
Abstract
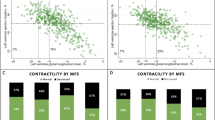
We explored the influence of global longitudinal strain (GLS) measured with two-dimensional speckle-tracking echocardiography on left ventricular mass regression (LVMR) in patients with pure aortic stenosis (AS) and normal left ventricular function undergoing aortic valve replacement (AVR). The study population included 83 patients with severe AS (aortic valve area <1 cm2) treated with AVR. Bioprostheses were implanted in 58 patients (69.8 %), and the 25 remaining patients (30.2 %) received mechanical prostheses. Peak systolic longitudinal strain was measured in four-chamber (PLS4ch), two-chamber (PLS2ch), and three-chamber (PLS3ch) views, and global longitudinal strain was obtained by averaging the peak systolic values of the 18 segments. Median follow-up was 66.6 months (interquartile range 49.7–86.3 months). At follow-up, values of PLS4ch, PLS2ch, PLS3ch, and GLS were significantly lower (less negative) in patients who did not show left ventricular (LV) mass regression (all P < 0.001). Baseline global strain was the strongest predictor of lack of LVMR (odds ratio 3.5 (95 % confidence interval 3.0–4.9), P < 0.001), and GLS value ≥−9.9 % predicted lack of LVMR with 95 % sensitivity and 87 % specificity (P < 0.001). Other multivariable predictors were the preoperative LV mass value (cutoff value ≥147 g/m2, P < 0.001), baseline effective orifice area index (cutoff ≤0.35 cm2/m2, P = 0.01), and baseline mean gradient (cutoff ≥58 mmHg, P = 0.01). Finally, we failed to find interactions between GLS and other significant parameters (all P < 0.05). Global longitudinal strain accurately predicts LV mass regression in patients with pure AS undergoing AVR. Our findings must be confirmed by further larger studies.




Similar content being viewed by others

References
Grossman W (1980) Cardiac hypertrophy: useful adaptation or pathologic process? Am J Med 69:576–584
Frohlich ED, Apstein C, Chobanian AV, Devereux RB, Dustan HP, Dzau V, Fauad-Tarazi F, Horan MJ, Marcus M, Massie B (1992) The heart in hypertension. N Engl J Med 327:998–1008
Aurigemma GP, Silver KH, McLaughlin M, Mauser J, Gaasch WH (1994) Impact of chamber geometry and gender on left ventricular systolic function in patients >60 years of age with aortic stenosis. Am J Cardiol 74:794–798
Ballo P, Mondillo S, Motto A, Faraguti SA (2006) Left ventricular midwall mechanics in subjects with aortic stenosis and normal systolic chamber function. J Heart Valve Dis 15:639–650
Cramariuc D, Cioffi G, Rieck AE, Devereux RB, Staal EM, Ray S, Wachtell K, Gerdts E (2009) Low-flow aortic stenosis in asymptomatic patients: valvular-arterial impedance and systolic function from the SEAS Substudy. JACC Cardiovasc Imaging 2:390–399
Aurigemma GP, Silver KH, Priest MA, Gaasch WH (1995) Geometric changes allow normal ejection fraction despite depressed myocardial shortening in hypertensive left ventricular hypertrophy. J Am Coll Cardiol 26:195–202
Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP (1990) Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. N Engl J Med 322:1561–1566
Wakabayashi K, Tsu**o T, Naito Y, Ezumi A, Lee-Kawabata M, Nakao S, Goda A, Sakata Y, Yamamoto K, Daimon T, Masuyama T (2011) Administration of angiotensin-converting enzyme inhibitors is associated with slow progression of mild aortic stenosis in Japanese patients. Heart Vessels 26:252–257
Vahanian A, Baumgartner H, Bax J, Butchart E, Dion R, Filippatos G, Flachskampf F, Hall R, Iung B, Kasprzak J, Nataf P, Tornos P, Torracca L, Wenink A, Task Force on the management of valvular hearth disease of the European Society of Cardiology, ESC Committee for Practice Guidelines (2007) Guidelines on the management of valvular heart disease: The Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology. Eur Heart J 28:230–268
Breitenbach I, Harringer W, Tsui S, Amorim MJ, Herregods M, Bogaert J, Goiti J, Gerosa G (2011) Magnetic resonance imaging versus echocardiography to ascertain the regression of left ventricular hypertrophy after bioprosthetic aortic valve replacement: results of the REST study. J Thorac Cardiovasc Surg. doi:10.1016/j.jtcvs
Notomi Y, Lysyansky P, Setser RM, Shiota T, Popovic ZB, Martin-Miklovic MG, Weaver JA, Oryszak SJ, Greenberg NL, White RD, Thomas JD (2005) Measurement of ventricular torsion by two-dimensional ultrasound speckle tracking imaging. J Am Coll Cardiol 45:2034–2041
Cho GY, Chan J, Leano R, Strudwick M, Marwick TH (2006) Comparison of two-dimensional speckle and tissue velocity based strain and validation with harmonic phase magnetic resonance imaging. Am J Cardiol 97:1661–1666
D’Andrea A, Caso P, Romano S, Scarafile R, Riegler L, Salerno G, Limongelli G, Di Salvo G, Calabrò P, Del Viscovo L, Romano G, Maiello C, Santangelo L, Severino S, Cuomo S, Cotrufo M, Calabrò R (2007) Different effects of cardiac resynchronization therapy on left atrial function in patients with either idiopathic or ischaemic dilated cardiomyopathy: a two-dimensional speckle strain study. Eur Heart J 28:2738–2748
Cianciulli TF, Saccheri MC, Lax JA, Bermann AM, Ferreiro DE (2010) Two-dimensional speckle tracking echocardiography for the assessment of atrial function. World J Cardiol 26:163–170
Akins CW, Miller DC, Turina MI, Kouchoukos NT, Blackstone EH, Grunkemeier GL, Takkenberg JJ, David TE, Butchart EG, Adams DH, Shahian DM, Hagl S, Mayer JE, Lytle BW (2008) Councils of the American Association for Thoracic Surgery; Society of Thoracic Surgeons; European Association for Cardio-Thoracic Surgery; Ad Hoc Liaison Committee for Standardizing Definitions of Prosthetic Heart Valve Morbidity. Guidelines for reporting morbidity and mortality after cardiac valvular interventions. J Thorac Cardiovasc Surg 135:732–738
Sahn DJ, DeMaria A, Kisslo J, Weyman A (1978) Recommendation regarding quantitation in M-mode echocardiography: results of survey of echocardiographic measurements. Circulation 58:1072–1081
Devereux RB, Alonso DR, Lutas EM, Gottlieb GJ, Campo E, Sachs I, Reichek N (1986) Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. Am J Cardiol 57:450–458
Schiller NB, Shah PM, Crawford M, DeMaria A, Devereux R, Feigenbaum H, Gutgesell H, Reichek N, Sahn D, Schnittger I (1989) Recommendations for quantitation of the left ventricle by two-dimensional echocardiography. American Society of Echocardiography Committee on Standards, Subcommittee on Quantitation of Two-Dimensional Echocardiograms. J Am Soc Echocardiogr 2:358–367
Aurigemma GP, Douglas PS, Gaash WH (1997) Quantitative evaluation of left ventricular structure, wall stress and systolic function. In: Otto CM (ed.) The practice of clinical echocardiography. Saunders, Philadelphia, pp 1–24
Bonow RO, Carabello BA, Kanu C, de Leon AC Jr, Faxon DP, Freed MD, Gaasch WH, Lytle BW, Nishimura RA, O’Gara PT, O’Rourke RA, Otto CM, Shah PM, Shanewise JS, Smith SC Jr, Jacobs AK, Adams CD, Anderson JL, Antman EM, Fuster V, Halperin JL, Hiratzka LF, Hunt SA, Page RL, Riegel B (2006) ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to revise the 1998 Guidelines for the Management of Patients with Valvular Heart Disease): developed in collaboration with the Society of Cardiovascular Anesthesiologists: endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. Circulation 114:e84–e231
Romesburg HC (2004) Cluster analysis for researchers. Lulu Press, Morrisville, pp 1–330
Chambers J (2006) The left ventricle in aortic stenosis: evidence for the use of ACE inhibitors. Heart 92:420–433
Koren MJ, Devereux RB, Casae PN, Savage DD, Laragh JH (1991) Relation of left ventricular mass and geometry to morbidity and mortality in uncomplicated essential hypertension. Ann Intern Med 114:345–352
Levy D (1991) Clinical significance of left ventricular hypertrophy: insights from the Framingham study. J Cardiovasc Pharmacol 17(Suppl 2):S1–S6
Ghali JK, Liao Y, Simmons B, Castaner A, Cao G, Cooper RS (1992) The prognostic role of left ventricular hypertrophy in patients with or without coronary artery disease. Ann Intern Med 117:831–836
Kannel WB, Dannenberg AL, Levy D (1987) Population implications of echocardiographic left ventricular hypertrophy. Am J Cardiol 60:851–893
Ruel M, Al-Faleh H, Kulik A, Chan KL, Mesana TG, Burwash JG (2006) Prosthesis-patient mismatch after aortic valve replacement predominantly affects patients with pre-existing left ventricular dysfunction: effect on survival, freedom from heart failure, and left ventricular mass regression. J Thorac Cardiovasc Surg 131:1036–1044
Fuster RG, Montero Argudo JA, Albarova OG, Sos FH, López SC, Codoñer MB, Buendía Miñano JA, Albarran IR (2005) Patient-prosthesis mismatch in aortic valve replacement: really tolerable? Eur J Cardiothorac Surg 27:441–449
Toggweiler S, Zuber M, Gerber K, Schläpfer R, Erne P, Stulz P (2009) Left ventricular mass regression following implantation of MIRA bileaflet valves in patients with severe aortic stenosis. Heart Vessels 24:37–40
Kühl HP, Franke A, Puschmann D, Schöndube FA, Hoffmann R, Hanrath P (2002) Regression of left ventricular mass one year after aortic valve replacement for pure severe aortic stenosis. Am J Cardiol 89:408–413
De Paulis R, Sommariva L, Colagrande L, De Matteis GM, Fratini S, Tomai F, Bassano C, Penta de Peppo A, Chiariello L (1998) Regression of left ventricular hypertrophy after aortic valve replacement for aortic stenosis with different valve substitutes. J Thorac Cardiovasc Surg 116:590–598
Ali A, Patel A, Ali Z, Abu-Omar Y, Saeed A, Athanasiou T, Pepper J (2011) Enhanced left ventricular mass regression after aortic valve replacement in patients with aortic stenosis is associated with improved long-term survival. J Thorac Cardiovasc Surg 142:285–291
Weidemann F, Jamal F, Sutherland GR, Claus P, Kowalski M, Hatle L, De Scheerder I, Bijnens B, Rademakers FE (2002) Myocardial function defined by strain rate and strain during alterations in inotropic states and heart rate. Am J Physiol Heart Circ Physiol 283:H792–H799
Weidemann F, Jamal F, Kowalski M, Kukulski T, D’hooge J, Bijnens B, Hatle L, De Scheerder I, Sutherland GR (2002) Can strain rate and strain quantify changes in regional systolic function during dobutamine infusion, β-blockade, and atrial pacing-implications for quantitative stress echocardiography. J Am Soc Echocardiogr 15:416–424
Korinek J, Wang J, Sengupta PP, Miyazaki C, Kjaergaard J, McMahon E, Abraham TP, Belohlavek M (2005) Two-dimensional strain-A Doppler-independent ultrasound method for quantitation of regional deformation: validation in vitro and in vivo. J Am Soc Echocardiogr 18:1247–1253
Kim H, Shin HW, Son J, Yoon HJ, Park HS, Cho YK, Han CD, Nam CW, Hur SH, Kim YN, Kim KB (2011) Two-dimensional strain or strain rate findings in mild to moderate diastolic dysfunction with preserved ejection fraction. Heart Vessels 26:39–45
Fang LL, Zhang PY, Wang C, Wang LM, Ma XW, Shi HW, Feng XH (2011) Two-dimensional strain combined with adenosine stress echocardiography assessment of viable myocardium. Heart Vessels 26:206–213
Miyazaki S, Daimon M, Miyazaki T, Onishi Y, Koiso Y, Nishizaki Y, Ichikawa R, Chiang SJ, Makinae H, Suzuki H, Daida H (2011) Global longitudinal strain in relation to the severity of aortic stenosis: a two-dimensional speckle-tracking study. Echocardiography 28:703–708
Cramariuc D, Gerdts E, Davidsen ES, Segadal L, Matre K (2010) Myocardial deformation in aortic valve stenosis: relation to left ventricular geometry. Heart 96:106–112
Delgado V, Tops LF, van Bommel RJ, van der Kley F, Marsan NA, Klautz RJ, Versteegh MI, Holman ER, Schalij MJ, Bax JJ (2009) Strain analysis in patients with severe aortic stenosis and preserved left ventricular ejection fraction undergoing surgical valve replacement. Eur Heart J 30:3037–3047
Sensky PR, Loubani M, Keal RP, Samani NJ, Sosnowski AW, Galiñanes M (2003) Does the type of prosthesis influence early left ventricular mass regression after aortic valve replacement? Assessment with magnetic resonance imaging. Am Heart J 146:e13
Weidemann F, Herrmann S, Störk S, Niemann M, Frantz S, Lange V, Beer M, Gattenlöhner S, Voelker W, Ertl G, Strotmann JM (2009) Impact of myocardial fibrosis in patients with symptomatic severe aortic stenosis. Circulation 120:577–584
Krayenbuehl HP, Hess OM, Monrad ES, Schneider J, Mall G, Turina M (1989) Left ventricular myocardial structure in aortic valve disease before, intermediate and late after aortic valve replacement. Circulation 79:744–755
Del Rizzo DF, Abdoh A, Cartier P, Doty D, Westaby S (1999) Factors affecting left ventricular mass regression after aortic valve replacement with stentless valves. Semin Thorac Cardiovasc Surg 11(Suppl 1):114–120
Uwabe K, Kitamura M, Hachida M, Endo M, Hashimoto A, Koyanagi H (1995) Long-term outcome of left ventricular dysfunction after surgery for severe aortic stenosis. J Heart Valve Dis 4:503–507
Lund O, Emmertsen K, Nielsen TT, Jensen FT, Flo C, Pilegaard HK, Rasmussen BS, Hansen OK, Kristensen LH (1997) Impact of size mismatch and left ventricular function on performance of the St. Jude disc valve after aortic valve replacement. Ann Thorac Surg 63:1227–1234
Lim E, Ali A, Theodorou P, Sousa I, Ashrafian H, Chamageorgakis T, Duncan A, Henein M, Diggle P, Pepper J (2008) Longitudinal study of the profile and predictors of left ventricular mass regression after stentless aortic valve replacement. Ann Thorac Surg 85:2026–2029
Maselli D, Pizio R, Bruno LP, Di Bella I, De Gasperis C (1999) Left ventricular mass reduction after aortic valve replacement: homografts, stentless and stented valves. Ann Thorac Surg 67:966–971
Gelsomino S, Frassani R, Morocutti G, Nucifora R, Da Col P, Minen G, Morelli A, Livi U (2001) Time course of left ventricular remodeling after stentless aortic valve replacement. Am Heart J 142:556–562
Katz J, Milliken MC, Stray Gundersen J, Buja LM, Parkey RW, Mitchell JH, Peshock RM (1988) Estimation of human myocardial mass with MR imaging. Radiology 169:495–498
Gopal AS, Schnellbaecher MJ, Shen Z, Akinboboye OO, Sapin PM, King DL (1997) Freehand three-dimensional echocardiography for measurement of left ventricular mass: in vivo anatomic validation using explanted human hearts. J Am Coll Cardiol 30:802–810
Acknowledgments
We gratefully acknowledge Dr Judith Wilson for the English revision of the paper. Our heartfelt thanks are extended to Marco Di Stefano and Marco Dardi from EMAC/TOMTEC for their valuable suggestions and technical support.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gelsomino, S., Lucà, F., Parise, O. et al. Longitudinal strain predicts left ventricular mass regression after aortic valve replacement for severe aortic stenosis and preserved left ventricular function. Heart Vessels 28, 775–784 (2013). https://doi.org/10.1007/s00380-012-0308-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00380-012-0308-8