
Abstract
Purpose
Over 40% of newly diagnosed metastatic breast cancer patients are ≥ 70 years old; however, this population is less likely to be represented in clinical trials. The objective of this study was to analyze PFS, dose reductions, dose delays, and toxicity in a geriatric population receiving palbociclib in a non-trial setting.
Methods
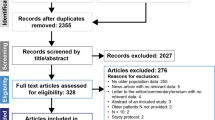
Patients with metastatic breast cancer receiving palbociclib in any line of therapy were identified from a cohort of 845 patients at a large academic institution. Dose delays, dose reductions, and toxicities were retrospectively extracted from the medical record. Data were analyzed using Fischer’s exact test for categorized variables and T test/Wilcoxon rank-sum test for continuous variables. PFS and OS were analyzed using the Kaplan–Meier method.
Results
605 patients who met eligibility criteria were included. 160 patients were ≥ 65 years old and 92 patients were ≥ 70 years old. Patients ≥ 70 had a significantly increased number of dose reductions (p = 0.03) and dose delays (p = 0.02) compared to the younger patients. There was no significant increase in toxicities, including neutropenic fever, infections, or hospitalizations, in the ≥ 70 cohort (p = 0.3). The ≥ 70 cohort had a significantly improved PFS as compared to the younger cohort (p = 0.02); however, age was no longer a significant variable in the multivariate analysis.
Conclusions
Palbociclib was well tolerated in the geriatric population and there was no difference in PFS between older and younger patients. These results are reassuring as palbociclib becomes the frontline standard of care therapy for patients.


Similar content being viewed by others


References
Herrera AP, Snipes SA, King DW, Torres-Vigil I, Goldberg DS, Weinberg AD (2010) Disparate inclusion of older adults in clinical trials: priorities and opportunities for policy and practice change. Am J Public Health 100(Suppl 1):S105–S112
Shenoy P, Harugeri A (2015) Elderly patients’ participation in clinical trials. Perspect Clin Res 6(4):184–189
Mitchell AP, Harrison MR, George DJ et al (2014) Clinical trial subjects compared to “real world” patients: generalizability of renal cell carcinoma trials. J Clin Oncol 32:6510–6510
Watts G (2012) Why the exclusion of older people from clinical research must stop. BMJ 344:e3445
American Cancer Society Cancer Facts & Figs (2017) Supplemental Data. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/breast-cancer-facts-and-figures/breast-cancer-facts-and-figures-2017-2018.pdf. Accessed 12 Jan 2018
Mariotto AB, Etzioni R, Hurlbert M et al (2017) Estimation of the number of women living with metastatic breast cancer in the United States. Cancer Epidemiol Biomark Prev 26(6):809–815
Howlader N, Altekruse SF, Li CI et al (2014) US incidence of breast cancer subtypes defined by joint hormone receptor and HER2 status. J Natl Cancer Inst 106(5):dju055
Reinert T, Barrios CH (2015) Optimal management of hormone receptor positive metastatic breast cancer in 2016. Ther Adv in Med Oncol 7(6):304–320
Wolff A (2016) CDK4 and CDK6 inhibition in breast cancer—a new standard. N Engl J Med 375:1993–1994
Fry DW, Harvey PJ, Keller PR et al (2004) Specific inhibition of cyclin-dependent kinase 4/6 by PD 0332991 and associated antitumor activity in human tumor xenografts. Mol Cancer Ther 3:1427–1438
Finn RS, Dering J, Conklin D et al (2009) PD 0332991, a selective cyclin D kinase 4/6 inhibitor, preferentially inhibits proliferation of luminal estrogen receptor-positive human breast cancer cell lines in vitro. Breast Cancer Res 11:R77–R77
Finn RS, Crown JP, Lang I et al (2015) The cyclin-dependent kinase 4/6 inhibitor palbociclib in combination with letrozole versus letrozole alone as first-line treatment of oestrogen receptor-positive, HER2-negative, advanced breast cancer (PALOMA-1/TRIO-18): a randomised phase 2 study. Lancet Oncol 16:25–35
Finn RS, Martin M, Rugo HS et al (2016) Palbociclib and letrozole in advanced breast cancer. N Engl J Med 375:1925–1936
Turner NC, Ro J, André F et al (2015) Palbociclib in hormone-receptor-positive advanced breast cancer. N Engl J Med 373:209–219
Cristofanilli M, Turner NC, Bondarenko I et al (2016) Fulvestrant plus palbociclib versus fulvestrant plus placebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous endocrine therapy (PALOMA-3): final analysis of the multicentre, double-blind, phase 3 randomised controlled trial. Lancet Oncol 17(4):425–439
Verma S, Bartlett CH, Schnell P et al (2016) Palbociclib in combination with fulvestrant in women with hormone receptor-positive/HER2-negative advanced metastatic breast cancer: detailed safety analysis from a multicenter, randomized, placebo-controlled, phase III study (PALOMA-3). Oncologist 21(10):1165–1175
Singh HA US food and drug administration pooled analysis of outcomes of older women with hormone-receptor positive metastatic breast cancer treated with a CDK4/6 inhibitor as initial endocrine based therapy. Presented at 2017 San Antonio Breast Cancer Symposium; Dec 2017; San Antonio, TX
Rugo HS, Turner NC, Finn RS et al (2018) Palbociclib plus endocrine therapy in older women with HR+/HER2- advanced breast cancer: a pooled analysis of randomised PALOMA clinical studies. Eur J Cancer 101:123–133
Yates JW (2001) Comorbidity considerations in geriatric oncology research. CA Cancer J Clin 51(6):329–336
Charlson ME, Pompei P, Ales KL, MacKenzie R (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40:373–383
Finn RS, Crown JP, Ettl J et al (2016) Efficacy and safety of palbociclib in combination with letrozole as first-line treatment of ER-positive, HER2-negative, advanced breast cancer: expanded analyses of subgroups from the randomized pivotal trial PALOMA-1/TRIO-18. Breast Cancer Res 18(1):67
Hu W, Sung T, Jessen BA et al (2016) Mechanistic Investigation of bone marrow suppression associated with palbociclib and its differentiation from cytotoxic chemotherapies. Clin Cancer Res 22(8):2000–2008
Johnson SM, Torrice CD, Bell JF et al (2010) Mitigation of hematologic radiation toxicity in mice through pharmacological quiescence induced by CDK4/6 inhibition. J Clin Invest 120(7):2528–2536
Sammons SL, Top** DL, Blackwell KL. HR+ (2017) HER2− advanced breast cancer and CDK4/6 inhibitors: mode of action, clinical activity, and safety profiles. Curr Cancer Drug Targets 17(7):637–649
Palbociclib (Ibrance) [package insert] (2017) Pfizer, New York
Funding
Dr. Clifton receives research support from T32 CA009666-24.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The following authors report conflicts of interest: Dr. Jennifer Litton—advisory boards and consulting for Pfizer (both uncompensated); research funding for clinical trials from Pfizer. Dr. Meghan Karuturi—consulting for Pfizer. Dr. Debu Tripathy—Novartis: clinical trial support (support paid to the institution), consultant, consulting for Pfizer. Dr. Clifton, Dr. Min, and Jaime Kimmel do not report any conflicts of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
The Institutional Review Board approved this study; informed consent requirement was waived given the retrospective study design.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Clifton, K., Min, Y., Kimmel, J. et al. Progression-free survival (PFS) and toxicities of palbociclib in a geriatric population. Breast Cancer Res Treat 175, 667–674 (2019). https://doi.org/10.1007/s10549-019-05181-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-019-05181-4