
Abstract
Background
Anatomical changes after intestinal resection and the effects of adjuvant treatment for colorectal cancer may lead to gastrointestinal disturbances. The aim of our study was to assess gastrointestinal function using validated health-related quality of life (HRQoL) questionnaires that are able to reliably quantify patients’ symptoms.
Methods
Two hundred and eighty-nine colorectal cancer patients underwent HRQoL assessment preoperatively and at 3,6 and 12 months postoperatively. They were evaluated with the Gastrointestinal Quality of Life Index (GIQLI) [“global” and “symptoms” scales and questions 3 (“bloating”), 4 (“excessive gas”), 6 (“gurgling noises”), 7 (“frequent bowel movements (BMs)”), 30 (“urgent BMs”), 31 (“diarrhea”), 32 (“constipation”), 36 (“uncontrolled stools”)] and the European Organization for Research and Treatment of Cancer (EORTC) modules QLQ-C30 (symptom scales: “constipation” and “diarrhea”) and QLQ-CR29 (symptom scales: “defecation problems,” “incontinence,” and “bloating”).
Results
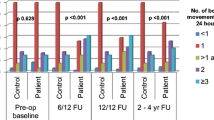
GIQLI “global” and “symptom” indices and the majority of single-item scores and the EORTC QLQ-C30 “constipation” and “diarrhea” subscales showed significant postoperative improvement (p < 0.05). Females and younger age (<70 years) patients appeared to have worse postoperative gastrointestinal function. Rectal cancer patients had more “urgent BMs,” “uncontrolled stools” and worse “global” and “symptom” scores at 3 months and more “diarrhea” at 3 and 6 months than colon cancer patients (p < 0.03). Right colectomy patients had less “excessive passage of gas,” “constipation,” and “uncontrolled stools” than left colectomy patients (3 months, p < 0.01). Anterior resection patients faced more gastrointestinal difficulties, especially in the first 6 months after surgery. Adverse effects related to stage and adjuvant treatment were predominant only at baseline (p < 0.05). GIQLI “diarrhea” and “constipation” scores were correlated with the respective EORTC QLQ-C30 domains (p = 0.0001).
Conclusions
Overall, gastrointestinal function is improved after colorectal cancer surgery. However, women and younger patients are at higher risk of postoperative gastrointestinal dysfunction.

Similar content being viewed by others


References
Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM (2010) Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 127:2893–2917
Schoetz DJ Jr (1991) Postcolectomy syndromes. World J Surg 15:605–608
Ho YH, Low D, Goh HS (1996) Bowel function survey after segmental colorectal resections. Dis Colon Rectum 39:307–310
Beckwith PS, Wolff BG, Frazee RC (1992) Ileorectostomy in the older patient. Dis Colon Rectum 35:301–304
Papa MZ, Karni T, Koller M et al (1997) Avoiding diarrhea after subtotal colectomy with primary anastomosis in the treatment of colon cancer. J Am Coll Surg 184:269–272
Eypasch E, Williams JI, Wood-Dauphinee S et al (1995) Gastrointestinal Quality of Life Index: development, validation and application of a new instrument. Br J Surg 82:216–222
Schwarz R, Hinz A (2001) Reference data for the quality of life questionnaire EORTC QLQ-C30 in the general German population. Eur J Cancer 37:1345–1351
Forgione A, Leroy J, Cahill RA et al (2009) Prospective evaluation of functional outcome after laparoscopic sigmoid colectomy. Ann Surg 249:218–224
Schwenk W, Neudecker J, Haase O et al (2004) Comparison of EORTC quality of life core questionnaire (EORTC QLQ-C30) and gastrointestinal quality of life index (GIQLI) in patients undergoing elective colorectal cancer resection. Int J Colorectal Dis 19:554–560
Maartense S, Dunker MS, Slors JF et al (2006) Laparoscopic-assisted versus open ileocolic resection for Crohn’s disease: a randomized trial. Ann Surg 243:143–149
Fayers PM, Aaronson N, Bjordal K (1999) The EORTC QLQ-C30 Scoring Manual, 2nd edn. European Organization for Research and Treatment of Cancer, Brussels, Belgium
Gujar S, Conroy T, Fleissner C et al (2007) Assessing quality of life in patients with colorectal cancer: an update of the EORTC quality of life questionnaire. Eur J Cancer 43:1564–1573
Whistance RN, Conroy T, Chie W et al (2009) European Organization for the Research and Treatment of Cancer Quality of Life Group. Clinical and psychometric validation of the EORTC QLQ-CR29 questionnaire module to assess health-related quality of life in patients with colorectal cancer. Eur J Cancer 45:3017–3026
Peng J, Shi D, Goodman KA et al (2011) Early results of quality of life for curatively treated rectal cancers in Chinese patients with EORTC QLQ-CR29. Radiat Oncol 6:93
Camilleri-Brennan J, Steele RJ (2001) The impact of recurrent cancer on quality of life. Eur J Surg Oncol 27:349–353
Aaronson NK, Ahmedzai S, Bergman B et al (1993) The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 85:365–372
Schulze T, Wust P, Gellermann J et al (2006) Influence of neoadjuvant radiochemotherapy combined with hyperthermia on the quality of life in rectum cancer patients. Int J Hyperth 22:301–318
Siassi M, Hohenberger W, Lösel F, Weiss M (2008) Quality of life and patient’s expectations after closure of a temporary stoma. Int J Colorectal Dis 23:1207–1212
Sloan JA (2002) Asking the obvious questions regarding patient burden. J Clin Oncol 20:4–6
Sloan J, Symonds T, Vargas-Chanes D, Fridley B (2003) Practical guidelines for assessing the clinical significance of health-related quality of life changes within clinical trials. Drug Inf J 37:23–31
Pescatori M, Anastasio G, Bottini C, Mentasti A (1992) New grading and scoring for anal incontinence. Evaluation of 335 patients. Dis Colon Rectum 35:482–487
Rockwood TH, Church JM, Fleshman JW et al (1999) Patient and surgeon ranking of the severity of symptoms associated with fecal incontinence: the fecal incontinence severity index. Dis Colon Rectum 42:1525–1532
Herschbach P (2002) The ‘Well-being paradox’ in quality-of-life research. Psychother Psychosom Med Psychol 52:141–150
Guillou PJ, Quirke P, Thorpe H et al (2005) Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): multicentre, randomised controlled trial. Lancet 365:1718–1726
Jayne DG, Guillou PJ, Thorpe H, UK MRC CLASICC Trial Group et al (2007) Randomized trial of laparoscopic-assisted resection of colorectal carcinoma: 3-year results of the UK MRC CLASICC Trial Group. J Clin Oncol 25:3061–3068
Ho YH, Wong J, Goh HS (1993) Level of anastomosis and anorectal manometry in predicting function following anterior resection for adenocarcinoma. Int J Colorectal Dis 8:170–174
Horgan FG, O’Connel PR, Shinkwin CA, Kirwan WO (1989) Effect of anterior resection on anal sphincter function. Br J Surg 76:783–786
Dapoigny M, Trolese JK, Bommelaer G, Toumut R (1988) Myoelectric spiking activity of right colon, left colon and rectosigmoid of healthy humans. Dig Dis Sci 33:1007–1012
Speakman CT, Madden MV, Nicholls RJ, Kamm MA (1991) Lateral ligament division during rectopexy causes constipation but prevents recurrence: results of a prospective randomized study. Br J Surg 78:1431–1433
The SCOTIA Study Group (1995) Single-stage treatment for malignant left-sided colonic obstruction: a prospective randomized clinical trial comparing subtotal colectomy with segmental resection following intraoperative irrigation. Subtotal colectomy versus on-table irrigation and anastomosis. Br J Surg 82:1622–1627
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Theodoropoulos, G.E., Papanikolaou, I.G., Karantanos, T. et al. Post-colectomy assessment of gastrointestinal function: a prospective study on colorectal cancer patients. Tech Coloproctol 17, 525–536 (2013). https://doi.org/10.1007/s10151-013-1008-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10151-013-1008-9