
Abstract
Aims and objectives
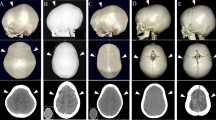
Isolated sagittal synostosis can be diagnosed easily on clinical grounds. This study was designed to determine if children could be operated on based solely on a clinical diagnosis or whether such an approach would result in any potentially unnecessary surgeries.
Materials and methods
Records of 114 consecutive children operated on for isolated nonsyndromic sagittal synostosis over a 14-year period (1987–2000) were reviewed to see whether the clinical findings were in concordance with the intraoperative findings and histopathology of the sagittal suture.
Results
The age at surgery ranged from 1.9 to 81.3 months (median 4.3 months). Preoperative skull radiographs were done in 78 children and computer tomography (CT) scans of the head in 12 children. One hundred percent of the skull radiographs and 83.3% of the CT scans were completed prior to referring the children to a pediatric neurosurgeon. CT scans confirmed the diagnosis in all patients in whom it was available. For the rest, pathology reports and/or operative records were available for 108 (94.7%) children and were confirmatory for sagittal craniosynostosis in all.
Conclusions
Accurate diagnosis of isolated sagittal synostosis can be made clinically, and operative correction can proceed without a need for radiological investigations, unless the clinical features are not completely typical. This approach could result in significantly reduced radiation exposure for the develo** brain and could provide economic benefits to health care providers.
Similar content being viewed by others


References
von Baer KE (1860) Die Macrocephalen im Boden der Krym und Osterreichs, verglichen mit der Bildungs-atweichung, welche Blumrnback Macrocephalus genannt hat. Mém Acad Imp Sci St-Pétersbg 7(6):2
Baumgartner JE, Seymour-Dempsey K, Teichgraeber JF, **a JJ, Waller AL, Gateno J (2004) Nonsynostotic scaphocephaly: the so-called sticky sagittal suture. J Neurosurg 101:16–20
Brenner D, Elliston C, Hall E, Berdon W (2001) Estimated risks of radiation-induced fatal cancer from pediatric CT. Am J Roentgenol 176:289–296
Brenner DJ, Elliston CD, Hall EJ, Berdon WE (2001) Estimates of the cancer risks from pediatric CT radiation are not merely theoretical: comment on “Point/counterpoint: in x-ray computed tomography, technique factors should be selected appropriate to patient size. Against the proposition”. Med Phys 28:2387–2388
Brenner DJ (2002) Estimating cancer risks from pediatric CT: going from the qualitative to the quantitative. Pediatr Radiol 32:223–228; discussion: 242–224
Furuya Y, Edwards MS, Alpers CE, Tress BM, Norman D, Ousterhout DK (1984) Computerized tomography of cranial sutures. Part 2: abnormalities of sutures and skull deformity in craniosynostosis. J Neurosurg 61:59–70
Hall P, Adami HO, Trichopoulos D, Pedersen NL, Lagiou P, Ekbom A, Ingvar M, Lundell M, Granath F (2004) Effect of low doses of ionising radiation in infancy on cognitive function in adulthood: Swedish population based cohort study. BMJ 328:19
Kabbani H, Raghuveer TS (2004) Craniosynostosis. Am Fam Physician 69:2863–2870
Medina LS (2000) Three-dimensional CT maximum intensity projections of the calvaria: a new approach for diagnosis of craniosynostosis and fractures. Am J Neuroradiol 21:1951–1954
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Agrawal, D., Steinbok, P. & Cochrane, D.D. Diagnosis of isolated sagittal synostosis: are radiographic studies necessary?. Childs Nerv Syst 22, 375–378 (2006). https://doi.org/10.1007/s00381-005-1243-0
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-005-1243-0