
Background
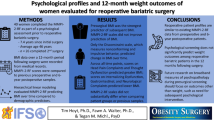
With bariatric restrictive procedures a major issue is predictors of clinical outcome; non-surgical (compliance) and psychological factors might play a role in long term-results of bariatric surgery. We evaluated a set of predictors of short-term and long-term clinical outcome including psychiatric and psychological variables, as well as measures of post-surgery compliance.
Methods
172 consecutive patients undergoing laparoscopic adjustable gastric banding (LAGB) with a minimum of 12 months follow-up, were studied; before surgery they were administered the NIMH Diagnostic Interview Schedule (Version III-R, DIS III-R) and the Structured Clinical Interview for DSM-IV Axis II Personality Disorders (Version 2.0, SCID-II). After surgery, patients were scheduled for visits at 2-week intervals for the first 2 months, at monthly intervals up to 1 year and 3-monthly intervals for 2 years; compliance with diet, rules, physical exercise, plus integrated compliance (sum of scores), and percentage of attendance at scheduled visits were recorded. Patients were contacted again at 36 and at 48 months.
Results
BMI, compliance, percentage of attendance at scheduled visits (positively), and narcissistic personality (negatively) were all associated with weight loss at 12, 24 (and 36 months). Percentage of attendance was also associated at 48 months. At stepwise regression analysis, BMI and integrated compliance predicted weight loss at 12, 24, and 36 months, while percentage of attendance at scheduled visits predicted weight loss at 48 months. Narcissistic personality predicted weight loss only at 12 months.
Conclusion
Adherence to scheduled visits and compliance to recommended rules, more than personality disorders, predict success of LAGB, at least during the first 4 years.
Similar content being viewed by others

References
Sturm R. Increases in clinically severe obesity in the United States, 1986–2000. Arch Intern Med 2003; 163: 2146–8.
Sauerland S, Angrisani L, Belachew M et al. European Association for Endoscopic Surgery. Obesity surgery: evidence-based guidelines of the European Association for Endoscopic Surgery (EAES). Surg Endosc 2005; 19: 200–21.
Buchwald H, Avidor Y, Braunwald E et al. Bariatric surgery: a systematic review and meta-analysis. JAMA 2004; 292: 1724–37.
Hsu LK, Benotti PN, Dwyer J et al. Non-surgical factors that influence the outcome of bariatric surgery: a review. Psychosom Med 1998; 60: 338–46.
Van Hout GCM, Verschure SKM, van Heck GL. Psychosocial predictors of success following bariatric surgery. Obes Surg 2005; 15: 552–60.
Guisado JA, Vaz FJ. Personality profiles of the morbidly obese after vertical banded gastroplasty. Obes Surg 2003; 13: 394–8.
Guisado JA, Vaz FJ, López-Ibor JJ et al. Eating behavior in morbidly obese patients undergoing gastric surgery: Differences between obese people with and without psychiatric disorders. Obes Surg 2001; 11: 576–80.
White MA, Masheb RM, Rothschild BS et al. The prognostic significance of regular binge eating in extremely obese gastric bypass patients: 12-month postoperative outcomes. J Clin Psychiatry 2006; 67: 1928–35.
Lanyon RI, Maxwell BM. Predictors of outcome after gastric bypass surgery. Obes Surg 2007; 17: 321–8.
Kalarchian MA, Marcus MD, Levine MD et al. Psychiatric disorders among bariatric surgery candidates: relationship to obesity and functional health status. Am J Psychiatry 2007; 164: 328–34.
Rosenberger PH, Henderson KE, Grilo CM. Psychiatric disorder comorbidity and association with eating disorders in bariatric surgery patients: A cross-sectional study using structured interview-based diagnosis. J Clin Psychiatry 2006; 67: 1080–5.
Pontiroli AE, Pizzocri P, Librenti MC et al. Laparoscopic adjustable gastric banding for the treatment of morbid (grade 3) obesity and its metabolic complications: a three-year study. J Clin Endocrinol Metab 2002; 87: 3555–61.
Pontiroli AE, Pizzocri P, Giacomelli M et al. Ultrasound measurement of visceral and subcutaneous fat in morbidly obese patients before and after laparoscopic adjustable gastric banding: comparison with computerized tomography and with anthropometric measurements. Obes Surg 2002; 12: 648–51.
Robins L, Helzer JE, Cottler L et al. NIMH Diagnostic Interview Schedule. Version III-R (DIS III-R). St. Louis MO: Washington University School of Medicine, 1989.
American Psychiatric Association. The Diagnostic and Statistical Manual of Mental Disorders, 3rd edn, revised. Washington DC: American Psychiatric Press, 1987.
First MB, Spitzer RL, Gibbon M et al. The Structured Clinical Interview for DSM-IV Axis II Personality Disorders (SCID-II), Version 2.0. New York, NY: Biometrics Research Department, New York State Psychiatric Institute, 1994.
American Psychiatric Association. The Diagnostic and Statistical Manual of Mental Disorders, 4th edn. Washington DC: American Psychiatric Press, 1994.
Maffei C, Fossati A, Agostoni I et al. Interrater reliability and internal consistency of the Structured Clinical Interview for DSMIV Axis II Personality Disorders (SCID-II), Version 2.0. J Pers Dis 1997; 11: 279–84.
Elkins G, Whitfield P, Marcus J et al. Noncompliance with behavioral recommendations following bariatric surgery. Obes Surg 2005; 15: 546–51.
Burgmer R, Grigutsch K, Zipfel S et al. The influence of eating behavior and eating pathology on weight loss after gastric restriction operations. Obes Surg 2005; 15: 684–91.
Israel A, Sebbag G, Fraser D et al. Nutritional behavior as a predictor of early success after vertical gastroplasty. Obes Surg 2005; 15: 88–94.
Busetto L, Segato G, De Luca M et al. Weight loss and postoperative complications in morbidly obese patients with binge eating disorder treated by laparoscopic adjustable gastric banding. Obes Surg 2005; 15: 195–201.
Black DW, Goldstein RB, Mason EE. Psychiatric diagnosis and weight loss following gastric surgery for obesity. Obes Surg 2003; 13: 746–51.
Branson R, Potoczna N, Brunotte R et al. Impact of age, sex and body mass index on outcomes at four years after gastric banding. Obes Surg 2005; 15: 834–42.
Dixon JB, O’Brien PE. Selecting the optimal patient for LAPBAND placement. Am J Surg 2002; 184: 17S–20S.
Watkins BM, Montgomery KF, Ahroni JH. Laparoscopic adjustable gastric banding: early experience in 400 consecutive patients in the USA. Obes Surg 2005; 15: 82–7.
Chau WY, Schmidt HJ, Kouli W et al. Patient characteristics impacting excess weight loss following laparoscopic adjustable gastric banding. Obes Surg 2005; 15: 346–50.
Averbukh Y, Heshka S, El-Shoreya H et al. Depression score predicts weight loss following Roux-en-Y gastric bypass. Obes Surg 2003; 13: 833–6.
Busetto L, Segato G, De Marchi F et al. Outcome predictors in morbidly obese recipients of an adjustable gastric band. Obes Surg 2002; 12: 83–92.
Vallis TM, Ross MA. The role of psychological factors in bariatric surgery for morbid obesity: identification of psychological predictors of success. Obes Surg 1993; 3: 346–51.
Clark MM, Balsiger BM, Sletten CD et al. Psychosocial factors and 2-year outcome following bariatric surgery for weight loss. Obes Surg 2003; 13: 739–45.
Buddeberg-Fischer B, Klaghofer R, Krug L et al. Physical and psychosocial outcome in morbidly obese patients with and without bariatric surgery: a 4 1/2-year follow-up. Obes Surg 2006; 16: 321–30.
Libeton M, Dixon JB, Laurie C et al. Patient motivation for bariatric surgery: characteristics and impact on outcomes. Obes Surg 2004; 14: 392–98.
Ray EC, Nickels MW, Sayeed S et al. Predicting success after gastric bypass: the role of psychosocial and behavioral factors. Surgery 2003; 134: 555–63.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pontiroli, A.E., Fossati, A., Vedani, P. et al. Post-surgery Adherence to Scheduled Visits and Compliance, More than Personality Disorders, Predict Outcome of Bariatric Restrictive Surgery in Morbidly Obese Patients. OBES SURG 17, 1492–1497 (2007). https://doi.org/10.1007/s11695-008-9428-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-008-9428-8