
Abstract
Background
Malnutrition and anorexia are common in children with chronic kidney disease (CKD) and gastrostomy tubes (GT) as well as nasogastric tubes (NGT) have been recommended to maximize nutritional support. The optimal requirement of vitamin C in children with CKD remains to be defined but oxalate is a breakdown product of vitamin C. Elevated vitamin C intake and bone oxalate were identified in two formula-fed dialyzed children with negative genetic testing for primary hyperoxaluria.
Methods
We evaluated the impact of nutritional support on serum ascorbic acid and plasma oxalate levels in 13 dialyzed infants and young children.
Results
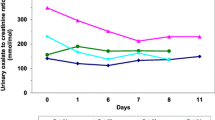
All patients were fed by GT or NGT since the first months of life; overall patients were receiving between 145 and 847% of the age-specific DRI for vitamin C. Mean serum ascorbic acid and plasma oxalate levels were elevated (244.7 ± 139.7 μM/L and 44.3 ± 23.1 μM/L, respectively), and values did not differ according to the degree of residual kidney function. Ascorbic acid levels did not correlate with oxalate levels (r = 0.44, p = 0.13).
Conclusions
Excessive vitamin C intake may contribute to oxalate accumulation in dialyzed children.


Similar content being viewed by others


References
KDOQI Work Group (2009) KDOQI clinical practice guideline for nutrition in children with CKD: 2008 update. Executive summary. Am J Kidney Dis 53(3 Suppl 2):S11–S104
Warady BA, Neu AM, Schaefer F (2014) Optimal care of the infant, child, and adolescent on dialysis: 2014 update. Am J Kidney Dis 64(1):128–142
Sullivan JF, Eisenstein AB (1972) Ascorbic acid depletion during hemodialysis. JAMA. 220(13):1697–1699
Blumberg A, Hanck A, Sander G (1983) Vitamin nutrition in patients on continuous ambulatory peritoneal dialysis (CAPD). Clin Nephrol 20(5):244–250
National Kidney Foundation (2009) KDOQI clinical practice guideline for nutrition in children with CKD: 2008 update. Am J Kidney Dis:S11–S104
Cochat P, Rumsby G (2013) Primary hyperoxaluria. N Engl J Med 369(7):649–658
Balcke P, Schmidt P, Zazgornik J, Kopsa H, Haubenstock A (1984) Ascorbic acid aggravates secondary hyperoxalemia in patients on chronic hemodialysis. Ann Intern Med 101(3):344–345
Hoppe B, Kemper MJ, Bokenkamp A, Langman CB (1998) Plasma calcium-oxalate saturation in children with renal insufficiency and in children with primary hyperoxaluria. Kidney Int 54(3):921–925
Ott SM, Andress DL, Sherrard DJ (1986) Bone oxalate in a long-term hemodialysis patient who ingested high doses of vitamin C. Am J Kidney Dis 8(6):450–454
National Kidney Foundation (2005) KDOQI clinical practice guidelines for bone metabolism and disease in children with chronic kidney disease. Am J Kidney Dis:S1–S122
Ladwig PM, Liedtke RR, Larson TS, Lieske JC (2005) Sensitive spectrophotometric assay for plasma oxalate. Clin Chem 51(12):2377–2380
Sirover WD, Liu Y, Logan A, Hunter K, Benz RL, Prasad D et al (2015) Plasma ascorbic acid concentrations in prevalent patients with end-stage renal disease on hemodialysis. J Ren Nutr 25(3):292–300
Salusky IB, Coburn JW, Brill J, Foley J, Slatopolsky E, Fine RN et al (1988) Bone disease in pediatric patients undergoing dialysis with CAPD or CCPD. Kidney Int 33(5):975–982
National Kidney Foundation (2006) KDOQI clinical practice guidelines for hemodialysis adequacy, update 2006. Am J Kidney Dis:S2–S90
National Kidney Foundation (2006) KDOQI clinical practice guidelines for peritoneal dialysis adequacy, update 2006. Am J Kidney Dis:S91–S97
Bhasin B, Urekli HM, Atta MG (2015) Primary and secondary hyperoxaluria: understanding the enigma. World J Nephrol 4(2):235–244
Knight J, Madduma-Liyanage K, Mobley JA, Assimos DG, Holmes RP (2016) Ascorbic acid intake and oxalate synthesis. Urolithiasis. 44(4):289–297
Hatch M, Mulgrew S, Bourke E, Keogh B, Costello J (1980) Effect of megadoses of ascorbic acid on serum and urinary oxalate. Eur Urol 6(3):166–169
Thomas LD, Elinder CG, Tiselius HG, Wolk A, Akesson A (2013) Ascorbic acid supplements and kidney stone incidence among men: a prospective study. JAMA Intern Med 173(5):386–388
Liu Y, Weisberg LS, Langman CB, Logan A, Hunter K, Prasad D et al (2016) Plasma oxalate levels in prevalent hemodialysis patients and potential implications for ascorbic acid supplementation. Clin Biochem 49(15):1133–1139
Bacchetta J, Boivin G, Cochat P (2015) Bone impairment in primary hyperoxaluria: a review. Pediatr Nephrol 31:1–6. https://doi.org/10.1007/s00467-015-3048-z
Marangella M, Vitale C, Petrarulo M, Tricerri A, Cerelli E, Cadario A et al (1995) Bony content of oxalate in patients with primary hyperoxaluria or oxalosis-unrelated renal failure. Kidney Int 48(1):182–187
Benhamou CL, Bardin T, Tourliere D, Voisin L, Audran M, Edouard C et al (1991) Bone involvement in primary oxalosis. Study of 20 cases. Rev Rhum Mal Osteoartic 58(11):763–769
Bacchetta J, Boivin G, Cochat P (2016) Bone impairment in primary hyperoxaluria: a review. Pediatr Nephrol 31(1):1–6
Hopp K, Cogal AG, Bergstralh EJ, Seide BM, Olson JB, Meek AM et al (2015) Phenotype-genotype correlations and estimated carrier frequencies of primary hyperoxaluria. Clin J Am Soc Nephrol 26(10):2559–2570
Fidler MC, Davidsson L, Zeder C, Walczyk T, Hurrell RF (2003) Iron absorption from ferrous fumarate in adult women is influenced by ascorbic acid but not by Na2EDTA. Br J Nutr 90(6):1081–1085
Wapnick AA, Bothwell TH, Seftel H (1970) The relationship between serum ion levels and ascorbic acid stores in siderotic Bantu. Br J Haematol 19(2):271–276
Deved V, Poyah P, James MT, Tonelli M, Manns BJ, Walsh M et al (2009) Ascorbic acid for anemia management in hemodialysis patients: a systematic review and meta-analysis. Am J Kidney Dis 54(6):1089–1097
Finkelstein FO, Juergensen P, Wang S, Santacroce S, Levine M, Kotanko P et al (2011) Hemoglobin and plasma vitamin C levels in patients on peritoneal dialysis. Perit Dial Int 31(1):74–79
Gastaldello K, Vereerstraeten A, Nzame-Nze T, Vanherweghem JL, Tielemans C (1995) Resistance to erythropoietin in iron-overloaded haemodialysis patients can be overcome by ascorbic acid administration. Nephrol Dial Transplant 10(Suppl 6):44–47
Levine M, Rumsey SC, Daruwala R, Park JB, Wang Y (1999) Criteria and recommendations for vitamin C intake. JAMA 281(15):1415–1423
Richter A, Kuhlmann MK, Seibert E, Kotanko P, Levin NW, Handelman GJ (2008) Vitamin C deficiency and secondary hyperparathyroidism in chronic haemodialysis patients. Nephrol Dial Transplant 23(6):2058–2063
Jackson P, Loughrey CM, Lightbody JH, McNamee PT, Young IS (1995) Effect of hemodialysis on total antioxidant capacity and serum antioxidants in patients with chronic renal failure. Clin Chem 41(8 Pt 1):1135–1138
Kallner A, Hartmann D, Hornig D (1979) Steady-state turnover and body pool of ascorbic acid in man. Am J Clin Nutr 32(3):530–539
Levine M, Padayatty SJ, Espey MG (2011) Vitamin C: a concentration-function approach yields pharmacology and therapeutic discoveries. Adv Nutr 2(2):78–88
Hornig D (1975) Distribution of ascorbic acid, metabolites and analogues in man and animals. Ann N Y Acad Sci 258:103–118
Blanchard J, Tozer TN, Rowland M (1997) Pharmacokinetic perspectives on megadoses of ascorbic acid. Am J Clin Nutr 66(5):1165–1171
Levine M, Conry-Cantilena C, Wang Y, Welch RW, Washko PW, Dhariwal KR et al (1996) Vitamin C pharmacokinetics in healthy volunteers: evidence for a recommended dietary allowance. Proc Natl Acad Sci U S A 93(8):3704–3709
Morena M, Cristol JP, Bosc JY, Tetta C, Forret G, Leger CL et al (2002) Convective and diffusive losses of vitamin C during haemodiafiltration session: a contributive factor to oxidative stress in haemodialysis patients. Nephrol Dial Transplant 17(3):422–427
Bohm V, Tiroke K, Schneider S, Sperschneider H, Stein G, Bitsch R (1997) Vitamin C status of patients with chronic renal failure, dialysis patients and patients after renal transplantation. Int J Vitam Nutr Res 67(4):262–266
Raimann JG, Levin NW, Craig RG, Sirover W, Kotanko P, Handelman G (2013) Is vitamin C intake too low in dialysis patients? Semin Dial 26(1):1–5
Frei B, England L, Ames BN (1989) Ascorbate is an outstanding antioxidant in human blood plasma. Proc Natl Acad Sci U S A 86(16):6377–6381
Kriley M, Warady BA (1991) Vitamin status of pediatric patients receiving long-term peritoneal dialysis. Am J Clin Nutr 53(6):1476–1479
Funding
This work was supported in part by USPHS grants DK-67563 and DK-35423, and CTSI grant UL1 TR-000124 and funds from the UCLA Children’s Discovery and Innovation Institute and from the Casey Lee Ball Foundation. The above were not involved in the study design, collection, and analysis; interpretation of data; writing of the report; or the decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The UCLA Institutional Review Board approved the review of medical records.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kennedy, S.S., Perilloux, A., Pereira, R.C. et al. Vitamin C overload may contribute to systemic oxalosis in children receiving dialysis. Pediatr Nephrol 36, 435–441 (2021). https://doi.org/10.1007/s00467-020-04702-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-020-04702-4