
Abstract
Objective
A new vaccine, Multimeric-001, containing conserved linear epitopes from the HA, NP, and M1 proteins of influenza type A and type B strains was designed to protect against seasonal and pandemic influenza virus strains, regardless of mutations. We assessed its safety and tolerability and characterized humoral and cellular immune responses elicited by its administration.
Methods
Sixty healthy volunteers received either 250 or 500 μg injections, with or without adjuvant (Montanide ISA 51VG), or matching placebo. Two intramuscular injections were administered, 21 days apart.
Results
Treatment was well tolerated and no significant adverse events were noted. Forty-two days after first injection, there was a 50-fold and 37-fold increase in IgG titers against Multimeric-001 protein, following the adjuvanted 500 and 250 μg doses, respectively. Sera from immunized subjects lysed MDCK cells infected with strains of influenza representing the major strains that infect humans: H1N1, H3N2, and influenza B. Proliferation of peripheral blood mononuclear cells as well as increase in IL-2 and IFN-gamma secretion occurred following incubation with the vaccine.
Conclusion
This vaccine model differs fundamentally from the current influenza virus vaccines, as it does not contain the variable regions of the virus hemagglutinin and hence does not induce hemagglutination inhibition antibodies that serve as surrogate markers for protection. In order to demonstrate the potential efficacy of the Multimeric-001, an alternative assay was employed, in which the lysis of MDCK cells infected with different virus strains was shown, with the involvement of the complement mechanism. The humoral and cellular responses suggest a cross-immunity of the vaccine toward influenza virus strains regardless of mutations. These results corroborate the protective effect of the vaccine, previously shown in animals. Larger-scale studies are under way to further substantiate the safety and efficacy of the vaccine candidate.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Vaccines used for prevention of influenza act on envelope glycoproteins of either inactivated or live attenuated viruses. These trivalent vaccines contain the hemagglutinin antigen and target two influenza A strains (H1N1 and H3N2) and one influenza B strain. Since the influenza viruses are mutating frequently, the vaccine composition must be adapted to the dominant circulating strains every upcoming winter, based on annual predictions by the World Health Organization [1]. Apart from the inconvenience and logistic implications of yearly vaccinations, the vast genetic variability in influenza strains often results in mismatches between the strains incorporated in the vaccines and those actually prevailing in the population [2–4]. A vaccine that protects against seasonal and pandemic strains, regardless of mutations, could dramatically change the current approach to influenza vaccination by either eliminating the need for annual revaccination or, alternatively, enhancing the immune response in susceptible populations (elderly, for example) and covering circulating strains not targeted in the seasonal vaccine.
One of the new approaches toward a rational design of vaccines is the use of epitopes corresponding to conserved immunogenic sequences of microbial proteins [5]. The epitope-based approach focuses on the minimal component that activates the lymphocyte: short peptides of eight to ten amino acids for activating T cells and longer regions of up to 20 amino acids for the B cell epitopes [6]. Many studies have shown the immunological efficacy of peptide-based vaccines against infectious diseases in animal models [7–10], as well as in clinical studies in which the responses to peptide vaccines against various infectious diseases including malaria [11, 12], hepatitis B [13], and HIV [14, 15] were demonstrated.
Integration of several conserved linear epitopes common to the vast majority of influenza strains potentially increases vaccine efficacy. As the influenza virus invades cells, activation of cell-mediated immunity is crucial for preventing its spread and shortening the duration of illness. Indeed, immunization of mice against influenza viruses with both B and T cell conserved epitopes yielded a response superior to either epitope administered separately [7, 16]. Based on these observations, the new vaccine was designed.
Initially, animal studies were carried out with vaccines containing only some of the epitopes that eventually comprised the final vaccine candidate tested in humans. A proof of concept study was performed in aged mice, employing B cell epitope together with T cell epitopes that target the murine MHC [17]. Another study tested a human–mouse radiation chimera as a model to examine human epitopes. The vaccine candidate used in that study consisted of four epitopes: the same B cell epitope (HA91) together with T cell epitopes that are specific to the common HLA molecules. The four-epitope vaccine was specific, however, only to influenza type A [18]. In these studies, the vaccines elicited both B cell- and T cell-mediated immune responses in vitro and protected mice against infection by several strains of influenza.
The final product selected to be administered to humans in the current study was termed “Multimeric-001.” This vaccine consists of nine conserved epitopes from the HA (four B and one Th epitopes), NP (Two CTL and one Th epitope), and M1 (one peptide that contains both B and CTL epitope) proteins of both influenza type A and type B strains (Victoria and Yamagata lineages) that are known to induce both humoral and cellular immunity. The epitopes are arranged in triplicates combined into a single recombinant polyepitope, as shown in Fig. 1.

Schematic structure and peptide sequence of the Multimeric-001 vaccine
The protein was expressed in Escherichia coli, thus allowing a fast, simple, and robust production process. Animal studies demonstrating the immunogenicity and the protective effects of the complete Multimeric-001 vaccine against various influenza strains have been carried out, as well as safety assessments (unpublished data). The purpose of this first-in-human phase I/II clinical trial was to assess the safety and tolerability of Multimeric-001 and to characterize immune responses elicited by its administration.
Materials and Methods
Study Design and Participants
This was a single-center, randomized, placebo-controlled, single-blind, first-in-human study. The study protocol was approved by the Institutional Review Board of the Tel Aviv Sourasky Medical Center (Tel Aviv, Israel) and was conducted in accordance with the Declaration of Helsinki and its amendments. The trial was registered with the ClinicalTrials.gov registry (number NCT00877448). Written informed consent was obtained from each participant prior to enrollment. Eligible subjects were healthy male and female volunteers aged 18 to 49 years. Any medical condition, clinically significant abnormality upon physical examination or laboratory safety tests, which in the investigator’s judgment contraindicated administration of the vaccine, resulted in exclusion from participation.
Vaccines and Placebos
Multimeric-001 was produced as a recombinant single 50-kDa protein in E. coli using standard fermentation and purification methods employing ion exchange and hydrophobic columns. The vaccine was supplied frozen in single-dose vials intended for intramuscular application. Subjects received twice a 0.2-ml injection of either low (250 μg) or high (500 μg) doses, formulated in PBS or adjuvant, or 0.2 ml of matching placebo. The adjuvant used was Montanide ISA 51 VG (Seppic, France). The two doses were selected based on expected immunogenicity and safety data extrapolated from pre-clinical data. The higher vaccine dose was administered only after the lower dose was proven to be safe.
Procedures
A scheme of the study design and treatment allocation is presented in Fig. 2. For safety reasons, three subjects (“Pioneer Group”) were vaccinated only once with a low dose (125 μg) of the Multimeric-001 vaccine and monitored for 7–9 days before further exposing the rest of the subjects to the planned doses. Sixty participants were then divided in four cohorts of 15 subjects each. Cohort 1 received 250 μg of Multimeric-001 (M250) without adjuvant, cohort 2 received 250 μg of adjuvanted Multimeric-001 (Adj M250), and cohorts 3 and 4 received the 500-μg dose, non-adjuvanted and adjuvanted (M500 and Adj M500), respectively. Two intramuscular injections were administered 21 days apart in the deltoid area of the arm.

Study design and treatment allocation
Within each cohort, subjects were randomized in a 2:1 ratio to receive either Multimeric-001 vaccine or matching placebo containing vehicle only, with or without adjuvant. Since the physical appearance of each formulation was distinguishable to the clinical trial staff, this was designated as a single-blinded study. Blood samples were collected at days 0, 21, and 42 to assess humoral and cellular immune responses.
Safety Evaluation
To assess safety and tolerability end points, the subjects were requested to report in a diary, for the first 7 days after each injection, any adverse event (AE), measure swelling and erythema at the injection site and record daily oral temperatures. Safety follow-up visits took place 7 days after each injection and 21 days after the second administration. Safety evaluations included vital signs, ECG, physical examination, local reaction (Draize score), routine safety lab tests, observed and spontaneously reported AEs, and the diary records.
Assessment of Antibody Response
Specificity and anti-antigen reactivity of IgG against Multimeric-001 protein was measured by indirect ELISA, using plates coated with Multimeric-001 (50 ng/well). A complement-mediated lysis assay, considered more sensitive than the hemagglutination inhibition (HI) test [20], was employed to detect the anti-viral effect of the antibodies raised against Multimeric-001 and the cross-protective immunity potential of this vaccine candidate. In this assay, 2.5 × 106 MDCK target cells were plated in 10 cm plate for 24 h. Next, the cells were trypsinized and infected with representative strains of influenza A/H1N1, A/H3N2, and influenza B: A/New Caledonia/20/99 (H1N1), A/Wisconsin/67/05 (H3N2), or B/Malaysia/2506/04 (Victoria/2/87 lineage) for additional 24 h. The multiplicity of infection is specific for each viral strain, and hence, the exact number was determined to result in 80% well coverage. The infected cells were then incubated with sera of subjects vaccinated with the adjuvanted M500 vaccine or with adjuvanted PBS (placebo) at 1:90, 1:180, 1:360, and 1:720 dilutions that bind the infected cells and mediate lysis by the complement component in a dose related response. Diluted (1:12) normal rabbit serum was added to each well as a source of complement. In addition to the examined sera, each test included control of wells without source of complement. The OD value of this control wells was subtracted from the examined wells. Preliminary setting of this test showed that the use of heat inactive complement leads to the same OD levels that are found in the absence of complement source. Lysed MDCK secrete lactate dehydrogenase to the culture supernatant, and this enzymatic activity was assayed (cytotoxicity kit, Roche) and served as a measure of cell lysis. Spontaneous lysis was subtracted from the specific lysis observed in the experimental and control sera. It should be noted that for each subject, the lysis effect was observed at different sera dilution, and hence, the data are demonstrated as percent responders showing a ≥30% lysis over baseline rather than the exact proportion of lysed cells.
Assessment of Cellular Response
Cellular stimulation was determined by monitoring lymphocyte proliferation and quantification of Th1 cytokines secretion of IL-2 and IFN-gamma in supernatants of peripheral blood mononuclear cells (PBMCs). In brief, PBMCs from all subjects were separated over Ficoll-Paque Plus solution (GE Healthcare, Sweden) and incubated for 72 h in the presence of Multimeric-001, influenza viruses (B/Malaysia/2506/04, A/California/07/2007, A/New Caledonia/20/99), or for 120 h with peptides that are T helper epitopes contained in the vaccine, derived from the NP and HA proteins. Cells were then pulsed with 1 μCi/well 3H-thymidine (18 h, 37°C), and thymidine uptake was measured as a measure for proliferation. Samples for IL-2 and IFN-gamma determination were removed from PBMCs culture media after 24 and 96 h, respectively, and measured by ELISA (Duoset; R&D Systems, Minneapolis, MN, USA).
Data Analysis
No formal sample size calculation was performed for this study, as the study was not designed to show statistical significance or statistical power. Being a pilot study, a sample size of n = 10 in each cohort was considered to be adequate for evaluation of its objectives. Safety data were summarized as descriptive statistics. For assessing immunological parameters, Fisher’s exact test was employed to test the differences in rate of responders between the study groups, and analysis of variance (ANOVA) using Dunnett method was applied to compare the change from days 0 to 42 between each of the treatment group [19]. Statistical analysis was conducted using the SAS® 9.1 software package (SAS Institute, Cary, NC, USA).
Results
Study Subjects
Sixty-three Caucasian male and female subjects were enrolled in the study. Three participants received a single dose of 125 μg and were included in the safety analysis only. The age of the participants ranged between 18.1 and 48.5 years with no statistical difference between cohorts. Of the 60 subjects who were assigned to the full treatment schedule, three withdrew due to reasons unrelated to the treatment.
Safety
Overall, the treatment was well tolerated. Only mild (88.6% of the reported AEs) and moderate adverse events were reported throughout the study and neither severe nor serious AEs were experienced by any of the subjects. The incidence of treatment-emergent adverse events is summarized in Table I.
The onset of AEs designated as “possibly related” occurred within 72 h of vaccination. 60.8% of the reactions resolved fully within 1 day, 25.1% within 2–7 days, and the rest within 8–15 days. There was no significant difference in causality and severity between vaccine recipients and their respective placebo recipients. No adverse events could be attributed specifically to a dose or formulation.
Humoral Immunity
After the first administration of Multimeric-001, only minimal immune responses were observed. Hence, the presented data refer to the response on day 42, i.e., 21 days following the second injection, as compared to day 0.
Multimeric-001-Directed ELISA
Post-immunization antibody titer was calculated as the ratio of mean antibody signal in day 42 and the mean signal in day 0 (Fig. 3 and Table II). Compared to baseline, there was a 50-fold increase following Adj M500 (p ≤ 0.05) and a 37-fold increase in anti-Multimeric-001 IgG titers following the Adj M250 vaccination (p ≤ 0.05). At least 8-fold increase was found in 100% of the subjects in each of these groups. Although the non-adjuvanted formulation also induced IgG responses significantly higher than placebo, the ratio and percentage of responders was substantially lower. As shown in Table II, the titers of the adjuvanted formulations are significantly higher than those found in the non-adjuvanted formulations.

IgG increase after two vaccinations with multimeric-001. IgG titers in sera were determined by indirect ELISA. The adjuvanted and non-adjuvanted formulations were compared with matching placebo (PBS). Quantification (450 nm) of post-immunization antibody titer toward the Multimeric-001 was calculated as a ratio of the mean antibody signal of day 42 and the mean signal of day 0. Error bars represent SE. Statistical significance calculated using Dunnett–ANOVA is marked as *p ≤ 0.05
Antibody-Dependent, Complement-Mediated Lysis
Antibody-dependent, complement-mediated lysis of infected MDCK cells by sera from subjects vaccinated with the adjuvanted 500-μg Multimeric-001 vaccine was by far superior to the other vaccines or placebo (data not shown), resulting in elevated proportion of participants exhibiting ≥30% lysis of MDCK cells infected with different strains of influenza including A/New Caledonia/20/99 (H1N1), A/Wisconsin/67/05 (H3N2), and B/Malaysia/2506/04 (Victoria lineage) strain. The percent of lysis capacity was calculated according to the following formula [20]:
When assessing the individual responses of sera collected from Adj M500-vaccinated subjects on day 42, a 22–28% increase in the percentage of subjects demonstrating a ≥30% elevation in lysis capacity was observed, compared to their adjuvanted placebo counterparts (Fig. 4). These data illustrate the heterotypic humoral immunity conferred by this vaccine. A comparatively high lysis (30%) was observed in pre-immunized sera of the participants. This, together with the small number of subjects per group, resulted in p values ≤0.3 for all three tests as determined using Fisher’s exact test.

Complement-dependent lysis of infected MDCK cells, mediated by sera of Multimeric-001-vaccinated subjects. Sera of subjects vaccinated with adjuvanted M500 (black columns) and adjuvanted PBS as placebo (white columns) were individually tested for their lysis capacities toward MDCK cells infected with one of three representative strains of influenza (A/H1N1, B-Victoria lineage, A/H3N2). The percent of subjects demonstrating lysis of at least 30% (above background) of the infected MDCK cells is presented
Cellular Immunity
PBMCs Proliferation
The most pronounced increase in PBMCs proliferation was observed in subjects who received adjuvanted M500, compared to subjects who received placebo (Fig. 5). A positive trend, yet less significant, was also noted in PBMCs isolated from subjects vaccinated with the other formulations.

Immunization with Multimeric-001 induces proliferation of PBMCs toward the vaccine. PBMCs from each subject on days 0 and 42 were incubated for 72 h with 5 μg of Multimeric-001. Cells were pulsed with 1 μCi/well 3H-thymidine (18 h, 37°C), and thymidine uptake was measured. Values from day 0 were subtracted from day 42 values for each participant; each group consisted of ten participants. Data represent geomean CPM +SE. *p < 0.05; **p < 0.15
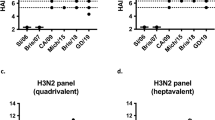
The proliferative response to the different viruses (Fig. 6) that represent the major strains that infect humans, i.e., A/H1N1, A/H3N2, and influenza B, shows the cross-immunity nature of the cellular response induced by this vaccine. Increased proliferation was demonstrated also in response to the Th peptides that are contained in the Multimeric-001 polypeptide showing that they operate as inducers of this response. The other peptides that represent B cell epitope from M1 and a CTL epitope from NP that are also contained in the Multimeric-001 served as negative controls and indeed did not induce proliferation responses.

Immunization with Multimeric-001 induces proliferation of PBMCs. PBMCs from each subject on days 0 and 42 were incubated with 75–150 HAU/well influenza viruses or 50 μg of free peptides M1 (B-cell epitope), NP (CTL epitope), HA (T helper epitope) or NP (T helper epitope), or 5 μg of Multimeric-001. Cells were pulsed with 1 μCi/well 3H-thymidine (18 h, 37°C), and thymidine uptake was measured. Values from day 0 were subtracted from day 42 values. The percent of responders (those demonstrating a minimum 2-fold increase in PBMC proliferation rates in comparison to the pre study levels) to various antigens in vitro is shown. Data were derived from subjects receiving 500-μg doses (black columns) and placebo controls (white columns)
IL-2 and IFN-gamma Secretion by Stimulated PBMCs
IL-2 and IFN-gamma are Th1 cytokines. IL-2 serves as a marker for lymphocyte proliferation, while IFN-gamma, a key player in the first line of anti-viral defense, is part of the non-specific immunity preceding the specific immune response. The concentration of IFN-gamma secreted in response to Multimeric-001 was several hundreds of picograms per milliliter per 25 × 104 cells, comparable to the levels secreted by 106 cells in response to immunization with a whole virus vaccine [21]. A trend of increase in IL-2 and IFN-gamma levels was observed following incubation of the PBMC collected from most vaccinated subjects with the Multimeric-001 vaccine (Fig. 7).

IL-2 and IFN-gamma secretion by PBMCs after exposure to Multimeric-001. PBMCs isolated from vaccinated subjects on days 0 and 42 post-immunization were incubated with 5 μg of Multimeric-001. Supernatant samples were collected after 24 h for IL-2 levels (a) and 96 h for IFN-gamma levels (b). Background signals depicting the amount of cytokines spontaneously released in the absence of antigen were subtracted from all samples. *p ≤ 0.05 (a); **p ≤ 0.15 (b)
Discussion
The data obtained from this first in human study demonstrated a positive safety and tolerability profile in all treatment groups. Robust humoral and cellular immune responses were observed following immunization with the active vaccine. The rate and magnitude of the immune responses were generally higher among subjects immunized with the adjuvanted formulations. In addition, response following the second injection was significantly higher than that of the first vaccination (data not shown). HI marker, currently used for assessing the efficacy of seasonal flu vaccines, is not applicable for the Multimeric-001 vaccine, since only conserved epitopes are included in the Multimeric-001 vaccine whereas the variable regions of hemagglutinin that induce HI antibodies are absent. Therefore, standard neutralization and HI assays are not relevant for the evaluation of this vaccine. Nevertheless, the vaccine proved efficient in animals exposed to various influenza strains. The universality of the vaccine in humans through its proposed humoral action is suggested by demonstrating complement-mediated antibody-dependent lysis. Although the Multimeric-001 does not contain any influenza virus or viral protein, it is capable of inducing virus specific immunity that is mediated by the complement mechanism. Lysis was observed following incubation of Multimeric-001 anti-sera with a source of complement (normal rabbit serum) and with MDCK cells infected with three different influenza virus strains (A/H1N1, A/H3N2, and influenza B-Victoria lineage). These viruses represent the three strains contained in the commercial influenza vaccines. The clinical implication of the 30% increase in lysis, observed in our study, is not clear. This may imply that antibodies specific to Multimeric-001 can reduce the amount of infected cells and facilitate recovery from infection. This issue can probably be further investigated in an in vivo challenge trial.
Cell-mediated immunity acts as a direct regulator of the immune response and is essential for immunity against intra-cellular pathogens including viruses. Therefore, the evaluation of the cell-mediated immunity is a good indicator of the anti-viral immune response of the host. IL-2 was secreted by activated lymphocytes and supports the in vitro proliferation. Its production is representative of PBMC activation. The production of IFN-gamma, observed in response to different human viruses, is an indicator of cell-mediated activity. Future studies with this vaccine candidate will further evaluate and characterize additional parameters of the cellular immunity.
T cell responses to Multimeric-001 were identified in the participants by cell proliferation and Th1 cytokines (IL-2 and IFN-gamma) secretion, following a single in vitro sensitization with Multimeric-001. In the proliferation assays, a marked dose-related response was observed following incubation with the Multimeric-001. The proliferation of lymphocytes following incubation with the different viruses was less pronounced, yet observed in all three tested viruses and showed a clear trend of this virus-specific immunity. The clinical significance of the 2-fold elevation warrants further evaluation. Nonetheless, the proliferation was associated with IL-2 and IFN-gamma secretion. The latter, being a key player in the first line of anti-viral defense, is part of the non-specific immunity activated before the specific immune system response is set off. This cytokine affects the differentiation, survival, and function of immune cells including T cells and dendritic cells and efficiently enhances a primary antibody response [22].
Evidence of anti-influenza immunity, both humoral and cellular, was found in many subjects prior to immunization (day 0), probably due to the background immunity induced by previous exposure to influenza viruses or vaccines. Inter-individual variability in response to both viruses and peptides was therefore more evident in the human subjects than in animals tested in pre-clinical studies. Nevertheless, a cross-strain elevation in humoral immunity was found, demonstrated by the potential capacity of the antibodies to neutralize several influenza strains (A/H1, A/H3, and influenza B) as well as the induction of cell-mediated immunity with anti-viral characteristics. Cross-strain cellular immunity, as described above, was particularly noted in the group immunized with 500 μg without adjuvant.
The Montanide ISA 51VG adjuvant was used in this study since it is known to accelerate both humoral and cellular immunity [15, 23] through several mechanisms such as depot effect, slow antigen release, and recruitment of antigen-presenting cells at the injection site [24]. Elevated humoral responses were indeed more prominent in the adjuvanted formulations. It is noteworthy, however, that Montanide ISA 51VG did not always contribute significantly to the cellular immune response. This was reflected by the fact that incubation with M250 resulted in similar IFN-gamma secretion as in the adjuvanted M500 formulation (Fig. 6b). No AEs attributed specifically to the adjuvant have been observed, and the safety profiles of the adjuvanted and non-adjuvanted formulations were comparable.
Conclusions
This vaccine model differs fundamentally from other universal vaccines currently under development because it is based on multiple B and T cell epitopes from both influenza A and influenza B viruses, combined into a single recombinant protein that can be produced in a fast, standard manufacturing process. The results of this first-in-human trial are encouraging and indicate that Multimeric-001 has the potential of inducing cross-strain immunity. Due to the small number of participants, this study points out trends which are not always statistically significant and must be further substantiated in larger scale studies.
References
World Health Organization. Recommended composition of influenza virus vaccines for use in the 2011 southern hemisphere influenza season. http://www.who.int/csr/disease/influenza/recommendations2011south/en/index.html. Accessed 9 Apr 2011.
Centers for Disease Control and Prevention. Seasonal Influenza (Flu). http://www.cdc.gov/flu/about/qa/flushot.htm. Accessed 9 Apr 2011.
Prevention and Control of Influenza; Recommendations of the Advisory Committee on Immunization Practices (ACIP). http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5306a1.htm. Accessed 9 Apr 2011.
Goodwin K, Viboud C, Simonsen L. Antibody response to influenza vaccination in the elderly: a quantitative review. Vaccine. 2006;24(8):1159–69.
Hans D, Young P, Fairlie D. Current status of short synthetic peptides as vaccines. Med Chem. 2006;2(6):627–46.
Rötzschke O, Falk K, Stevanović S, Jung G, Walden P, Rammensee H. Exact prediction of a natural T cell epitope. Eur J Immunol. 1991;21(11):2891–4.
Ben-Yedidia T, Arnon R. Design of peptide and polypeptide vaccines. Curr Opin Biotechnol. 1997;8(4):442–8.
Snyder J, Belyakov I, Dzutsev A, Lemmonier F, Berzofsky J. Protection against lethal vaccinia virus challenge in HLA-A2 transgenic mice by immunization with a single CD8+ T-cell peptide epitope of vaccinia and variola viruses. J Virol. 2004;78:7052–60.
Hsu S, Chargelegue D, Obeid O, Steward M. Synergistic effect of immunization with a peptide cocktail inducing antibody, helper and cytotoxic T-cell responses on protection against respiratory syncytial virus. J Gen Virol. 1999;80(Pt 6):1401–5.
Azizi A, Diaz-Mitoma F. Viral peptide immunogens: current challenges and opportunities. J Pept Sci. 2007;13(12):776–86.
Kashala O, Amador R, Valero M, et al. Safety, tolerability and immunogenicity of new formulations of the Plasmodium falciparum malaria peptide vaccine SPf66 combined with the immunological adjuvant QS-21. Vaccine. 2002;20(17–18):2263–77.
Nardin E, Oliveira G, Calvo-Calle J, et al. Synthetic malaria peptide vaccine elicits high levels of antibodies in vaccinees of defined HLA genotypes. J Infect Dis. 2000;182(5):1486–96.
Engler O, Dai W, Sette A, Hunziker I, Reichen J, Pichler W, Cerny A. Peptide vaccines against hepatitis B virus: from animal model to human studies. Mol Immunol. 2001;38(6):457–65.
Gahery H, Daniel N, Charmeteau B, Ourth L, Jackson A, Andrieu M, Choppin J, Salmon D, Pialoux G, Guillet J. New CD4+ and CD8+ T cell responses induced in chronically HIV type-1-infected patients after immunizations with an HIV type 1 lipopeptide vaccine. AIDS Res Hum Retroviruses. 2006;22(7):684–94.
Pinto L, Berzofsky J, Fowke K, et al. HIV-specific immunity following immunization with HIV synthetic envelope peptides in asymptomatic HIV-infected patients. AIDS. 1999;13(15):2003–12.
Levi R, Arnon R. Synthetic recombinant influenza vaccine induces efficient long-term immunity and cross-strain protection. Vaccine. 1996;14(1):85–92.
Ben-Yedidia T, Abel L, Arnon R, Globerson A. Efficacy of anti-influenza peptide vaccine in aged mice. Mech Ageing Dev. 1998;104:11–23.
Ben-Yedidia T, Marcus H, Reisner Y, Arnon R. Intranasal administration of peptide vaccine protects human/mouse radiation chimera from influenza infection. Int Immunol. 1999;11:1043–51.
Hsu JC. Multiple comparisons theory and methods. London: Chapman & Hall; 1996.
Quinnan G, Ennis F, Tuazon C, et al. Cytotoxic lymphocytes and antibody-dependent complement-mediated cytotoxicity induced by administration of influenza vaccine. Infect Immun. 1980;30(2):362–9.
Saurwein-Teissl M, Zisterer K, Schmitt T, Glück R, Cryz S, Grubeck-Loebenstein B. Whole virus influenza vaccine activates dendritic cells (DC) and stimulates cytokine production by peripheral blood mononuclear cells (PBMC) while subunit vaccines support T cell proliferation. Clin Exp Immunol. 1998;114(2):271–6.
Proietti E, Bracci L, Puzelli S, Di Pucchio T, Sestili P, De Vincenzi E, Venditti M, Capone I, Seif I, De Maeyer E, Tough D, Donatelli I, Belardelli F. Type I IFN as a natural adjuvant for a protective immune response: lessons from the influenza vaccine model. J Immunol. 2002;169(1):375–83.
Peek L, Middaugh C, Berkland C. Nanotechnology in vaccine delivery. Adv Drug Deliv Rev. 2008;60(8):915–28.
Valmori D, Souleimanian N, Tosello V, et al. Vaccination with NY-ESO-1 protein and CpG in Montanide induces integrated antibody/Th1 responses and CD8 T cells through cross-priming. Proc Natl Acad Sci U S A. 2007;104(21):8947–52.
Acknowledgments
This work was supported by BiondVax Pharmaceuticals Ltd., Israel who was involved in all stages of the study conduct and analysis. Funding was provided by both BiondVax Pharmaceuticals Ltd. and the Office of the Chief Scientist, the Ministry of Industry, Trade and Labor, Israel. All authors had full access to the data and had final responsibility in submitting such for publication. We thank BEI Resources, Manassas, VA, USA for providing the influenza virus strains used in this study.
Conflicts of Interest
Dr. Tamar Ben-Yedidia is the leader of the vaccine development project, and Mrs. Efrat Kate-Ilovitz and Mr. Yossi Singer are employees of BiondVax Pharmaceuticals Ltd.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Atsmon, J., Kate-Ilovitz, E., Shaikevich, D. et al. Safety and Immunogenicity of Multimeric-001—a Novel Universal Influenza Vaccine. J Clin Immunol 32, 595–603 (2012). https://doi.org/10.1007/s10875-011-9632-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10875-011-9632-5