect in human diseases. Additionally, due to their differential expression in a particular disease, lincRNAs can serve as valuable biomarkers for diagnosis and monitoring disease progression. Since the function of many lincRNAs in human diseases remains unknown, additional research on lincRNAs is essential for a better understanding of autoimmune and neurodegenerative disorders. With knowledge of these functions and the molecular pathways involved, we can identify promising therapeutic targets and shed light on the treatment of these diseases.
Data Availability
No datasets were generated during the current study.
References
Wilusz JE, Sunwoo H, Spector DL (2009) Long noncoding RNAs: functional surprises from the RNA world. Genes Dev 23:1494–1504. https://doi.org/10.1101/gad.1800909
Ransohoff JD, Wei Y, Khavari PA (2018) The functions and unique features of long intergenic non-coding RNA. Nat Rev Mol Cell Biol 19:143–157. https://doi.org/10.1038/nrm.2017.104
Quinn JJ, Chang HY (2016) Unique features of long non-coding RNA biogenesis and function. Nat Rev Genet 17:47–62. https://doi.org/10.1038/nrg.2015.10
Dhanoa JK, Sethi RS, Verma R et al (2018) Long non-coding RNA: its evolutionary relics and biological implications in mammals: a review. J Anim Sci Technol 60:25. https://doi.org/10.1186/s40781-018-0183-7
Kazimierczyk M, Kasprowicz MK, Kasprzyk ME, Wrzesinski J (2020) Human long noncoding RNA interactome: detection, characterization and function. Int J Mol Sci 21:1027. https://doi.org/10.3390/ijms21031027
Statello L, Guo CJ, Chen LL, Huarte M (2021) Gene regulation by long non-coding RNAs and its biological functions. Nat Rev Mol Cell Biol 22:96–118. https://doi.org/10.1038/s41580-020-00315-9
Yao RW, Wang Y, Chen LL (2019) Cellular functions of long noncoding RNAs. Nat Cell Biol 21:542–551. https://doi.org/10.1038/s41556-019-0311-8
Thompson AJ, Baranzini SE, Geurts J et al (2018) Multiple sclerosis. Lancet 391:1622–1636. https://doi.org/10.1016/S0140-6736(18)30481-1
Santoro M, Nociti V, Lucchini M et al (2016) Expression profile of long non-coding RNAs in serum of patients with multiple sclerosis. J Mol Neurosci 59:18–23. https://doi.org/10.1007/s12031-016-0741-8
Santoro M, Nociti V, Lucchini M et al (2020) A pilot study of lncRNAs expression profile in serum of progressive multiple sclerosis patients. Eur Rev Med Pharmacol Sci 24:3267–3273. https://doi.org/10.26355/eurrev_202003_20694
Shaker OG, Mahmoud RH, Abdelaleem OO et al (2019) LncRNAs, MALAT1 and lnc-DC as potential biomarkers for multiple sclerosis diagnosis. Biosci Rep 39:SR20181335. https://doi.org/10.1042/BSR20181335
Wang P, Xue Y, Han Y et al (2014) The STAT3-binding long noncoding RNA lnc-DC controls human dendritic cell differentiation. Science 344:310–313. https://doi.org/10.1126/science.1251456
Bahrami T, Taheri M, Javadi S et al (2021) Expression analysis of long non-coding RNA Lnc-DC in HLA-DRB1*15:01-negative patients with multiple sclerosis: a probable cause for gender differences in multiple sclerosis susceptibility? J Mol Neurosci 71:821–825. https://doi.org/10.1007/s12031-020-01704-7
Dastmalchi R, Ghafouri-Fard S, Omrani MD et al (2018) Dysregulation of long non-coding RNA profile in peripheral blood of multiple sclerosis patients. Mult Scler Relat Disord 25:219–226. https://doi.org/10.1016/j.msard.2018.07.044
Kotake Y, Kitagawa K, Ohhata T et al (2016) Long non-coding RNA, PANDA, contributes to the stabilization of p53 tumor suppressor protein. Anticancer Res 36:1605–1611
Zhang F, Liu G, Wei C et al (2017) Linc-MAF-4 regulates Th1/Th2 differentiation and is associated with the pathogenesis of multiple sclerosis by targeting MAF. FASEB J 31:519–525. https://doi.org/10.1096/fj.201600838R
Ranzani V, Rossetti G, Panzeri I et al (2015) The long intergenic noncoding RNA landscape of human lymphocytes highlights the regulation of T cell differentiation by linc-MAF-4. Nat Immunol 16:318–325. https://doi.org/10.1038/ni.3093
Ghoveud E, Teimuri S, Vatandoost J et al (2020) Potential biomarker and therapeutic LncRNAs in multiple sclerosis through targeting memory B cells. Neuromolecular Med 22:111–120. https://doi.org/10.1007/s12017-019-08570-6
Fenoglio C, Oldoni E, Serpente M et al (2018) LncRNAs expression profile in peripheral blood mononuclear cells from multiple sclerosis patients. J Neuroimmunol 324:129–135. https://doi.org/10.1016/j.jneuroim.2018.08.008
Tsuiji H, Yoshimoto R, Hasegawa Y et al (2011) Competition between a noncoding exon and introns: Gomafu contains tandem UACUAAC repeats and associates with splicing factor-1. Genes Cells 16:479–490. https://doi.org/10.1111/j.1365-2443.2011.01502.x
Mercer TR, Qureshi IA, Gokhan S et al (2010) Long noncoding RNAs in neuronal-glial fate specification and oligodendrocyte lineage maturation. BMC Neurosci 11:14. https://doi.org/10.1186/1471-2202-11-14
Eftekharian MM, Ghafouri-Fard S, Soudyab M et al (2017) Expression analysis of long non-coding RNAs in the blood of multiple sclerosis patients. J Mol Neurosci 63:333–341. https://doi.org/10.1007/s12031-017-0982-1
Hu G, Tang Q, Sharma S et al (2013) Expression and regulation of intergenic long noncoding RNAs during T cell development and differentiation. Nat Immunol 14:1190–1198. https://doi.org/10.1038/ni.2712
Shaker OG, Golam RM, Ayoub S et al (2020) Correlation between LincR-Gng2-5’and LincR-Epas1-3’as with the severity of multiple sclerosis in Egyptian patients. Int J Neurosci 130:515–521. https://doi.org/10.1080/00207454.2019.1695610
Lin YJ, Anzaghe M, Schulke S (2020) Update on the pathomechanism, diagnosis, and treatment options for rheumatoid arthritis. Cells 9:880. https://doi.org/10.3390/cells9040880
Song J, Kim D, Han J et al (2015) PBMC and exosome-derived Hotair is a critical regulator and potent marker for rheumatoid arthritis. Clin Exp Med 15:121–126. https://doi.org/10.1007/s10238-013-0271-4
Tian D, Sun S, Lee JT (2010) The long noncoding RNA, Jpx, is a molecular switch for X chromosome inactivation. Cell 143:390–403. https://doi.org/10.1016/j.cell.2010.09.049
Spurlock CF 3rd, Tossberg JT, Matlock BK et al (2014) Methotrexate inhibits NF-kappaB activity via long intergenic (noncoding) RNA-p21 induction. Arthritis Rheumatol 66:2947–2957. https://doi.org/10.1002/art.38805
Stuhlmuller B, Kunisch E, Franz J et al (2003) Detection of oncofetal h19 RNA in rheumatoid arthritis synovial tissue. Am J Pathol 163:901–911. https://doi.org/10.1016/S0002-9440(10)63450-5
Zou Y, Xu S, **ao Y et al (2018) Long noncoding RNA LERFS negatively regulates rheumatoid synovial aggression and proliferation. J Clin Invest 128:4510–4524. https://doi.org/10.1172/JCI97965
Yu H, Ding C, Dai S et al (2020) Long noncoding RNA FER1L4 regulates rheumatoid arthritis via targeting NLRC5. Clin Exp Rheumatol 38:713–723
Torkamandi S, Bahrami S, Ghorashi T et al (2021) Dysregulation of long noncoding RNA MEG3 and NLRC5 expressions in patients with relapsing-remitting multiple sclerosis: is there any correlation? Genes Immun 22:322–326. https://doi.org/10.1038/s41435-021-00154-4
Liu YR, Yang L, Xu QQ et al (2019) Long noncoding RNA MEG3 regulates rheumatoid arthritis by targeting NLRC5. J Cell Physiol 234:14270–14284. https://doi.org/10.1002/jcp.28126
Mo BY, Guo XH, Yang MR et al (2018) Long non-coding RNA GAPLINC promotes tumor-like biologic behaviors of fibroblast-like synoviocytes as microrna sponging in rheumatoid arthritis patients. Front Immunol 9:702. https://doi.org/10.3389/fimmu.2018.00702
Bi X, Guo XH, Mo BY et al (2019) LncRNA PICSAR promotes cell proliferation, migration and invasion of fibroblast-like synoviocytes by sponging miRNA-4701-5p in rheumatoid arthritis. EBioMedicine 50:408–420. https://doi.org/10.1016/j.ebiom.2019.11.024
Wang W, Guo P, Chen M et al (2020) FOXM1/LINC00152 feedback loop regulates proliferation and apoptosis in rheumatoid arthritis fibroblast-like synoviocytes via Wnt/beta-catenin signaling pathway. Biosci Rep 40:BSR20191900. https://doi.org/10.1042/BSR20191900
Jridi I, Canté-Barrett K, Pike-Overzet K, Staal FJT (2020) Inflammation and Wnt Signaling: Target for Immunomodulatory Therapy? Front Cell Dev Biol 8:615131. https://doi.org/10.3389/FCELL.2020.615131
Ljungberg JK, Kling JC, Tran TT, Blumenthal A (2019) Functions of the WNT signaling network in sha** host responses to infection. Front Immunol 10:2521. https://doi.org/10.3389/FIMMU.2019.02521
Yan ZF, Zhao XY, Liu W, Liu XP (2018) UCA1 impacts progress of rheumatoid arthritis by inducing the apoptosis of fibroblast-like synoviocyte. Eur Rev Med Pharmacol Sci 22:914–920. https://doi.org/10.26355/eurrev_201802_14370
Zhang CW, Wu X, Liu D et al (2019) Long non-coding RNA PVT1 knockdown suppresses fibroblast-like synoviocyte inflammation and induces apoptosis in rheumatoid arthritis through demethylation of sirt6. J Biol Eng 13:60. https://doi.org/10.1186/s13036-019-0184-1
Tang J, Yi S, Liu Y (2020) Long non-coding RNA PVT1 can regulate the proliferation and inflammatory responses of rheumatoid arthritis fibroblast-like synoviocytes by targeting microRNA-145-5p. Hum Cell 33:1081–1090. https://doi.org/10.1007/s13577-020-00419-6
Wang J, Shen C, Li R et al (2021) Increased long noncoding RNA LINK-A contributes to rheumatoid synovial inflammation and aggression. JCI Insight 6:e146757. https://doi.org/10.1172/JCI.INSIGHT.146757
Fava A, Petri M (2019) Systemic lupus erythematosus: Diagnosis and clinical management. J Autoimmun 96:1–13. https://doi.org/10.1016/j.jaut.2018.11.001
Wu Y, Zhang F, Ma J et al (2015) Association of large intergenic noncoding RNA expression with disease activity and organ damage in systemic lupus erythematosus. Arthritis Res Ther 17:131. https://doi.org/10.1186/s13075-015-0632-3
Wu GC, Li J, Leng RX et al (2017) Identification of long non-coding RNAs GAS5, linc0597 and lnc-DC in plasma as novel biomarkers for systemic lupus erythematosus. Oncotarget 8:23650–23663. https://doi.org/10.18632/oncotarget.15569
Wu GC, Hu Y, Guan SY et al (2019) Differential plasma expression profiles of long non-coding RNAs reveal potential biomarkers for systemic lupus erythematosus. Biomolecules 9:206. https://doi.org/10.3390/biom9060206
Liao Z, Ye Z, Xue Z et al (2019) Identification of renal long non-coding RNA RP11–2B6.2 as a positive regulator of type i interferon signaling pathway in lupus nephritis. Front Immunol 10:975. https://doi.org/10.3389/fimmu.2019.00975
Pfeffer LM (2011) The role of nuclear factor κB in the interferon response. J Interferon Cytokine Res 31:553–559. https://doi.org/10.1089/JIR.2011.0028
Mazewski C, Perez RE, Fish EN, Platanias LC (2020) Type I interferon (IFN)-regulated activation of canonical and non-canonical signaling pathways. Front Immunol 11:606456. https://doi.org/10.3389/FIMMU.2020.606456
Ivashkiv LB, Donlin LT (2014) Regulation of type I interferon responses. Nat Rev Immunol 14:36–49. https://doi.org/10.1038/NRI3581
Ye H, Wang X, Wang L et al (2019) Full high-throughput sequencing analysis of differences in expression profiles of long noncoding RNAs and their mechanisms of action in systemic lupus erythematosus. Arthritis Res Ther 21:70. https://doi.org/10.1186/s13075-019-1853-7
Wang Y, Chen S, Chen S et al (2018) Long noncoding RNA expression profile and association with SLEDAI score in monocyte-derived dendritic cells from patients with systematic lupus erythematosus. Arthritis Res Ther 20:138. https://doi.org/10.1186/s13075-018-1640-x
Chen X, Luo X, Wei Y et al (2021) LncRNA H19 induces immune dysregulation of BMMSCs, at least partly, by inhibiting IL-2 production. Mol Med 27:61. https://doi.org/10.1186/S10020-021-00326-Y
Zhang Y, **e L, Lu W et al (2021) LncRNA MIAT enhances systemic lupus erythematosus by upregulating CFHR5 expression via miR-222 degradation. Cent Eur J Immunol 46:17–26. https://doi.org/10.5114/CEJI.2021.105242
Lu C, Shao X, Zhou S, Pan C (2021) LINC00176 facilitates CD4+T cell adhesion in systemic lupus erythematosus via the WNT5a signaling pathway by regulating WIF1. Mol Immunol 134:202–209. https://doi.org/10.1016/J.MOLIMM.2021.02.018
Liu X, Lin J, Wu H et al (2021) A novel long noncoding RNA lincRNA00892 Activates CD4+ T cells in systemic lupus erythematosus by regulating CD40L. Front Pharmacol 12:733902. https://doi.org/10.3389/fphar.2021.733902
Chivasso C, Sarrand J, Perret J et al (2021) The involvement of innate and adaptive immunity in the initiation and perpetuation of Sjogren’s syndrome. Int J Mol Sci 22:658. https://doi.org/10.3390/ijms22020658
Chen Y, Chen Y, Zu B et al (2020) Identification of long noncoding RNAs lnc-DC in plasma as a new biomarker for primary Sjogren’s syndrome. J Immunol Res 2020:9236234. https://doi.org/10.1155/2020/9236234
Fu J, Shi H, Wang B et al (2020) LncRNA PVT1 links Myc to glycolytic metabolism upon CD4(+) T cell activation and Sjogren’s syndrome-like autoimmune response. J Autoimmun 107:102358. https://doi.org/10.1016/j.jaut.2019.102358
Dolcino M, Tinazzi E, Vitali C et al (2019) Long non-coding RNAs modulate Sjogren’s syndrome associated gene expression and are involved in the pathogenesis of the disease. J Clin Med 8:1349. https://doi.org/10.3390/jcm8091349
Peng Y, Luo X, Chen Y et al (2020) LncRNA and mRNA expression profile of peripheral blood mononuclear cells in primary Sjogren’s syndrome patients. Sci Rep 10:19629. https://doi.org/10.1038/s41598-020-76701-2
Liu T, Zhang L, Joo D, Sun SC (2017) NF-κB signaling in inflammation. Signal Transduct Target Ther 2:17023. https://doi.org/10.1038/SIGTRANS.2017.23
Moens U, Kostenko S, Sveinbjørnsson B (2013) The role of mitogen-activated protein kinase-activated protein kinases (MAPKAPKs) in inflammation. Genes (Basel) 4:101. https://doi.org/10.3390/GENES4020101
Rawlings JS, Rosler KM, Harrison DA (2004) The JAK/STAT signaling pathway. J Cell Sci 117:1281–1283. https://doi.org/10.1242/JCS.00963
Banerjee S, Biehl A, Gadina M et al (2017) JAK-STAT signaling as a target for inflammatory and autoimmune diseases: current and future prospects. Drugs 77:521–546. https://doi.org/10.1007/S40265-017-0701-9
Inamo J, Suzuki K, Takeshita M et al (2020) Identification of novel genes associated with dysregulation of B cells in patients with primary Sjogren’s syndrome. Arthritis Res Ther 22:153. https://doi.org/10.1186/s13075-020-02248-2
Wu Y-Y, Kuo H-C (2020) Functional roles and networks of non-coding RNAs in the pathogenesis of neurodegenerative diseases. J Biomed Sci 27:49. https://doi.org/10.1186/S12929-020-00636-Z
Tan X, Liu Y, Liu Y et al (2021) Dysregulation of long non-coding RNAs and their mechanisms in Huntington’s disease. J Neurosci Res 99:2074–2090. https://doi.org/10.1002/JNR.24825
Johnson R (2012) Long non-coding RNAs in Huntington’s disease neurodegeneration. Neurobiol Dis 46:245–254. https://doi.org/10.1016/J.NBD.2011.12.006
Zhang H, Wang W, Li N et al (2018) LncRNA DGCR5 suppresses neuronal apoptosis to improve acute spinal cord injury through targeting PRDM5. Cell Cycle 17:1992–2000. https://doi.org/10.1080/15384101.2018.1509622
Lin N, Chang KY, Li Z et al (2014) An evolutionarily conserved long noncoding RNA TUNA controls pluripotency and neural lineage commitment. Mol Cell 53:1005–1019. https://doi.org/10.1016/J.MOLCEL.2014.01.021
Labadorf A, Hoss AG, Lagomarsino V et al (2015) RNA sequence analysis of human huntington disease brain reveals an extensive increase in inflammatory and developmental gene expression. PLoS ONE 10:e0143563. https://doi.org/10.1371/JOURNAL.PONE.0143563
Colpo GD, Rocha NP, Stimming EF, Teixeira AL (2020) Gene expression profiling in Huntington’s disease: does comorbidity with depressive symptoms matter? Int J Mol Sci 21:8474. https://doi.org/10.3390/IJMS21228474
Kouli A, Torsney KM, Kuan W-L (2018) Parkinson’s disease: etiology, neuropathology, and pathogenesis. Parkinson’s Disease: Pathogenesis and Clinical Aspects 3–26. https://doi.org/10.15586/CODONPUBLICATIONS.PARKINSONSDISEASE.2018.CH1
Kraus TFJ, Haider M, Spanner J et al (2016) Altered long noncoding RNA expression precedes the course of Parkinson’s disease—a preliminary report. Mol Neurobiol 54:2869–2877. https://doi.org/10.1007/S12035-016-9854-X
Ding XM, Zhao LJ, Qiao HY et al (2019) Long non-coding RNA-p21 regulates MPP+-induced neuronal injury by targeting miR-625 and derepressing TRPM2 in SH-SY5Y cells. Chem Biol Interact 307:73–81. https://doi.org/10.1016/J.CBI.2019.04.017
Xu X, Zhuang C, Wu Z et al (2018) LincRNA-p21 inhibits cell viability and promotes cell apoptosis in Parkinson’s disease through activating α-synuclein expression. Biomed Res Int 2018:8181374. https://doi.org/10.1155/2018/8181374
Ye Y, He X, Lu F et al (2018) A lincRNA-p21/miR-181 family feedback loop regulates microglial activation during systemic LPS- and MPTP- induced neuroinflammation. Cell Death Dis 9:803. https://doi.org/10.1038/s41419-018-0821-5
He X, Yuan W, Yang CQ et al (2022) Ghrelin alleviates 6-hydroxydopamine-induced neurotoxicity in SH-SY5Y cells. Neural Regen Res 17:170–177. https://doi.org/10.4103/1673-5374.314314
Zhang Y, **a Q, Lin J (2020) LncRNA H19 attenuates apoptosis in MPTP-induced Parkinson’s disease through regulating miR-585-3p/PIK3R3. Neurochem Res 45:1700–1710. https://doi.org/10.1007/s11064-020-03035-w
Jiang J, Piao X, Hu S et al (2020) LncRNA H19 diminishes dopaminergic neuron loss by mediating microRNA-301b-3p in Parkinson’s disease via the HPRT1-mediated Wnt/β-catenin signaling pathway. Aging (Albany NY) 12:8820–8836. https://doi.org/10.18632/AGING.102877
Ghafouri-Fard S, Gholipour M, Abak A et al (2021) Expression analysis of NF-κB-related lncRNAs in Parkinson’s disease. Front Immunol 12:755246. https://doi.org/10.3389/FIMMU.2021.755246
Xu X, Zhang Y, Kang Y et al (2021) LncRNA MIAT inhibits MPP+-induced neuronal damage through regulating the miR-132/SIRT1 axis in PC12 cells. Neurochem Res 46:3365–3374. https://doi.org/10.1007/s11064-021-03437-4
Shen Y, Cui X, Hu Y et al (2021) LncRNA-MIAT regulates the growth of SHSY5Y cells by regulating the miR-34-5p-SYT1 axis and exerts a neuroprotective effect in a mouse model of Parkinson’s disease. Am J Transl Res 13:9993–10013
Lang Y, Zhang H, Yu H et al (2022) Long non-coding RNA myocardial infarction-associated transcript promotes 1-Methyl-4-phenylpyridinium ion-induced neuronal inflammation and oxidative stress in Parkinson’s disease through regulating microRNA-221-3p/ transforming growth factor /nuclear factor E2-related factor 2 axis. Bioengineered 13:930–940. https://doi.org/10.1080/21655979.2021.2015527
Zhou S, Zhang D, Guo J et al (2020) Long non-coding RNA NORAD functions as a microRNA-204-5p sponge to repress the progression of Parkinson’s disease in vitro by increasing the solute carrier family 5 member 3 expression. IUBMB Life 72:2045–2055. https://doi.org/10.1002/IUB.2344
Lu M, Sun WL, Shen J et al (2018) LncRNA-UCA1 promotes PD development by upregulating SNCA. Eur Rev Med Pharmacol Sci 22:7908–7915. https://doi.org/10.26355/EURREV_201811_16417
Zheng Y, Liu J, Zhuang J et al (2021) Silencing of UCA1 protects against MPP+-induced cytotoxicity in SK-N-SH cells via modulating KCTD20 expression by sponging miR-423-5p. Neurochem Res 46:878–887. https://doi.org/10.1007/s11064-020-03214-9
Li D, Zhang J, Li X et al (2020) Insights into lncRNAs in Alzheimer’s disease mechanisms. RNA Biol 18:1037–1047. https://doi.org/10.1080/15476286.2020.1788848
Jiang Q, Shan K, Qun-Wang X et al (2016) Long non-coding RNA-MIAT promotes neurovascular remodeling in the eye and brain. Oncotarget 7:49688–49698. https://doi.org/10.18632/ONCOTARGET.10434
Fan Y, Zhang J, Zhuang X et al (2021) Epigenetic transcripts of LINC01311 and hsa-miR-146a-5p regulate neural development in a cellular model of Alzheimer’s disease. IUBMB Life 73:916–926. https://doi.org/10.1002/IUB.2472
Zhang Y-Y, Bao H-L, Dong L-X et al (2021) Silenced lncRNA H19 and up-regulated microRNA-129 accelerates viability and restrains apoptosis of PC12 cells induced by Aβ25-35 in a cellular model of Alzheimer’s disease. Cell Cycle 20:112–125. https://doi.org/10.1080/15384101.2020.1863681
Yan Y, Yan H, Teng Y et al (2020) Long non-coding RNA 00507/miRNA-181c-5p/TTBK1/MAPT axis regulates tau hyperphosphorylation in Alzheimer’s disease. J Gene Med 22:e3268. https://doi.org/10.1002/JGM.3268
Li D, Zhang J, Wang M et al (2018) Activity dependent LoNA regulates translation by coordinating rRNA transcription and methylation. Nat Commun 9:1726. https://doi.org/10.1038/s41467-018-04072-4
Hong H, Mo Y, Li D et al (2020) Aberrant expression profiles of lncRNAs and their associated nearby coding genes in the hippocampus of the samp8 mouse model with AD. Mol Ther Nucleic Acids 20:140–154. https://doi.org/10.1016/J.OMTN.2020.02.008
Cao M, Li H, Zhao J et al (2019) Identification of age- and gender-associated long noncoding RNAs in the human brain with Alzheimer’s disease. Neurobiol Aging 81:116–126. https://doi.org/10.1016/J.NEUROBIOLAGING.2019.05.023
Garofalo M, Pandini C, Bordoni M et al (2020) Alzheimer’s, Parkinson’s disease and amyotrophic lateral sclerosis gene expression patterns divergence reveals different grade of RNA metabolism involvement. Int J Mol Sci 21:9500. https://doi.org/10.3390/IJMS21249500
Imamura K, Imamachi N, Akizuki G et al (2014) Long noncoding RNA NEAT1-dependent SFPQ relocation from promoter region to paraspeckle mediates IL8 expression upon immune stimuli. Mol Cell 53:393–406. https://doi.org/10.1016/j.molcel.2014.01.009
Lund BT, Ashikian N, Ta HQ et al (2004) Increased CXCL8 (IL-8) expression in multiple sclerosis. J Neuroimmunol 155:161–171. https://doi.org/10.1016/j.jneuroim.2004.06.008
Bsibsi M, Bajramovic JJ, Vogt MH et al (2010) The microtubule regulator stathmin is an endogenous protein agonist for TLR3. J Immunol 184:6929–6937. https://doi.org/10.4049/jimmunol.0902419
Gast M, Rauch BH, Haghikia A et al (2019) Long noncoding RNA NEAT1 modulates immune cell functions and is suppressed in early onset myocardial infarction patients. Cardiovasc Res 115:1886–1906. https://doi.org/10.1093/cvr/cvz085
Liu R, Jiang C, Li J et al (2021) Serum-derived exosomes containing NEAT1 promote the occurrence of rheumatoid arthritis through regulation of miR-144-3p/ROCK2 axis. Ther Adv Chronic Dis 12:2040622321991705. https://doi.org/10.1177/2040622321991705
Guo T, **ng Y, Chen Z et al (2021) Long non-coding RNA NEAT1 knockdown alleviates rheumatoid arthritis by reducing IL-18 through p300/CBP repression. Inflammation 45:100–115. https://doi.org/10.1007/s10753-021-01531-x
**ao J, Wang R, Zhou W et al (2021) LncRNA NEAT1 regulates the proliferation and production of the inflammatory cytokines in rheumatoid arthritis fibroblast-like synoviocytes by targeting miR-204-5p. Hum Cell 34:372–382. https://doi.org/10.1007/s13577-020-00461-4
Zhang F, Wu L, Qian J et al (2016) Identification of the long noncoding RNA NEAT1 as a novel inflammatory regulator acting through MAPK pathway in human lupus. J Autoimmun 75:96–104. https://doi.org/10.1016/j.jaut.2016.07.012
Jiang Y, Zhao Y, Mo X (2021) Expression of lncRNA NEAT1 in peripheral blood mononuclear cells of patients with systemic lupus erythematosus and its correlation with Th1/Th2 balance. Int J Clin Exp Pathol 14:646–652
Azari H, Karimi E, Shekari M et al (2021) Construction of a lncRNA-miRNA-mRNA network to determine the key regulators of the Th1/Th2 imbalance in multiple sclerosis. Epigenomics 13:1797–1815. https://doi.org/10.2217/epi-2021-0296
Huang S, Dong D, Zhang Y et al (2021) Long non-coding RNA nuclear paraspeckle assembly transcript 1 promotes activation of T helper 2 cells via inhibiting STAT6 ubiquitination. Hum Cell 34:800–807. https://doi.org/10.1007/s13577-021-00496-1
Ye L, Shi H, Yu C et al (2020) LncRNA Neat1 positively regulates MAPK signaling and is involved in the pathogenesis of Sjogren’s syndrome. Int Immunopharmacol 88:106992. https://doi.org/10.1016/j.intimp.2020.106992
Chanda K, Das S, Chakraborty J et al (2018) Altered Levels of Long NcRNAs Meg3 and Neat1 in Cell And Animal Models Of Huntington’s Disease. RNA Biol 15:1348–1363. https://doi.org/10.1080/15476286.2018.1534524
Sunwoo JS, Lee ST, Im W et al (2017) Altered expression of the long noncoding RNA NEAT1 in Huntington’s disease. Mol Neurobiol 54:1577–1586. https://doi.org/10.1007/S12035-016-9928-9
Cheng C, Spengler RM, Keiser MS et al (2018) The long non-coding RNA NEAT1 is elevated in polyglutamine repeat expansion diseases and protects from disease gene-dependent toxicities. Hum Mol Genet 27:4303–4314. https://doi.org/10.1093/HMG/DDY331
Dong LI, Zheng Y, Gao L, Luo X (2021) lncRNA NEAT1 prompts autophagy and apoptosis in MPTP-induced Parkinson’s disease by impairing miR-374c-5p. Acta Biochim Biophys Sin (Shanghai) 53:870–882. https://doi.org/10.1093/ABBS/GMAB055
Liu T, Zhang Y, Liu W, Zhao J (2020) LncRNA NEAT1 regulates the development of Parkinson’s disease by targeting AXIN1 via sponging miR-212-3p. Neurochem Res 46:230–240. https://doi.org/10.1007/S11064-020-03157-1
Liu R, Li F, Zhao W (2020) Long noncoding RNA NEAT1 knockdown inhibits MPP+-induced apoptosis, inflammation and cytotoxicity in SK-N-SH cells by regulating miR-212-5p/RAB3IP axis. Neurosci Lett 731:135060. https://doi.org/10.1016/J.NEULET.2020.135060
Zhou S, Zhang D, Guo J et al (2021) Deficiency of NEAT1 prevented MPP+-induced inflammatory response, oxidative stress and apoptosis in dopaminergic SK-N-SH neuroblastoma cells via miR-1277-5p/ARHGAP26 axis. Brain Res 1750:147156. https://doi.org/10.1016/J.BRAINRES.2020.147156
Chen M-Y, Fan K, Zhao L-J et al (2021) Long non-coding RNA nuclear enriched abundant transcript 1 (NEAT1) sponges microRNA-124-3p to up-regulate phosphodiesterase 4B (PDE4B) to accelerate the progression of Parkinson’s disease. Bioengineered 12:708–719. https://doi.org/10.1080/21655979.2021.1883279
Wang S, Wen Q, **ong B et al (2021) Long noncoding RNA NEAT1 knockdown ameliorates 1-methyl-4-phenylpyridine–induced cell injury through MicroRNA-519a-3p/SP1 axis in Parkinson disease. World Neurosurg 156:e93–e103. https://doi.org/10.1016/J.WNEU.2021.08.147
Boros FA, Vécsei L, Klivényi P (2021) NEAT1 on the field of Parkinson’s disease: offense, defense, or a player on the bench? J Parkinsons Dis 11:123–138. https://doi.org/10.3233/JPD-202374
Spreafico M, Grillo B, Rusconi F et al (2018) Multiple layers of CDK5R1 regulation in Alzheimer’s disease implicate long non-coding RNAs. Int J Mol Sci 19:2022. https://doi.org/10.3390/IJMS19072022
Zhao M-Y, Wang G-Q, Wang N-N et al (2019) The long-non-coding RNA NEAT1 is a novel target for Alzheimer’s disease progression via miR-124/BACE1 axis. Neurol Res 41:489–497. https://doi.org/10.1080/01616412.2018.1548747
Huang Z, Zhao J, Wang W et al (2020) Depletion of LncRNA NEAT1 rescues mitochondrial dysfunction through NEDD4L-dependent PINK1 degradation in animal models of Alzheimer’s disease. Front Cell Neurosci 14:28. https://doi.org/10.3389/FNCEL.2020.00028
Ke S, Yang Z, Yang F et al (2019) Long noncoding RNA NEAT1 aggravates Aβ-induced neuronal damage by targeting miR-107 in Alzheimer’s disease. Yonsei Med J 60:640–650. https://doi.org/10.3349/YMJ.2019.60.7.640
Dong L-X, Zhang Y-Y, Bao H-L et al (2021) LncRNA NEAT1 promotes Alzheimer’s disease by down regulating micro-27a-3p. Am J Transl Res 13:8885–8896
Arun G, Aggarwal D, Spector DL (2020) MALAT1 long non-coding RNA: functional implications. Non-Coding RNA 6:22. https://doi.org/10.3390/NCRNA6020022
Cardamone G, Paraboschi EM, Solda G et al (2019) Not only cancer: the long non-coding RNA MALAT1 affects the repertoire of alternatively spliced transcripts and circular RNAs in multiple sclerosis. Hum Mol Genet 28:1414–1428. https://doi.org/10.1093/hmg/ddy438
Ghaderian S, Shomali N, Behravesh S et al (2020) The emerging role of lncRNAs in multiple sclerosis. J Neuroimmunol 347:577347. https://doi.org/10.1016/j.jneuroim.2020.577347
Li GQ, Fang YX, Liu Y et al (2019) MALAT1-driven inhibition of Wnt signal impedes proliferation and inflammation in fibroblast-like synoviocytes through CTNNB1 promoter methylation in rheumatoid arthritis. Hum Gene Ther 30:1008–1022. https://doi.org/10.1089/hum.2018.212
Yang H, Liang N, Wang M et al (2017) Long noncoding RNA MALAT-1 is a novel inflammatory regulator in human systemic lupus erythematosus. Oncotarget 8:77400–77406. https://doi.org/10.18632/oncotarget.20490
Chen Q, Huang X, Li R (2018) lncRNA MALAT1/miR-205-5p axis regulates MPP+-induced cell apoptosis in MN9D cells by directly targeting LRRK2. Am J Transl Res 10:563–572
Lv K, Liu Y, Zheng Y et al (2021) Long non-coding RNA MALAT1 regulates cell proliferation and apoptosis via miR-135b-5p/GPNMB axis in Parkinson’s disease cell model. Biol Res 54:10. https://doi.org/10.1186/s40659-021-00332-8
Liu W, Zhang Q, Zhang J et al (2017) Long non-coding RNA MALAT1 contributes to cell apoptosis by sponging miR-124 in Parkinson disease. Cell Biosci 7:19. https://doi.org/10.1186/S13578-017-0147-5
Lu Y, Gong Z, ** X et al (2020) LncRNA MALAT1 targeting miR-124-3p regulates DAPK1 expression contributes to cell apoptosis in Parkinson’s Disease. J Cell Biochem 121:4838–4848. https://doi.org/10.1002/JCB.29711
Cai LJ, Tu L, Huang XM et al (2020) LncRNA MALAT1 facilitates inflammasome activation via epigenetic suppression of Nrf2 in Parkinson’s disease. Mol Brain 13:130. https://doi.org/10.1186/s13041-020-00656-8
Angelopoulou E, Paudel YN, Piperi C (2019) miR-124 and Parkinson’s disease: a biomarker with therapeutic potential. Pharmacol Res 150:104515. https://doi.org/10.1016/J.PHRS.2019.104515
Zhuang J, Cai P, Chen Z et al (2020) Long noncoding RNA MALAT1 and its target microRNA-125b are potential biomarkers for Alzheimer’s disease management via interactions with FOXQ1, PTGS2 and CDK5. Am J Transl Res 12:5940–5954
Ma P, Li Y, Zhang W et al (2019) Long non-coding RNA MALAT1 inhibits neuron apoptosis and neuroinflammation while stimulates neurite outgrowth and its correlation with MiR-125b mediates PTGS2, CDK5 and FOXQ1 in Alzheimer’s disease. Curr Alzheimer Res 16:596–612. https://doi.org/10.2174/1567205016666190725130134
Li L, Xu Y, Zhao M, Gao Z (2020) Neuro-protective roles of long non-coding RNA MALAT1 in Alzheimer’s disease with the involvement of the microRNA-30b/CNR1 network and the following PI3K/AKT activation. Exp Mol Pathol 117:104545. https://doi.org/10.1016/J.YEXMP.2020.104545
Matsuda S, Nakagawa Y, Tsuji A et al (2018) Implications of PI3K/AKT/PTEN signaling on superoxide dismutases expression and in the pathogenesis of Alzheimer’s disease. Diseases 6:28. https://doi.org/10.3390/DISEASES6020028
Parobkova E, Matej R (2021) Amyotrophic lateral sclerosis and frontotemporal lobar degenerations: similarities in genetic background. Diagnostics 11:509. https://doi.org/10.3390/DIAGNOSTICS11030509
Liu D, Zuo X, Zhang P et al (2021) The novel regulatory role of lncRNA-miRNA-mRNA axis in amyotrophic lateral sclerosis: an integrated bioinformatics analysis. Comput Math Methods Med 2021:5526179. https://doi.org/10.1155/2021/5526179
Chen K-W, Chen J-A (2020) Functional roles of long non-coding RNAs in motor neuron development and disease. J Biomed Sci 27:38. https://doi.org/10.1186/S12929-020-00628-Z
Nishimoto Y, Nakagawa S, Hirose T et al (2013) The long non-coding RNA nuclear-enriched abundant transcript 1_2 induces paraspeckle formation in the motor neuron during the early phase of amyotrophic lateral sclerosis. Mol Brain 6:31. https://doi.org/10.1186/1756-6606-6-31
Shelkovnikova TA, Kukharsky MS, An H et al (2018) Protective paraspeckle hyper-assembly downstream of TDP-43 loss of function in amyotrophic lateral sclerosis. Mol Neurodegener 13:30. https://doi.org/10.1186/S13024-018-0263-7
An H, Skelt L, Notaro A et al (2019) ALS-linked FUS mutations confer loss and gain of function in the nucleus by promoting excessive formation of dysfunctional paraspeckles. Acta Neuropathol Commun 7:7. https://doi.org/10.1186/S40478-019-0658-X
Shelkovnikova TA, Robinson HK, Troakes C et al (2014) Compromised paraspeckle formation as a pathogenic factor in FUSopathies. Hum Mol Genet 23:2298–2312. https://doi.org/10.1093/HMG/DDT622
Matsukawa K, Kukharsky MS, Park SK et al (2021) Long non-coding RNA NEAT1_1 ameliorates TDP-43 toxicity in in vivo models of TDP-43 proteinopathy. RNA Biol 18:1546–1554. https://doi.org/10.1080/15476286.2020.1860580
Zhou H, Sun L, Wan F (2019) Molecular mechanisms of TUG1 in the proliferation, apoptosis, migration and invasion of cancer cells (Review). Oncol Lett 18:4393–4402. https://doi.org/10.3892/ol.2019.10848
Khalil AM, Guttman M, Huarte M et al (2009) Many human large intergenic noncoding RNAs associate with chromatin-modifying complexes and affect gene expression. Proc Natl Acad Sci U S A 106:11667–11672. https://doi.org/10.1073/PNAS.0904715106
Cheng J, Duan Y, Zhang F et al (2021) The role of lncRNA TUG1 in the Parkinson disease and its effect on microglial inflammatory response. Neuromolecular Med 23:327–334. https://doi.org/10.1007/s12017-020-08626-y
Zhai K, Liu B, Gao L (2020) Long-noncoding RNA TUG1 promotes Parkinson’s disease via modulating MiR-152-3p/PTEN pathway. Hum Gene Ther 31:1274–1287. https://doi.org/10.1089/HUM.2020.106
Sekar S, Taghibiglou C (2018) Elevated nuclear phosphatase and tensin homolog (PTEN) and altered insulin signaling in substantia nigral region of patients with Parkinson’s disease. Neurosci Lett 666:139–143. https://doi.org/10.1016/J.NEULET.2017.12.049
Li X, Wang S-W, LI X-L et al (2020) Knockdown of long non-coding RNA TUG1 depresses apoptosis of hippocampal neurons in Alzheimer’s disease by elevating microRNA-15a and repressing ROCK1 expression. Inflamm Res 69:897–910. https://doi.org/10.1007/S00011-020-01364-8
Zhang M, Lu N, Guo XY et al (2021) Influences of the lncRNA TUG1-miRNA-34a-5p network on fibroblast-like synoviocytes (FLSs) dysfunction in rheumatoid arthritis through targeting the lactate dehydrogenase A (LDHA). J Clin Lab Anal 35:e23969. https://doi.org/10.1002/jcla.23969
Cao HY, Li D, Wang YP et al (2020) Clinical significance of reduced expression of lncRNA TUG1 in the peripheral blood of systemic lupus erythematosus patients. Int J Rheum Dis 23:428–434. https://doi.org/10.1111/1756-185X.13786
Choudhari R, Sedano MJ, Harrison AL et al (2020) Long noncoding RNAs in cancer: From discovery to therapeutic targets. Adv Clin Chem 95:105–147. https://doi.org/10.1016/BS.ACC.2019.08.003
Li JQ, Hu SY, Wang ZY et al (2016) Long non-coding RNA MEG3 inhibits microRNA-125a-5p expression and induces immune imbalance of Treg/Th17 in immune thrombocytopenic purpura. Biomed Pharmacother 83:905–911. https://doi.org/10.1016/j.biopha.2016.07.057
Moradi A, RahimiNaiini M, Yazdanpanahi N et al (2020) Evaluation of the expression levels of three long non-coding RNAs in multiple sclerosis. Cell J 22:165–170. https://doi.org/10.22074/cellj.2020.6555
Quan Y, Wang J, Wang S, Zhao J (2020) Association of the plasma long non-coding RNA MEG3 with Parkinson’s disease. Front Neurol 11:532891. https://doi.org/10.3389/FNEUR.2020.532891
Huang H, Zheng S, Lu M (2021) Downregulation of lncRNA MEG3 is involved in Parkinson’s disease. Metab Brain Dis 36:2323–2328. https://doi.org/10.1007/s11011-021-00835-z
Yi J, Chen B, Yao X et al (2019) Upregulation of the lncRNA MEG3 improves cognitive impairment, alleviates neuronal damage, and inhibits activation of astrocytes in hippocampus tissues in Alzheimer’s disease through inactivating the PI3K/Akt signaling pathway. J Cell Biochem 120:18053–18065. https://doi.org/10.1002/JCB.29108
Wang W, Min L, Qiu X et al (2021) Biological function of long non-coding RNA (LncRNA) **st. Front Cell Dev Biol 9:645647. https://doi.org/10.3389/FCELL.2021.645647
Wang ZQ, **u DH, Jiang JL, Liu GF (2020) Long non-coding RNA XIST binding to let-7c-5p contributes to rheumatoid arthritis through its effects on proliferation and differentiation of osteoblasts via regulation of STAT3. J Clin Lab Anal 34:e23496. https://doi.org/10.1002/jcla.23496
Zhou Q, Zhang MM, Liu M et al (2021) LncRNA XIST sponges miR-199a-3p to modulate the Sp1/LRRK2 signal pathway to accelerate Parkinson’s disease progression. Aging (Albany NY) 13:4115–4137. https://doi.org/10.18632/AGING.202378
Yue D, Guanqun G, **gxin L et al (2020) Silencing of long noncoding RNA XIST attenuated Alzheimer’s disease-related BACE1 alteration through miR-124. Cell Biol Int 44:630–636. https://doi.org/10.1002/CBIN.11263
Wang X, Wang C, Geng C, Zhao K (2018) LncRNA XIST knockdown attenuates Aβ25-35-induced toxicity, oxidative stress, and apoptosis in primary cultured rat hippocampal neurons by targeting miR-132. Int J Clin Exp Pathol 11:3915–3924
Funding
This work was supported by Polish National Science Centre, Narodowe Centrum Nauki under Grant UMO-2018/30/E/NZ2/00295 (to KDR).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. The first draft of the manuscript was written by Patrycja Plewka and Katarzyna Dorota Raczynska, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval
Ethic approval was not required for the current study.
Consent to Participate
No consent to participate was required for the current study.
Consent to Publish
No consent for publication was required for the current study.
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Plewka, P., Raczynska, K.D. Long Intergenic Noncoding RNAs Affect Biological Pathways Underlying Autoimmune and Neurodegenerative Disorders. Mol Neurobiol 59, 5785–5808 (2022). https://doi.org/10.1007/s12035-022-02941-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12035-022-02941-0