
Abstract
Purpose
Although the relationship between preoperative risk factors and outcomes has been extensively studied, the effect of intraoperative hemodynamic changes in a patient’s postoperative course has been less well defined.
Methods
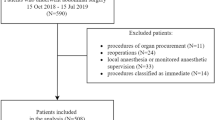
We designed a prospective observational study to assess the impact of several variables, and especially hypotension, on postoperative outcome. Patients considered eligible for the study, all more than 18 years old, were mentally stable patients scheduled for major abdominal surgery with an expected duration of more than 2 h. Total hypotension time (THT), with other variables that possibly influence the outcome, was analyzed using multivariate logistic regression analysis in 100 consecutive patients.
Results
Total hypotension time was isolated as a factor significantly associated with morbidity [odds ratio, 5.1 (1.95–13.35)] and significantly prolonged hospital stay [odds ratio, 4.56 (1.85–10.96)]. Patients who had prolonged THT presented more complications (50 vs. 30), especially of the cardiovascular, pulmonary, and gastrointestinal systems. These complications led to delayed hospital discharge in a significant number of patients (36 with THT vs. 17 others). Finally, duration of surgery was associated with postoperative complications [odds ratio, 3.1 (1.2–8.0)].
Conclusion
Persistent hypotension during elective major abdominal surgery is a significant risk factor for postoperative complications and may prolong hospitalization and affect patient outcomes. Anesthetic management for the avoidance of hypotension, as much as possible, during major abdominal surgery may positively affect outcomes.
Similar content being viewed by others


References
Fleisher LA, Anderson GF. Perioperative risk: how can we study the influence of provider characteristics? Anesthesiology. 2002;96:1039–41.
Monk T, Saini V, Weldon B, Sigl JC. Anesthetic management and one-year mortality after non-cardiac surgery. Anesth Analg. 2005;100:4–10.
Charlson ME, Pompei P, Ales KL, Mackenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies development and validation. J Chron Dis. 1987;40:373–83.
** F, Chung F. Minimizing perioperative adverse events in the elderly. Br J Anaesth. 2001;87:608–24.
Fasting S, Gisvold SE. Serious intraoperative problems: a five year review of 83,844 anesthetics. Can J Anaesth. 2002;49:545–53.
Fowkes FG, Lunn JN, Farrow SC, Robertson IB, Samuel P. Epidemiology in anaesthesia. III. Mortality risk in patients with coexisting physical disease. Br J Anaesth. 1982;54:819–25.
Hallan S, Molaug PO, Arnulf V, Gisvold SE. Causes and risk factors of intraoperative anesthesia complications. A prospective study of 14,735 anaesthesias. Tidsskr Nor Laegeforen. 1990;110:38–41.
Sigurdsson GH, McAteer E. Morbidity and mortality associated with anaesthesia. Acta Anaesthesiol Scand. 1996;40:1057–63.
Arbous MS, Grobbee DE, van Kleef JW, de Lange JJ, Spoormans HH, Touw P, Werner FM, Meursing AE. Mortality associated with anaesthesia: a qualitative analysis to identify risk factors. Anaesthesia. 2001;56:1141–53.
Reich DL, Bennett-Guerrero E, Bodian CA, Hossain S, Winfree W, Krol M. Intraoperative tachycardia and hypertension are independently associated with adverse outcome in non-cardiac surgery of long duration. Anesth Analg. 2002;95:273–7.
Nortcliffe SA, Buggy DJ. Implications of anesthesia for infection and wound healing. Int Anesthesiol Clin. 1992;41:201–20.
Badner NH, Knill RL, Brown JE, Novick TV, Gelb AW. Myocardial infarction after noncardiac surgery. Anesthesiology. 1998;88:572–8.
Reich DL, Wood RK Jr, Emre S, Bodian CA, Hossain S, Krol M, Feirman D. Association of intraoperative hypotension and pulmonary hypertension with adverse outcomes after orthotopic liver transplantation. J Cardiothorac Vasc Anesth. 2003;17:699–702.
Charlson ME, MacKenzie CR, Gold JP, Ales KL, Topkins M, Fairclough GP Jr, Shires GT. The preoperative and intraoperative hemodynamic predictors of postoperative myocardial infarction or ischemia in patients undergoing noncardiac surgery. Ann Surg. 1989;210:637–48.
Jain U, Laflamme CJ, Aggarwal A, Ramsay JG, Comunale ME, Ghoshal S, Ngo L, Ziola K, Hollemberg M, Mangano DT. Electrocardiographic and hemodynamic changes and their association with myocardial infarction during coronary artery bypass surgery. Anesthesiology. 1997;86:576–91.
Williams-Russo P, Sharrock NE, Mattis S, Liguori GA, Mancuso C, Peterson MG, Hollenberg J, Ranawat C, Salvati E, Sculco T (1999) Randomized trial of hypotensive epidural anesthesia in older persons. Anaesthesiology. 91:926–35.
Charlson ME, Mackenzie CR, Gold JP, Ales KM, Topkins M, Shires GT. Preoperative characteristics predicting intraoperative hypotension and hypertension among hypertensives and diabetics undergoing non cardiac surgery. Ann Surg. 1990;212:66–81.
Coldman L, Caldera DL. Risks of general anesthesia and elective operation in the hypertensive patient. Anesthesiology. 1979;50:285–92.
Gullen DJ, Apolone G, Greenfeeld S, Guadagnoli E, Cleary P. ASA physical status and age predict morbidity after three surgical procedures. Ann Surg. 1994;220:3–9.
Fisher JD. New York Heart Association classification. Arch Intern Med. 1972;129:836.
Reich DL, Hossain S, Krol M, Baez B, Patel P, Bernstein A, Bodian CA. Predictors of hypotension after induction of general anesthesia. Anesth Analg. 2005;101:622–8.
Bijker JB, van Klei WA, Kappen TH, van Wolfswinken L, Moons KG, Kalkman CJ. Incidence of intraoperative hypotension as a function of the chosen definition. Literature definitions applied to a retrospective cohort using automated data collection. Anesthesiology. 2007;107:213–20.
Gibson S, Farrell M. A review of age in the neurophysiology of nociception and the perpetual experience of pain. Clin J Pain. 2004;4:227–38.
Altman DG. Practical statistics for medical research. London: Chapman & Hall; 1991. p. 74–106.
Bennet-Guerrero E, Welsby I, Dunn TJ, Young LR, Wahl TI, Diers TL, Phillips-Bute BG, Newman MF, Mythen MG. The use of a postoperative morbidity survey to evaluate patients with prolonged hospitalization after routine, moderate risk, elective surgery. Anesth Analg. 1999;89:514–9.
Vacanti C, Van Houten R, Hill R. A statistical analysis of the relationship of physical status to postoperative morbidity in 68,388 cases. Anesth Analg. 1970;49:564–6.
Mc Bride WT, Armstrong MA, Mc Bride SJ. Immunomodulation: an important concept in modern anaesthesia. Anaesthesia. 1996;51:465–73.
Mythen MG, Web AR. The role of gut mucosal hypoperfusion in the pathogenesis of post-operative organ dysfunction. Intensive Care Med. 1994;20:203–9.
Carli F. Perioperative factors influencing surgical morbidity: what the anesthesiologist needs to know. Can J Anesth. 1999;46:R70–9.
Salo M. Effects of anaesthesia and surgery on the immune response. Acta Anaesth Scand. 1992;36:201–20.
Grozier TA, Muller JE, Quittkat D, Sydow M, Wuttke W, Kettler D. Effects of anaesthesia on the cytokine response to abdominal surgery. Br J Anaesth. 1994;72:280–5.
Kudoh A, Katagai H, Takazawa T, Matsuki A. Plasma proinflammatory cytokine response to surgical stress in elderly patients. Cytokine. 2001;15:270–3.
Kehlet H. Modification of responses to surgery by neural blockade: clinical implications. In: Cousins MJ, Bridenbaugh PO, editors. Neural blockade in clinical anesthesia and management of pain. 3rd ed. Philadelphia: Lippincott; 1998. p. 129–71.
Liu SS, Carpenter RL, Neal JM. Epidural anesthesia and analgesia. Their role in postoperative outcome. Anesthesiology. 1995;82:1474–506.
Moiniche S, Hjorts NC, Hansen BL, Dahl JB, Rosenberg J, Gebuhr P, Kehlet H. The effect of balanced analgesia on early convalescence after major orthopaedic surgery. Acta Anaesth Scand. 1994;38:328–35.
Christensen T, Kehlet H. Postoperative fatigue. World J Surg. 1993;17:220–5.
Kehlet H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth. 1997;78:606–17.
Kehlet H, Dahl JB. Anaesthesia, surgery, and challenges in postoperative recovery. Lancet. 2003;362:1921–28.
De Camp MM, Demling R. Posttraumatic multisystem organ failure. JAMA. 1988;260:530–4.
Hamilton-Davies C, Mythen MG, Salmon JB, Jacobson D, Shukla A, Webb AR. Comparison of commonly used clinical indicators of hypovolemia with gastrointestinal tonometry. Intensive Care Med. 1997;23:276–81.
Marik PE. Gastric intramucosal pH: a better predictor of multiorgan dysfunction syndrome and death than oxygen-derived variables in patients with sepsis. Chest. 1993;104:225–9.
Chang MC, Cheatham ML, Nelson LD, Ratherford EJ, Morris JA Jr. Gastric tonometry supplements information provided by systemic indicators of oxygen transport. J Trauma. 1994;37:488–94.
Acknowledgments
The authors acknowledge E. Zintzaras, MSc, PhD, Assoc. Professor of Biomaths and Biometry in the University of Thessaly, for his key role in the study design, data management, and statistical analysis.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Tassoudis, V., Vretzakis, G., Petsiti, A. et al. Impact of intraoperative hypotension on hospital stay in major abdominal surgery. J Anesth 25, 492–499 (2011). https://doi.org/10.1007/s00540-011-1152-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-011-1152-1