
Abstract
Background
Returning to work is a major issue for patients having had an aneurysmal subarachnoid hemorrhage (SAH). It is important, at an early stage, to identify the patients that are unlikely to return to work. The objective of this study was to assess the predictive value of the Montreal Cognitive Assessment (MoCA) at 6 months after ictus on return to work at 12 months.
Methods
In this prospective study were 96 patients with SAH included in the acute phase. Cognitive functions were assessed at 6 months using the MoCA and return to work at 12 months. The predictive value of MoCA on return to work was analyzed using the area under the receiver operating characteristic curve as well as logistic regression.
Results
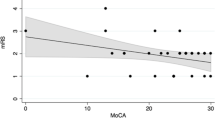
Of those that had work before the SAH, 52 % were working at 12 months after the ictus. These patients had scored significantly better on MoCA at 6 months (p = 0.01). The area under the receiver operating characteristic curve was 0.75. By using a cut-off on MoCA of <27, 68 % of the patients could be correctly classified as returned/not returned to work. Adding data from the acute phase to the MoCA in a logistic regression model increased the percentage of patients correctly classified as returned/not returned to work by 2 %.
Conclusions
Returning to work is a major issue for SAH patients. It is important to identify factors that may interfere with a patient’s ability to return to work, and address these issues appropriately. In our study, estimating cognitive functions at 6 months after SAH using the MoCA alone allowed us to predict return to work correctly in 68 % of the cases. We feel that this provides useful information in planning rehabilitation, but that other post-SAH symptoms have to be considered as well.


Similar content being viewed by others


References
No Author (1988) Report of World Federation of Neurological Surgeons Committee on a Universal Subarachnoid Hemorrhage Grading Scale. J Neurosurg 68(6):985–986
(2009) The Swedish Stroke Register one year follow-up form (Swedish version) http://www.riksstroke.org/sve/riksstroke-rregistreringsplattform/formular/?archived=1. Accessed 26 Sept 2015
Benke T, Koylu B, Delazer M, Trinka E, Kemmler G (2005) Cholinergic treatment of amnesia following basal forebrain lesion due to aneurysm rupture—an open-label pilot study. Eur J Neurol 12:791–796
Fisher CM, Kistler JP, Davis JM (1980) Relation of cerebral vasospasm to subarachnoid hemorrhage visualized by computerized tomographic scanning. Neurosurgery 6:1–9
Hachinski V, Iadecola C, Petersen RC, Breteler MM, Nyenhuis DL, Black SE, Powers WJ, DeCarli C, Merino JG, Kalaria RN, Vinters HV, Holtzman DM, Rosenberg GA, Wallin A, Dichgans M, Marler JR, Leblanc GG (2006) National Institute of Neurological Disorders and Stroke–Canadian Stroke Network vascular cognitive impairment harmonization standards. Stroke 37:2220–2241
Harris C (2014) Factors influencing return to work after aneurysmal subarachnoid hemorrhage. J Neurosci Nurs 46:207–217
Haug T, Sorteberg A, Finset A, Lindegaard KF, Lundar T, Sorteberg W (2010) Cognitive functioning and health-related quality of life 1 year after aneurysmal subarachnoid hemorrhage in preoperative comatose patients (Hunt and Hess Grade V patients). Neurosurgery 66:475–484, discussion 484–475
Johnston SC, Selvin S, Gress DR (1998) The burden, trends, and demographics of mortality from subarachnoid hemorrhage. Neurology 50:1413–1418
Kenny RA, Coen RF, Frewen J, Donoghue OA, Cronin H, Savva GM (2013) Normative values of cognitive and physical function in older adults: findings from the Irish Longitudinal Study on Ageing. J Am Geriatr Soc 61(Suppl 2):S279–290
Kollegger H, Zeiler K, Oder W, Dal-Bianco P, Schmidbauer M, Deecke L (1989) Subarachnoid haemorrhage: prognostic factors as related to working capacity. Int Disabil Stud 11:57–60
Kreiter KT, Copeland D, Bernardini GL, Bates JE, Peery S, Claassen J, Du YE, Stern Y, Connolly ES, Mayer SA (2002) Predictors of cognitive dysfunction after subarachnoid hemorrhage. Stroke 33:200–208
Latimer SF, Wilson FC, McCusker CG, Caldwell SB, Rennie I (2012) Subarachnoid haemorrhage (SAH): long-term cognitive outcome in patients treated with surgical clip** or endovascular coiling. Disabil Rehabil 35:845–850
Mayer SA, Kreiter KT, Copeland D, Bernardini GL, Bates JE, Peery S, Claassen J, Du YE, Connolly ES Jr (2002) Global and domain-specific cognitive impairment and outcome after subarachnoid hemorrhage. Neurology 59:1750–1758
Narazaki K, Nofuji Y, Honda T, Matsuo E, Yonemoto K, Kumagai S (2012) Normative data for the Montreal Cognitive Assessment in a Japanese community-dwelling older population. Neuroepidemiology 40:23–29
Nasreddine ZS, Phillips NA, Bedirian V, Charbonneau S, Whitehead V, Collin I, Cummings JL, Chertkow H (2005) The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc 53:695–699
Passier PE, Visser-Meily JM, Rinkel GJ, Lindeman E, Post MW (2011) Life satisfaction and return to work after aneurysmal subarachnoid hemorrhage. J Stroke Cerebrovasc Dis 20:324–329
Passier PE, Visser-Meily JM, van Zandvoort MJ, Post MW, Rinkel GJ, van Heugten C (2010) Prevalence and determinants of cognitive complaints after aneurysmal subarachnoid hemorrhage. Cerebrovasc Dis 29:557–563
Powell J, Kitchen N, Heslin J, Greenwood R (2004) Psychosocial outcomes at 18 months after good neurological recovery from aneurysmal subarachnoid haemorrhage. J Neurol Neurosurg Psychiatry 75:1119–1124
Powell J, Kitchen N, Heslin J, Greenwood R (2002) Psychosocial outcomes at three and nine months after good neurological recovery from aneurysmal subarachnoid haemorrhage: predictors and prognosis. J Neurol Neurosurg Psychiatry 72:772–781
Pritchard C, Foulkes L, Lang DA, Neil-Dwyer G (2001) Psychosocial outcomes for patients and carers after aneurysmal subarachnoid haemorrhage. Br J Neurosurg 15:456–463
Ryttlefors M, Howells T, Nilsson P, Ronne-Engstrom E, Enblad P (2007) Secondary insults in subarachnoid hemorrhage: occurrence and impact on outcome and clinical deterioration. Neurosurgery 61:704–714, discussion 714–705
Sandvei MS, Mathiesen EB, Vatten LJ, Muller TB, Lindekleiv H, Ingebrigtsen T, Njolstad I, Wilsgaard T, Lochen ML, Vik A, Romundstad PR (2011) Incidence and mortality of aneurysmal subarachnoid hemorrhage in two Norwegian cohorts, 1984–2007. Neurology 77:1833–1839
Schweizer TA, Al-Khindi T, Macdonald RL (2012) Mini-mental state examination versus Montreal Cognitive Assessment: rapid assessment tools for cognitive and functional outcome after aneurysmal subarachnoid hemorrhage. J Neurol Sci 316:137–140
Springer MV, Schmidt JM, Wartenberg KE, Frontera JA, Badjatia N, Mayer SA (2009) Predictors of global cognitive impairment 1 year after subarachnoid hemorrhage. Neurosurgery 65:1043–1050, discussion 1050–1041
Tu QY, ** H, Ding BR, Yang X, Lei ZH, Bai S, Zhang YD, Tang XQ (2013) Reliability, validity, and optimal cutoff score of the Montreal Cognitive Assessment (Changsha version) in ischemic cerebrovascular disease patients of Hunan Province, China. Dement Geriatr Cogn Dis Extra 3:25–36
Vilkki J, Juvela S, Malmivaara K, Siironen J, Hernesniemi J (2012) Predictors of work status and quality of life 9–13 years after aneurysmal subarachnoid hemorrahage. Acta Neurochir (Wien) 154:1437–1446
Wallmark S, Ronne-Engstrom E, Lundstrom E (2014) Prevalence of spasticity after aneurysmal subarachnoid haemorrhage. J Rehabil Med 46:23–27
Wong GK, Lam S, Ngai K, Wong A, Mok V, Poon WS (2012) Evaluation of cognitive impairment by the Montreal Cognitive Assessment in patients with aneurysmal subarachnoid haemorrhage: prevalence, risk factors and correlations with 3 month outcomes. J Neurol Neurosurg Psychiatry 83(11):1112–1117
Wong GK, Lam SW, Wong A, Lai M, Siu D, Poon WS, Mok V (2014) MoCA-assessed cognitive function and excellent outcome after aneurysmal subarachnoid hemorrhage at 1 year. Eur J Neurol 21:725–730
Wong GK, Lam SW, Wong A, Ngai K, Poon WS, Mok V (2013) Comparison of Montreal Cognitive Assessment and mini–mental state examination in evaluating cognitive domain deficit following aneurysmal subarachnoid haemorrhage. PLoS One 8, e59946
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
Erik, Karin and Gösta Selanders Foundation, Hedström’s, Ländell’s and Larsson’s Foundation at Uppsala University provided financial support in the form of grant funding. The sponsors had no role in the design or conduct of this research.
Conflict of interest
The author(s) declare that they have no competing interests.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Wallmark, S., Ronne-Engström, E. & Lundström, E. Predicting return to work after subarachnoid hemorrhage using the Montreal Cognitive Assessment (MoCA). Acta Neurochir 158, 233–239 (2016). https://doi.org/10.1007/s00701-015-2665-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-015-2665-4