
Abstract
Background
Traumatic injuries to the cervical spine cause significant disability. Much of the morbidity and mortality that occurs in patients afflicted with cervical spinal cord injury (SCI) occurs early after injury due to primary neurologic dysfunction, systemic inflammation, concomitant injuries, treatments to prevent and ameliorate secondary insults, and prolonged immobilization. This study was undertaken to determine the incidence of organ dysfunction and failure using validated measures: the Multiple Organ Dysfunction Score (MODS) and the Sequential Organ Failure Assessment (SOFA). We also sought to determine if certain patient or injury characteristics were associated with the development of organ dysfunction and failure.
Methods
All patients who sustained isolated blunt cervical SCIs admitted to the R Adams Cowley Shock Trauma Center over a 15-month period were identified. American Spinal Injury Association (ASIA) motor scores, ASIA impairment scale (AIS) scores, and level of injury were recorded. Admission, first daily, worst daily, and aggregate MOD and SOFA scores were assigned for each of six organ systems. A P < 0.05 was considered significant for all statistical tests.
Results
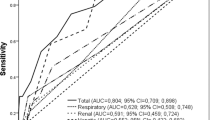
Of 1,028 patients admitted with blunt spine injuries between January, 2007 and March, 2008, 40 patients were identified with an isolated cervical SCI that required an ICU length of stay (LOS) >24 h. Organ failure of at least one organ system occurred in 75% of patients as calculated by MOD score and 85% of patients calculated using SOFA criteria. Multiple organ failure was found in 55% by MOD and 62.5% by SOFA scores. The most frequent system to fail was the cardiovascular system by aggregate MODS (84%), while the respiratory system was the most frequently failed system by aggregate SOFA criteria (70%). There was a strong inverse correlation between ASIA motor score and aggregate MODS and SOFA scores (r = −0.56, P = 0.0002 and r = −0.51, P = 0.0009). AIS was also found to be inversely correlated with the development of organ failure (r = −0.47, P = 0.002 and r = −0.45, P = 0.004) while anatomic level of injury was found to correlate poorly with the incidence of organ failure (r = −0.11, P = 0.5 and r = −0.10, P = 0.5). Only ASIA motor score was significantly associated with sum aggregate organ dysfunction scores when controlling for age and injury severity score (parameter estimate = −0.082, P = 0.0005 for MODS and parameter estimate = −0.057, P = 0.006 for SOFA).
Conclusions
This study is the first to describe the incidence of organ dysfunction and failure in patients with isolated acute traumatic cervical SCI using validated organ system dysfunction scores. Respiratory, cardiovascular, neurologic, renal, hepatic, and hematologic dysfunction occurred commonly both on admission and over the ICU stay. Respiratory, cardiovascular, and neurologic failure were frequently found, while renal, hepatic, and hematologic failures were uncommon. Multiple organ failure occurred in the majority of patients. ASIA motor score and AIS were found to strongly correlate with the development of organ dysfunction and failure. Level of injury should be used with caution when describing the risk of complications and the need for medical interventions.






Similar content being viewed by others


References
National Spinal Cord Injury Statistical Center (2009) Spinal cord injury facts. http://www.fscip.org/facts.htm.
DeVivo MJ, Krause JS, Lammertse DP. Recent trends in mortality and causes of death among persons with spinal cord injury. Arch Phys Med Rehabil. 1999;80:1411–9.
McKinley WO, Jackson AB, Cardenas DD, et al. Long-term medical complications after traumatic spinal cord injury: a regional model systems analysis. Arch Phys Med Rehabil. 1999;80:1402–10.
DeVivo MJ, Ivie III. CS. Life expectancy on ventilator-dependent persons with spinal cord injury. Chest. 1995;108:226–32. doi:10.1378/chest.108.1.226.
Chesnut RM. Management of brain and spine injuries. Crit Care Clin. 2004;20:25–55. doi:10.1016/S0749-0704(03)00090-3.
Licina P, Nowitzke AM. Approach and consideration regarding the patient with spinal injury. Int J Care Injured. 2005;36:S-B2–12. doi:10.1016/j.injury.2005.06.010.
Dewar D, Moore FA, Moore EE, et al. Postinjury multiple organ failure. Int J Care Injured. 2009;40:912–8.
Marshall JC, Cook DJ, Christou NV, et al. Multiple organ dysfunction score: a reliable descriptor of a complex clinical outcome. Crit Care Med. 1995;23(10):1638–52.
Vincent JL, Moreno R, Takala J, et al. The SOFA (sepsis-related organ failure assessment) score to describe organ dysfunction/failure. Intensive Care Med. 1996;22:707–10.
Cook R, Cook D, Tilley J, et al. Multiple organ dysfunction: baseline and serial component scores. Crit Care Med. 2001;29(11):2046–50.
Bota DP, Melot C, Ferreira FL, et al. The multiple organ dysfunction score (MODS) versus the sequential organ failure assessment (SOFA) score in outcome prediction. Intensive Care Med. 2002;28:1619–24.
Grotz M, von Griensven M, Stalp M, et al. Scoring multiple organ failure after severe trauma. Comparison of the Goris, Marshall and Moore scores. Chirurg. 2001;72(6):723–30.
Frink M, van Griensven M, Kobbe P, et al. IL-6 predicts organ dysfunction and mortality in patients with multiple injuries. Scand J Trauma Resusc Emerg Med. 2009;17(1):49.
Antonelli M, Moreno R, Vincent JL, et al. Application of SOFA score to trauma patients. Intensive Care Med. 1999;25:389–94.
Ulvik A, Kvåle R, Wentzel-Larsen T, et al. Multiple organ failure after trauma affects even long-term survival and functional status. Crit Care. 2007;11:R95. doi:10.1186/cc6111.
Zygun DA, Kortbeek JB, Fick GH, et al. Non-neurologic organ dysfunction in severe traumatic brain injury. Crit Care Med. 2005;33(3):654–60.
Zygun D, Berthiaume L, Laupland K, et al. SOFA is superior to MOD score for the determination of non-neurologic organ dysfunction in patients with severe traumatic brain injury: a cohort study. Crit Care. 2006;10:R115. doi:10.1186/cc5007.
Heuer M, Taeger G, Kaiser GM, et al. Prognostic factors of liver injury in polytraumatic patients. Results from 895 severe abdominal trauma cases. J Gastrointestin Liver Dis. 2009;18(2):197–203.
Sauaia A, Moore EE, Johnson JL, et al. Validation of post-injury multiple organ failure scores. Shock. 2009;31(5):438–47.
Abbreviated Injury Scale, 2005. Association for the advancement of automotive medicine: Barrington, IL; 2005.
Apuzzo MLJ. Pharmacological therapy after acute cervical spinal cord injury. In: Guidelines for the management of acute cervical spine and spinal cord injuries, chap 9. Neurosurgery. 2002;50(3):63–72.
Blood pressure management after acute spinal cord injury. In: Guidelines for the management of acute cervical spine and spinal cord injuries, chap 8. Neurosurgery. 2002;50(3):S58–S62.
American Spinal Injury Association/International Medical Society of Paraplegia. International standards for neurological and functional classification of spinal cord injury-Revised 2000. Chicago, IL: ASIA; 2002.
International Standards for the Classification of Spinal Cord Injury. Motor Exam Guide. Downloaded from http://www.asia-spinalinjury.org/publications/Motor_Exam_Guide.pdf.
Standard Neurological Classification of Spinal Cord Injury. Downloaded from http://www.asia-spinalinjury.org/publications/2006_Classif_worksheet.pdf.
Marshall JC. The multiple organ dysfunction (MOD) score. Sepsis. 1997;1:49–52.
Vincent JL, de Mondonca A, Cantraine F, et al. Use the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Crit Care Med. 1998;26(11):1793–800.
Gruber A, Reinprecht A, Illievich UM, et al. Extracerebral organ dysfunction and neurologic outcome after aneurysmal subarachnoid hemorrhage. Crit Care Med. 1999;27(3):505–14.
Solenski NJ, Haley EC, Kassell NF, et al. Medical complications of aneurysmal subarachnoid hemorrhage: a report of the multicenter, cooperative aneurysm study. Crit Care Med. 1995;23(6):992–3.
Lan MY, Wu SJ, Chang YY, et al. Neurologic and non-neurologic predictors of mortality in ischemic stroke patients admitted to the intensive care unit. J Formos Med Assoc. 2006;105(8):653–8.
Kemp CD, Johnson JC, Riordan WP, et al. How we die: the impact of neurologic organ dysfunction after severe traumatic brain injury. J Am Coll Surg. 2008;74(9):866–72.
Gris D, Hamilton EF, Weaver LC. The systemic inflammatory response after spinal cord injury damages the lungs and kidneys. Exp Neurol. 2008;211:259–70.
Kattail D, Furlan JC, Fehlings MG. Epidemiology and clinical outcomes of acute spine trauma and spinal cord injury: experience from a specialized spine trauma center in Canada in comparison with a large national registry. J Trauma. 2009;67(5):936–43.
Claxton AR, Wong DT, Chung F, et al. Predictors of hospital mortality and mechanical ventilation in patients with cervical spinal cord injury. Can J Anaesth. 1998;45(2):144–9.
Bilello JF, Davis JW, Cunningham MA, et al. Cervical spinal cord injury and the need for cardiovascular intervention. Arch Surg. 2003;138:1127–9.
Fletcher DJ, Taddonio RF, Byrne DW, et al. Incidence of acute care complications in vertebral column fracture patients with and without spinal cord injury. Spine. 1995;20(10):1136–46.
Jackson AB, Groomes TE. Incidence of respiratory complications following spinal cord injury. Arch Phys Med Rehabil. 1994;75(3):270–5.
Como JJ, Sutton ERH, McCunn M, et al. Characterizing the need for mechanical ventilation following cervical spinal cord injury with neurologic deficit. J Trauma. 2005;59(4):912–6.
Zimmer MB, Nantwi K, Goshgarian HG. Effect of spinal cord injury on the respiratory system: basic research and current clinical treatment options. J Spinal Cord Med. 2007;30:319–30.
Brown R, DiMarco A, Hoit JD, et al. Respiratory dysfunction and management in spinal cord injury. Respir Care. 2006;51(8):853–70.
Fishburn MJ, Mariano RJ, Ditunno JF Jr. Atelectasis and pneumonia in acute spinal cord injury. Arch Phys Med Rehabil. 1990;71:197–200.
Berlly M, Shem K. Respiratory management during the first five days after spinal cord injury. J Spinal Cord Med. 2007;30(4):309–18.
Lemons VR, Wagner FC Jr. Respiratory complications after cervical spinal cord injury. Spine. 1994;19(20):2315–20.
Winslow C, Rozovsky J. Effect of spinal cord injury on the respiratory system. Am J Phys Med Rehabil. 2003;82:803–14.
Guly HR, Bouamra O, Lecky FE. The incidence of neurogenic shock in patients with isolated spinal cord injury in the emergency department. Resuscitation. 2008;76:57–62.
Tuli S, Tuli J, Coleman WP, et al. Hemodynamic parameters and timing of surgical decompression in acute cervical spinal cord injury. J Spinal Cord Med. 2007;30:482–90.
Teasell RW, Arnold JM, Krassioukov A, et al. Cardiovascular consequences of loss of supraspinal control of the sympathetic nervous system after spinal cord injury. Arch Phys Med Rahbil. 2000;81(4):506–16.
Furlan JC, Fehlings MG. Cardiovascular complications after acute spinal cord injury: pathophysiology, diagnosis, and management. Neurosurg Focus. 2008;25(5):E13.
Mairov DN, Fehlings MG, Krassioukov AV. Relationship between severity of spinal cord injury and abnormalities in neurogenic cardiovascular control in conscious rats. J Neurotrauma. 1998;15(5):365–74.
MacDiarmid SA, McIntyre WJ, Anthony A, et al. Monitoring of renal function in patients with spinal cord injury. Brit J Urol. 2000;85(9):1014–8.
Mohler JL, Barton SD, Blouin RA, et al. The valuation of creatinine clearance in spinal cord injury patients. J Urol. 1986;136:366.
Vaidyanathan S, Watt JWH, Singh G, et al. Dosage of once-daily gentamicin in spinal cord injury patients. Spinal Cord. 2000;38:197–8.
Garcia-Lopez P, Martinez-Cruz A, Guizar-Sahagún G, et al. Acute spinal cord injury changes the disposition of some, but not all drugs given intravenously. Spinal Cord. 2007;45:603–8.
Furlan JC, Krassioukov AV, Fehlings MG. Hematologic abnormalities within the first week after acute isolated traumatic cervical spinal cord injury: a case control cohort study. Spine. 2006;31(23):2674–83.
Wing P, Dalsey W, Alvarez E, et al. Early acute management in adults with spinal cord injury. A clinical practice guideline for health-care professionals. J Spinal Cord Med. 2008;31(4):408–79.
Hassid VJ, Schinco MA, Tepas JJ, et al. Definitive establishment of airway control is critical for optimal outcome in lower cervical spinal cord injury. J Trauma. 2008;65:1328–32.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Stein, D.M., Menaker, J., McQuillan, K. et al. Risk Factors for Organ Dysfunction and Failure in Patients with Acute Traumatic Cervical Spinal Cord Injury. Neurocrit Care 13, 29–39 (2010). https://doi.org/10.1007/s12028-010-9359-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-010-9359-9