
Abstract
Background
The intracerebral hemorrhage (ICH) score is a simple grading scale that can be used to stratify risk of 30 day mortality in ICH patients. A similar risk stratification scale for subarachnoid hemorrhage (SAH) is lacking. We sought to develop a risk stratification mortality score for SAH.
Methods
With approval from the Institutional Review Board, we retrospectively reviewed 400 consecutive SAH patients admitted to our institution from August 1, 2006 to March 1, 2011. The SAH score was developed from a multivariable logistic regression model which was validated with bootstrap method. A separate cohort of 302 SAH patients was used for evaluation of the score.
Results
Among 400 patients with SAH, the mean age was 56.9 ± 13.9 years (range, 21.5–96.2). Among the 366 patients with known causes of SAH, 292 (79.8 %) of patients had aneurysmal SAH, 65 (17.8 %) were angiogram negative, and 9 (2 %) were other vascular causes. The overall in-hospital mortality rate was 20 %. In multivariable analysis, the variables independently associated with the in-hospital mortality were Hunt and Hess score (HH) (p < 0.0001), age (p < 0.0001), intraventricular hemorrhage (IVH) (p = 0.049), and re-bleed (p = 0.01). The SAH score (0–8) was made by adding the following points: HH (HH1-3 = 0, HH4 = 1, HH5 = 4), age (<60 = 0, 60–80 = 1, ≥80 = 2), IVH (no = 0, yes = 1), and re-bleed within 24 h (no = 0, yes = 1). Using our model, the in-hospital mortality rates for patients with score of 0, 1, 2, 3, 4, 5, 6, and 7 were 0.9, 4.5, 9.1, 34.5, 52.9, 60, 82.1, and 83.3 % respectively. Validation analysis indicates good predictive performance of this model.
Conclusion
The SAH score allows a practical method of risk stratification of the in-hospital mortality. The in-hospital mortality increases with increasing SAH mortality score. Further investigation is warranted to validate these findings.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Subarachnoid hemorrhage (SAH) is a neurologic catastrophe with a natural history associated with high morbidity and mortality rates [1]. Sudden death occurs in 12 % of patients even before reaching medical attention [2]. For those who survive the initial hemorrhage, they face a critical period after SAH due to risk from a myriad of complications including cardiac injury, cerebral vasospasm, hydrocephalus, and re-bleeding, which can further devastate the patient. The intracerebral hemorrhage (ICH) score is a simple grading scale that stratifies risk of 30 day mortality in ICH patients [3]. It uses standard clinical and radiographic data such as GCS score, ICH volume, intraventricular hemorrhage (IVH), infratentorial location, and age >80 to predict 30 day mortality, with the 30 day mortality increasing as ICH score increases. The ICH score has become a useful research and clinical tool in risk stratification for ICH. We sought to develop a similar clinico-radiographic risk stratification scale for SAH.
Patients and Methods
With approval from the Institutional Review Board, we retrospectively reviewed 400 consecutive SAH patients admitted to our institution from August 1, 2006 to February 1, 2011. Our institution is a tertiary referral academic medical center that received transfers from surrounding outside hospital’s emergency rooms (ER). Our academic institution has a dedicated closed-unit neuro-intensive care unit staffed only by neurointensivists boarded by the United Council for Neurologic Subspecialities. We have institutional SAH protocols and order sets that are followed on all SAH patients.
Patients were identified from the Get with the Guidelines stroke database. We excluded CT negative SAH and traumatic SAH. Data were collected on demographic information and medical history including age, history of hypertension (HTN), diabetes mellitus (DM), coronary artery disease (CAD), hyperlipidemia (HL), prior stroke, and smoking history. Data were collected on Hunt and Hess score (HH), Glasgow Coma Scale (GCS), in-hospital mortality, and proximate cause of death. Complications, which are collected, included symptomatic cerebral vasospasm (defined as cerebral vasospasm requiring intra-arterial vasodilator infusion or angioplasty), radiographic infarct (defined as new or evolving hypodensity on CT brain), cardiac troponin I (cTI) leak (defined as cTI level >0.5 ng/mL), and re-bleed (defined as new or expanded hemorrhage on CT within 24 h of admission), including pre-hospital or intra-operative rupture. CT brain imaging was reviewed by the study neurologist (VL, SJ, SP) for Fisher scale [4] and the presence of IVH. We chose to use the original Fisher scale rather than the modified Fisher scale, because we wanted to evaluate thickness of blood and the presence of IVH as separate elements rather than a combined data point.
Univariate analysis was performed with Chi square test and Fisher’s exact test as appropriate. Multivariable logistic regression model was used to identify variables that independently predicted in-hospital mortality. Odds ratios (OR), 95 % confidence intervals (CI), and p values were reported. To evaluate predictive performance of our model, internal validation was carried out with bootstrap** (using 500 resamplings) which is an efficient internal validation procedure for logistic regression model [6]. We estimated Optimism-corrected model’s predictive performance including overall performance, discrimination ability, and calibration which were measured with Nagelkerke’s R 2, c statistic (the area under the receiver operating curve), and calibration slope, respectively [5, 6]. The SAH score was developed from the validated model. A separate cohort of 302 SAH patients admitted February 1, 2011 to December 1, 2013 was used to evaluate the performance of the SAH score. All statistical analysis was performed using commercially available statistical software (R version 2.15 and SAS 9.2).
Results
Patient Characteristics
Among 400 patients with SAH, the mean age was 56.9 ±13.9 years (range, 21.5–96.2), and 261 (65.3 %) were female. Baseline characteristics are reported in Table 1.
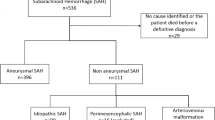
There were 162 (40.5 %) black and 160 (40 %) white. Most were HH2 or 3 (65 %), had IVH (55.4 %), and were Fisher scale 3 (75 %). Most patients (94.2 %) were transfers from outside hospital ERs. Among the 366 patients with known causes, 292 (79.8 %) of patients had aneurysmal SAH, 65 (17.8 %) were angiogram negative, and 9 patients had other vascular lesions (arteriovenous malformation or dural arteriovenous fistula). In a small number of patients (34), testing could not be performed and were of unknown cause. However, most of the patients with unknown cause of SAH died (32). Among the 292 patients with aneurysmal SAH, 179 (61.3 %) underwent endovascular treatment, 93 (31.8 %) underwent surgical treatment, 11 (3.8 %) underwent both, and 9 (3.1 %) expired before any treatment.
Most patients, 261 (65 %), were discharge to home or acute rehabilitation facilities (ARF), and 59 (14.7 %) were discharged to other facility (including nursing home, skilled nursing facility, or ventilator weaning facility). Among survivors, the mean length of stay was 17 ± 8 days (range, 0–77 days). The overall in-hospital mortality rate was 20 %. The mean time to death was 7.5 ± 7.7 days (range 0–31 days). Among 80 patients who died, the cause of the in-hospital mortality was withdrawal of support in 61 (76 %), brain death in 15 (18.8 %), and cardiopulmonary death in 4 (5 %). The mean time to death was significantly different between the groups and was 8.4 days for withdrawal of support, 2.7 days for brain death, and 11.3 days for cardiopulmonary death (p = 0.02). The majority of brain deaths (14/15) occurred within 4 days of admission.
Model Development and Validation
In univariate analysis, the following items were significantly associated with the in-hospital mortality: age, HH, FG, CAD, IVH, prior stroke, GCS, and re-bleed (Table 2). Gender, HTN, DM, HL, symptomatic cerebral vasospasm, and radiographic cerebral infarct were not significantly related to the in-hospital mortality. Significant factors from the univariate analysis were included in the multivariate logistic regression analysis. Based on the distribution of our cohort and their association with the in-hospital mortality, we categorized age as <60, 60–79 and >80 and HH as 1–3, 4 and 5. In multivariate analysis, the variables independently associated with the in-hospital mortality were HH (p < 0.0001), age (p < 0.0001), IVH (p = 0.049), and re-bleed (p = 0.01) (Table 3). We also examined GCS; however, due to its strong correlation with HH, either of them was significant in multivariate analysis, but not both. Since HH and GCS are a measure of the same information, i.e., the patient’s clinical exam severity, we chose to pursue HH as the more relevant scale for SAH patients. From the internal validation analysis with bootstrap**, the optimism corrected Nagelkerke’s R 2, c statistic, and calibration slope were 0.53, 0.91, and 0.95, respectively, which all indicate good predictive performance of this model.
The SAH score
We developed a risk stratification scale (the SAH score) from the above internally validated logistic regression model. Based on the strength of association with the in-hospital mortality, the four predictors were assigned weighted points (Table 4). The weighted points were derived from the regression coefficients from the logistic model. The SAH score was the sum of individual points, and it ranged from 0 to 8.
The in-hospital mortality rates for patients with score of 0, 1, 2, 3, 4, 5, 6, and 7 were 0.9, 4.5, 9.1, 34.5, 52.9, 60, 82.1, and 83.3 %, respectively (Fig. 1). Each increase in the score was associated with an increase in the in-hospital mortality (p < 0.0001 for trend). There were no patients with a score of 8. With 83.3 % mortality rate for patients with score 7, we expect patients with score 8 have even higher risk of mortality. However, this needs to be examined in a larger study. For ease of clinical application of the SAH score, we can simplify the classification of the risk as low (SAH score 0–2), moderate (SAH score 3–5), and high (SAH score 6–8).

Mortality rate based on SAH score
In the separate cohort of 302 SAH patients, there were only few patients with score higher or equal to 6, so we evaluated the SAH score in this cohort with the simplified classification. The in-hospital mortality rates were 4.8, 60, and 71.4 % for patients with low (score 0–2), moderate (score 3–5), and high (score 6–8) risk, respectively.
Discussion
Compared with other stroke subtypes, SAH is an uncommon cause of stroke overall. However, because the median age of death for SAH is 59 years compared with 81 years for ischemic stroke, SAH produces a relatively large burden of premature mortality compared with ischemic stroke [7]. With improved care, SAH mortality has steadily decreased since in the last four decades in the US and internationally [7–11]. Clinical scores, such as HH, GCS, and World Federation of Neurological Surgeons classification, are used as an indicator of clinical severity, which is an indirect maker of prognosis. Studies on long-term mortality in SAH are limited, although the 1-year mortality after SAH is increased compared to matched controls, and this excess risk in SAH survivors is attributable to cerebrovascular disease [12].
Several prognostic scores have been developed in the SAH population. The SAH physiological derangement score was developed from a prospective observational study of 413 SAH patients [13]. Among 20 physiologic variables, 4 were independently associated with death or severe disability at 3 months, including Arteriolar–alveolar gradient, Serum bicarb, Serum glucose, and Mean arterial pressure. Although the SAH physiologic derangement score provides useful information, it was made by adjusting for over-riding “known predictors” of mortality, such as in-hospital re-bleeding, aneurysm size, IVH, LOC, HH, and age. Because the SAH physiologic derangement score excluded factors more meaningful and relevant to mortality, it is not clinically intuitive for practitioners and has not gained widespread use. The admission bioclinical score (ABC score) was developed using data from 526 aneurysmal subarachnoid hemorrhage (aSAH) patients who underwent aneurysm coiling [14]. This ABC score predicts 1-year mortality and consists of GCS, S100 B, and cTI. However, this study had selection bias by only including SAH patients who survived long enough to be coiled (excluding those who were clipped or did not receive aneurysm treatment), thus limiting the generalizability of their findings. Turck et al. [15] developed a six-parameter clinical and biomarker panel, including WFNS, H-FABP, S100B, NDKA, UFD-1, and cT1, to predict unfavorable clinical 6 month outcomes after aSAH.
The elements of our SAH score have been consistently associated with mortality in previously published reports. The severities of the initial hemorrhage (as measured by HH and the presence of IVH), age, and re-bleeding have been consistently shown to impact mortality in SAH [16, 17]. Naidech reported a re-bleed rate of 6.9 % and those with re-bleed were more likely to die in the hospital [17]. Short-term (30 day) mortality was 45 % in the Cincinnati study, a large representative metropolitan population, with most deaths occurring early within the first 2 days and attributable to the initial hemorrhage or re-bleeding [16]. Our data also confirm that many deaths in SAH occur early, with over one-third (37.5 %) occurring within 2 days and over half (53.8 %) the deaths occurring within 5 days. Mortality from brain death occurs significantly earlier than death due to other causes. Thus, it is reasonable to suggest that factors impacting early mortality (such as severity of initial hemorrhage or re-bleeding) have a greater impact on short-term SAH mortality compared with delayed complications.
Other elements that have been traditionally considered a significant cause of mortality after SAH were not found to be independent predictors of the in-hospital mortality in our analysis and were therefore excluded from the SAH mortality score. Two elements that deserve mention are cerebral vasospasm and cardiac injury. Cerebral vasospasm (and by extrapolation radiographic infarct) were not included in the SAH mortality score, because both elements were not found to be independent predictors of the in-hospital mortality. The International Cooperative Study on the Timing of Aneurysm Surgery reported that delayed arterial vasospasm accounted for a quarter of deaths at 6 months [18]. Of note, the International Cooperative Study by design excluded moribund patients and thus likely underestimated the impact of the initial severity of SAH and re-bleeding. In contrast, the Cincinnati population-based study found that most deaths were due to the initial hemorrhage and vasospasm played a minor role in 30 day mortality [16]. Our data confirm the results of the Cincinnati study, and cerebral vasospasm likely contributes to poor functional outcomes rather than short-term mortality.
Although perimesencephalic angiogram negative SAH has reduced complications and good outcome, angiogram-negative non-perimesencephalic SAH is not a benign entity and is associated with complications seen in aSAH [19, 20]. There is also a high frequency of early mortality in SAH patients, with the result that many patients expire before work-up can be completed to determine the cause. In our cohort, 34 (8 %) were unknown category (testing was not completed), and among these patients 32 (94 %) died. The unknown category comprises 40 % of the overall deaths. To exclude a large proportion of SAH patients in a mortality, study would artificially attribute more importance to factors that may not be associated with true mortality. For these reasons, we chose to include all SAH patients in our dataset.
The advantage of our SAH score is that it is simple for clinicians to use, incorporates intuitive information that is part of standard clinical and radiographic bedside assessment of SAH patients, and offers objective standardized risk stratification. The results appear to be logical and appropriate with mortality increasing steadily with SAH score. The elements of the SAH score can be easily recalled by the mnemonic HAIR (HH, Age, IVH, Re-bleed).
A major limitation of the SAH score is that since the proximate cause of death in most SAH patients is withdrawal of care (comfort care), these results could be part of a “self-fulfilling prophecy” via withdrawal of care. In ICH as well, withdrawal of support has been shown to be proximate cause of death in the majority of patients [21]. Aggressiveness of care by hospitals (as measured by early DNR order) has shown to impact mortality in ICH even after adjusting for case mix [22]. ICH patients with early care limitations have a mortality rate in excess of that predicted by scores, even after adjustment for expected predictors of ICH mortality [23, 24]. These same concerns in the ICH population are prevalent with SAH models of mortality. Just as ICH predictive models’ performance is impacted by early DNR status, it would be reasonable to assume that SAH score would also underestimate mortality in patients with early care limitations and overestimate mortality in those without early DNR orders. However, despite these limitations, the ICH score has still remained a useful clinical and research tool. Therefore, a similar SAH score may still be useful to clinicians and researchers, as long as potential pitfalls and limitations are recognized. Just as the ICH mortality score has found use as a research tool to adjust for ICH severity, we expect that SAH HAIR score can also be useful as a “severity” score, and we do not advocate using this score to prognosticate. Other limitations of our study include issues inherent to a retrospective study, such as biased recall and missing data. Of note, there were only a few patients with score 7 and no patients in the subgroup with the highest score (score 8). Our results represent one institution’s experience, and these results need to be validated externally in independent cohorts with larger numbers.
Conclusion
The SAH score allows for risk stratification of the in-hospital mortality. The in-hospital mortality increases with increasing SAH mortality score. Further investigation is warranted to validate these findings.
References
Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Huffman MD, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Magid D, Marcus GM, Marelli A, Matchar DB, McGuire DK, Mohler ER, Moy CS, Mussolino ME, Nichol G, Paynter NP, Schreiner PJ, Sorlie PD, Stein J, Turan TN, Virani SS, Wong ND, Woo D, Turner MB, American Heart Association Statistics Committee, Stroke Statistics Subcommittee. Heart disease and stroke statistics—2013 update: a report from the American Heart Association. Circulation. 2013;1(127):e6–245.
Schievink WI, Wijdicks EF, Parisi JE, Piepgras DG, Whisnant JP. Sudden death from aneurysmal subarachnoid hemorrhage. Neurology. 1995;45:871–4.
Hemphill JC III, Bonovich DC, Besmertis L, Manley GT, Johnston SC. The ICH score: a simple, reliable grading scale for intracerebral hemorrhage. Stroke. 2001;32:891–7.
Fisher CM, Kistler JP, Davis JM. Relation of cerebral vasospasm to subarachnoid hemorrhage visualized by computerized tomographic scanning. Neurosurgery. 1980;6:1–9.
Steyerberg EW, Vickers AJ, Cook NR, Gerds T, Gonen M, Obuchowski N, Pencina MJ, Kattan MW. Assessing the performance of prediction models—a framework for traditional and novel measures. Epidemiology. 2010;21:128–38.
Steyerberg EW, Harrell FE Jr, Borsboom GJJM, Eijkemans MJC, Vergouwe Y, Habbema JDF. Internal validation of predictive models: efficiency of some procedures for logistic regression analysis. J Clin Epidemiol. 2001;54:774–81.
Johnston SC, Selvin S, Gress DR. The burden, trends, and demographics of mortality from subarachnoid hemorrhage. Neurology. 1998;50:1413–8.
Hop JW, Rinkel GJ, Algra A, van Gijn J. Case-fatality rates and functional outcome after subarachnoid hemorrhage: a systematic review. Stroke. 1997;28:660–4.
Koffijberg H, Buskens E, Granath F, Adami J, Ekbom A, Rinkel GJ, et al. Subarachnoid haemorrhage in Sweden 1987–2002: regional incidence and case fatality rates. J Neurol Neurosurg Psychiatry. 2008;79:294–9.
Nieuwkamp DJ, Setz LE, Algra A, Linn FH, de Rooij NK, Rinkel GJE. Changes in case fatality of aneurysmal subarachnoid haemorrhage over time, according to age, sex, and region: a meta-analysis. Lancet Neurol. 2009;8:635–42.
Lovelock CE, Rinkel GJE, Rothwell PM. Time trends in outcome of subarachnoid hemorrhage: population-based study and systematic review. Neurology. 2010;74:1494–501.
Korja M, Silventoinen K, Laatikainen T, Jousilahti P, Salomaa V, Kaprio J. Cause-specific mortality of 1-year survivors of subarachnoid hemorrhage. Neurology. 2013;80:1–6.
Claassen J, Vu A, Kreiter KT, Kowalski RG, Du EY, Ostapkovich N, Fitzsimmons BF, Connolly ES, Mayer SA. Effect of acute physiologic derangements on outcome after subarachnoid hemorrhage. Crit Care Med. 2004;32:832–8.
Degos V, Apfel CC, Sanchez P, Colonne C, Renuit I, Clarencon F, Nouet A, Boch AL, Pourmohamad T, Kim H, Gourraud PA, Young WL, Puybasset L. An admission bioclinical score to predict 1-year outcomes in patients undergoing aneurysm coiling. Stroke. 2012;43:1253–9.
Turck N, Vutskits L, Sanchez-Pena P, Robin X, Hainard A, Gex-Fabry M, Fouda C, Bassem H, Mueller M, Lisacek F, Puybasset L, Sanchez JC. A multiparameter panel method for outcome prediction following aneurysmal subarachnoid hemorrhage. Intensive Care Med. 2010;36:107–15.
Broderick JP, Brott TG, Duldner JE, Tomsick T, Leach A. Initial and recurrent bleeding are the major causes of death following subarachnoid hemorrhage. Stroke. 1994;25:1342–7.
Naidech AM, Janjua N, Kreiter KT, Ostapkovich ND, Fitzsimmons BF, Parra A, Commichau C, Connolly ES, Mayer SA. Predictors and impact of Aneurysm Rebleeding after subarachnoid hemorrhage. Arch Neurol. 2005;62:410–6.
Kassell NF, Torner JC, Haley EC, Jane JA, Adams HP, Kongable GL. The international cooperative study on the timing of Aneurysm surgery. Part 1: overall management RESULTS. J Neurosurg. 1990;73:18–36.
Boswell S, Thorell W, Gogela S, Lyden E, Surdell D. Angiogram-negative subarachnoid hemorrhage: outcomes data and review of the literature. J Stroke Cerebrovasc Dis. 2013;6:750–7.
Lin N, Zenonos G, Kim AH, Nalbach SV, Du R, Frerichs KU, Friedlander RM, Gormley WB. Angiogram-negative subarachnoid hemorrhage: relationship between bleeding pattern and clinical outcome. Neurocrit Care. 2012;3:389–98.
Naidech AM, Bernstein RA, Bassin SL, Garg RJ, Liebling S, Bendok BR, Batjer HH, Bleck TP. How patients die after intracerebral hemorrhage. Neurocrit Care. 2009;11:45–9.
Hemphill JC 3rd, Newman J, Zhao S, Johnston SC. Hospital usage of early do-not-resuscitate orders and outcome after Intracerebral hemorrhage. Stroke. 2004;35:1130–4.
Zahuranec DB, Brown DL, Lisabeth LD, Gonzales NR, Longwell PJ, Smith MA, Garcia NM, Morgenstern LB. Early care limitations independently predict mortality after Intracerebral hemorrhage. Neurology. 2007;68:1651–7.
Zahuranec DB, Morgenstern LB, Sánchez BN, Resnicow K, White DB, Hemphill JC 3rd. Do-not-resuscitate orders and predictive models after intracerebral hemorrhage. Neurology. 2010;75:626–33.
Conflict of interest
Dr. Lee, Dr. Ouyang, Dr. John, Dr. Conners, Dr. Bleck, Dr. Temes, Dr. Cutting have no conflict of interest.
Funding
Dr. Garg received funding from an Unrestricted Clinical Research Training Grant from the AHA. Dr. Prabhakaran received funding from Genentech on QUESTS study in Chicago.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lee, V.H., Ouyang, B., John, S. et al. Risk Stratification for the In-Hospital Mortality in Subarachnoid Hemorrhage: The HAIR Score. Neurocrit Care 21, 14–19 (2014). https://doi.org/10.1007/s12028-013-9952-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-013-9952-9