
Abstract
The prevalence of cardiovascular disease increases exponentially with age, highlighting the contribution of aging mechanisms to cardiac diseases. Although model organisms which share human disease pathologies can elucidate mechanisms driving disease, they do not provide us with innate examples how cardiac aging might be slowed or attenuated. The identification of animal models that preserve cardiac function throughout most of life offers an alternative approach to study mechanisms which might slow cardiac aging. One such species may be the naked mole-rat (NMR), a mouse-sized (40 g) rodent with extraordinary longevity (> 37 years), and constant mortality hazard over its four decades of life. We used a cross-sectional study design to measure a range of physiological parameters in NMRs between 2 and 34 years of age and compared these findings with those of mice aged between 3 months and 2.5 years. We observed a rapid decline in body fat content and bone mineral density in old mice, but no changes in NMRs. Similarly, rhythm disorders (premature atrial and ventricular complexes) occurred in aged mice but not in NMRs. Magnetic resonance and ultrasound imaging showed age-dependent increases in cardiac hypertrophy and diastolic dysfunction in mice which were absent in NMRs. Finally, cardiac stress tests showed an age-dependent decline in normalized cardiac output in mice, which was absent in NMRs. Unlike mice, that manifest several aspects of human cardiac aging, NMRs maintain cardiac function and reserve capacity throughout their long lives and may offer insights on how to delay or prevent cardiac aging.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
With aging human populations cardiovascular diseases have become the primary cause of death globally and a substantial burden for healthcare systems [1]. Indeed, age is the strongest risk factor for cardiovascular diseases [2]. Furthermore, the prevalence of many comorbidities such as obesity, dyslipidemia, and diabetes also increases substantially with age compounding the severity of cardiovascular pathology and mortality [3]. Mice manifest many aspects of cardiac aging that are commonly observed in humans. For example, cardiac hypertrophy, diastolic dysfunction, increased rates of arrhythmia, and decreased functional reserve capacity become evident at less than half of their observed maximum lifespan [4,5,6,8, 13, 42, 43], suggesting that left ventricular compliance is well maintained in NMRs. Several factors affect E/A ratios limiting its sensitivity. Newer methods such as E′/A′ and E/E′ particularly when combined with atrial area measurements provide a more sensitive and robust assessment of diastolic dysfunction [44].
Large age-associated changes have been reported for human cardiac reserve capacity [45]. We therefore examined age-associated changes in cardiac reserve capacity in mice and NMRs following beta adrenergic stimulation with dobutamine. Dobutamine administration increased heart rates and contractility in both species, but there was a decline in the chronotropic response in older mice compared to young mice. A decreasing ability to increase heart rates following beta adrenergic stimulation in mice has been reported previously [46], and similar effects have been observed in humans [45, 47,48,49]. While beta adrenergic stimulation led to a small increase in stroke volume in young mice, it reduced stroke volumes in older mice leading to a linear decline in normalized cardiac output with advancing age. Our observations in young mice agree with a previous cardiac MRI study [50], but MRI data for older mice is missing in the literature. Similar to our observation in mice a substantial decline in cardiac reserve capacity with advancing age has been observed in humans [45, 47,48,49]. In contrast to mice and humans, dobutamine-induced increases in stroke volume and cardiac output did not change with age in NMRs indicating preserved cardiac reserve capacity with advancing age.
We relied primarily on ultrasound to measure cardiac parameters in NMRs as all our NMRs are identified by RFID chips, implanted at 90 days in the sub scapular region. These chips often migrate and are found within 3–4 cm from the heart leading to significant signal drop-out on gradient-echo-based MRI. Cardiac MRI is the gold standard for functional assessments in rodents and humans since it does not rely on any geometric assumptions offering full three-dimensional coverage and low variability [51, 52]. The higher variability of ultrasound-based measurements lowers the ability to detect small changes and makes comparisons to MRI based measurements difficult. We consequently performed cardiac MRI on a separate cohort of young and old NMRs whose RFID chips were sufficiently distant from the heart. This analysis showed that NMR cardiac function at rest and under stress does not change with age. It also showed that NMR ejection fraction at rest is approximately 60% and dobutamine increases cardiac output by roughly 10% which is closer to what has been observed in mice than a prior study suggested [53]. The less variable and more precise MRI study confirmed our ultrasound-based findings that NMR cardiac function at rest and under stress does not change with age.
Our ability to detect age-associated changes is limited by two factors: First, the cross-sectional design of our study leads to higher biological variability compared to a longitudinal study where individual baselines can be used for analysis. However, with a maximum lifespan > 38 years in NMRs, longitudinal studies would take decades to complete. Second, the coefficient of variation for the different assays used together with the sample size determines the minimum age-associated change which can be detected. For example, the coefficient of variation for bone mineral density measurements was 2.9% with group sizes n > 24 (assuming no sexual dimorphism) limiting the detectable relative change to 2.4% for a two-point comparison. Using the same assumptions with coefficient of variations for MRI-based stroke volume, ejection fraction, and posterior wall thickness measurements of 12.1, 6.1, and 5.9, respectively, we can expect to detect relative changes greater than 10, 5, and 4.9%. There is also a possibility that differences in response to anesthetic gases between young and old animals affect measurements despite standardized temperatures and breathing rates for data acquisition.
Conclusion
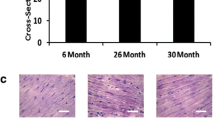
This study demonstrates that unlike mice that exhibit pronounced declines in body composition and cardiac function commencing shortly after sexual maturity, NMRs can maintain tissue homeostasis throughout their four-decade long maximum lifespan. Furthermore, NMRs do not show any signs of diastolic dysfunction or cardiac hypertrophy and maintain similar functional cardiac reserve capacity at advanced age to that exhibited when young adults, at the prime of life. Collectively, these data reveal that the naked mole-rat provides a proof-of-concept that age-related declines in body composition and cardiac function are not inevitable. Elucidating these mechanisms may lead to the discovery of therapies to reduce the burden of age-associated cardiovascular pathology, morbidity, and mortality and thereby enhance quality of life in older humans.
Data availability
Raw data is available upon request.
Code availability
Custom processing scripts are available upon request.
Change history
19 February 2022
A reference entry Laborde S, et al has been changed to Piantoni C, et al.
References
Virani SS, et al. Heart disease and stroke statistics-2020 update: a report from the American Heart Association. Circulation. 2020;141:E139–596.
North BJ, Sinclair DA. The intersection between aging and cardiovascular disease. Circ Res. 2012;110:1097–108.
Moore JX, Chaudhary N, Akinyemiju T. Metabolic syndrome prevalence by race/ethnicity and sex in the United States, National Health and Nutrition Examination Survey, 1988–2012. Prev Chronic Dis. 2017;14:160287.
Feng W, et al. Increased age-related cardiac dysfunction in bradykinin B2 receptor-deficient mice. J Gerontol - Ser A Biol Sci Med Sci. 2016;71:178–87.
Feridooni HA, et al. The impact of age and frailty on ventricular structure and function in C57BL/6J mice. J Physiol. 2017;595:3721–42.
Kiper C, Grimes B, Van Zant G, Satin J. Mouse strain determines cardiac growth potential. PLoS One. 2013;8:e70512.
**e K, et al. Every-other-day feeding extends lifespan but fails to delay many symptoms of aging in mice. Nat Commun. 2017;8:155.
Dai D-F, et al. Overexpression of catalase targeted to mitochondria attenuates murine cardiac aging. Circulation. 2009;119:2789-2797
Buffenstein R, Ruby JG. Opportunities for new insight into aging from the naked mole-rat and other non-traditional models. Nat Aging. 2021;1:3–4.
Buffenstein R. Negligible senescence in the longest living rodent, the naked mole-rat: Insights from a successfully aging species. J Comp Physiol B Biochem Syst Environ Physiol. 2008;178:439–45.
Ruby JG, Smith M, Buffenstein R. Naked mole-rat mortality rates defy gompertzian laws by not increasing with age. Elife. 2018;7:e31157.
Grimes KM, Lindsey ML, Gelfond JAL, Buffenstein R. Getting to the heart of the matter: age-related changes in diastolic heart function in the longest-lived rodent, the naked mole rat. J Gerontol - Ser A Biol Sci Med Sci. 2012;67A:384–94.
Grimes KM, Reddy AK, Lindsey ML, Buffenstein R. And the beat goes on: maintained cardiovascular function during aging in the longest-lived rodent, the naked mole-rat. Am J Physiol - Heart Circ Physiol. 2014;307:H284-91.
Csiszar A, et al. Vascular aging in the longest-living rodent, the naked mole rat. Am J Physiol - Heart Circ Physiol. 2007;293:H919-27.
Riegler J, et al. Comparison of segmentation methods for MRI measurement of cardiac function in rats. J Magn Reson Imaging. 2010;32:869–77.
Heiberg E, et al. Design and validation of segment — freely available software for cardiovascular image analysis. BMC Med Imaging. 2010;10:1.
Keipert S, Voigt A, Klaus S. Dietary effects on body composition, glucose metabolism, and longevity are modulated by skeletal muscle mitochondrial uncoupling in mice. Aging Cell. 2011;10:122–36.
Kyle UG, Genton L, Slosman DO, Pichard C. Fat-free and fat mass percentiles in 5225 healthy subjects aged 15 to 98 years. Nutrition. 2001;17:534–41.
Silver AJ, Guillen CP, Kahl MJ, Morley JE. Effect of aging on body fat. J Am Geriatr Soc. 1993;41:211–3.
Halloran BP, et al. Changes in bone structure and mass with advancing age in the male C57BL/6J mouse. J Bone Miner Res. 2002;17:1044–50.
Ferguson VL, Ayers RA, Bateman TA, Simske SJ. Bone development and age-related bone loss in male C57BL/6J mice. Bone. 2003;33:387–98.
Kim H-K, Lee YJ, Lee Y-K, Kim H, Koo K-H. Which index for muscle mass represents an aging process? J Bone Metab. 2018;25:219.
Edrey YH, Hanes M, Pinto M, Mele J, Buffenstein R. Successful aging and sustained good health in the naked mole rat: A long-lived mammalian model for biogerontology and biomedical research. ILAR J. 2011;52:41–53.
Carmeli-Ligati S, et al. The structure, composition and mechanical properties of the skeleton of the naked mole-rat (Heterocephalus glaber). Bone. 2019;128:115035.
Montoya-Sanhueza G, Bennett NC, Oosthuizen MK, Dengler-Crish CM, Chinsamy A. Bone remodeling in the longest living rodent, the naked mole-rat: Interelement variation and the effects of reproduction. J Anat. 2021;239:81–100
Chow GV, Marine JE, Fleg JL. Epidemiology of arrhythmias and conduction disorders in older adults. Clin Geriatr Med. 2012;28:539–53.
Piantoni C, et al. Age-related changes in cardiac autonomic modulation and heart rate variability in mice. Front Neurosci. 2021;15:617698.
Swedberg K, et al. Prognostic relevance of atrial fibrillation in patients with chronic heart failure on long-term treatment with beta-blockers: results from COMET. Eur Heart J. 2005;26:1303–8.
Køber L, et al. Previously known and newly diagnosed atrial fibrillation: a major risk indicator after a myocardial infarction complicated by heart failure or left ventricular dysfunction. Eur J Heart Fail. 2006;8:591–8.
Dries DL, et al. Atrial fibrillation is associated with an increased risk for mortality and heart failure progression in patients with asymptomatic and symptomatic left ventricular systolic dysfunction: a retrospective analysis of the SOLVD trials. J Am Coll Cardiol. 1998;32:695–703.
Merentie M, et al. Mouse ECG findings in aging, with conduction system affecting drugs and in cardiac pathologies: development and validation of ECG analysis algorithm in mice. Physiol Rep. 2015;3:e12639.
**ng S, et al. Genetic influence on electrocardiogram time intervals and heart rate in aging mice. Am J Physiol - Heart Circ Physiol. 2009;296:H1907-13.
Rossi S, et al. The effect of aging on the specialized conducting system: a telemetry ECG study in rats over a 6 month period. PLoS One. 2014;9:e112697.
Dhingra R, et al. Electrocardiographic QRS duration and the risk of congestive heart failure: The Framingham heart study. Hypertension. 2006;47:861–7.
Dai DF, et al. Age-dependent cardiomyopathy in mitochondrial mutator mice is attenuated by overexpression of catalase targeted to mitochondria. Aging Cell. 2010;9:536–44.
DuPont JJ, Kim SK, Kenney RM, Jaffe IZ. Sex differences in the time course and mechanisms of vascular and cardiac aging in mice: role of the smooth muscle cell mineralocorticoid receptor. Am J Physiol - Heart Circ Physiol. 2021;320:H169–80.
Fraticelli A, Josephson R, Danziger R, Lakatta E, Spurgeon H. Morphological and contractile characteristics of rat cardiac myocytes from maturation to senescence. Am J Physiol - Heat Circ Physiol. 1989;257:H259-65.
Kannel WB. Incidence and epidemiology of heart failure. Heart Fail Rev. 2000;5:167–73.
Spirito P, et al. Magnitude of left ventricular hypertrophy and risk of sudden death in hypertrophic cardiomyopathy. N Engl J Med. 2000;342:1778–85.
Kane GC, et al. Progression of left ventricular diastolic dysfunction and risk of heart failure. JAMA - J Am Med Assoc. 2011;306:856–63.
From AM, Scott CG, Chen HH. The development of heart failure in patients with diabetes mellitus and pre-clinical diastolic dysfunction. a population-based study. J Am Coll Cardiol. 2010;55:300–5.
Medrano G, et al. Left atrial volume and pulmonary artery diameter are noninvasive measures of age-related diastolic dysfunction in mice. J Gerontol - Ser A Biol Sci Med Sci. 2016;71:1141–50.
Chiao YA, et al. Matrix metalloproteinase-9 deletion attenuates myocardial fibrosis and diastolic dysfunction in ageing mice. Cardiovasc Res. 2012;96:444–55.
Schnelle M, et al. Echocardiographic evaluation of diastolic function in mouse models of heart disease. J Mol Cell Cardiol. 2018;114:20–8.
Lakatta EG, Levy D. Arterial and cardiac aging: major shareholders in cardiovascular disease enterprises: Part II: the aging heart in health: Links to heart disease. Circulation. 2003;107:346–54.
Hirleman ED, Yu Q, Larson DF. Lusitrophic effects of dobutamine in young and aged mice in vivo. J Extra Corpor Technol. 2008;40:10–5.
Njemanze H, et al. Age-related decline in cardiac autonomic function is not attenuated with increased physical activity. Oncotarget. 2016;7:76390–7.
Kostis JB, et al. The effect of age on heart rate in subjects free of heart disease. Studies by ambulatory electrocardiography and maximal exercise stress test. Circulation. 1982;65:141–5.
Rodeheffer RJ, et al. Exercise cardiac output is maintained with advancing age in healthy human subjects: cardiac dilatation and increased stroke volume compensate for a diminished heart rate. Circulation. 1984;69:203–13.
Wiesmann F, et al. Dobutamine-stress magnetic resonance microimaging in mice: acute changes of cardiac geometry and function in normal and failing murine hearts. Circ Res. 2001;88:563–9.
Jenkins C, Bricknell K, Hanekom L, Marwick TH. Reproducibility and accuracy of echocardiographic measurements of left ventricular parameters using real-time three-dimensional echocardiography. J Am Coll Cardiol. 2004;44:878–86.
Price AN, et al. Cardiovascular magnetic resonance imaging in experimental models. Open Cardiovasc Med J. 2010;4:278–92.
Grimes KM, et al. Cardiac function of the naked mole-rat: Ecophysiological responses to working underground. Am J Physiol - Heart Circ Physiol. 2014;306:H730-7.
Acknowledgements
We would like to thank the animal care specialists in the Buffenstein laboratory for providing excellent NMR care and assistance with NMR handling.
Funding
This study was funded by Calico Life Sciences LLC.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
E.C., M.S., R.B., and J.R. are employees of Calico Life Sciences LLC.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Can, E., Smith, M., Boukens, B.J. et al. Naked mole-rats maintain cardiac function and body composition well into their fourth decade of life. GeroScience 44, 731–746 (2022). https://doi.org/10.1007/s11357-022-00522-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11357-022-00522-6