
Abstract
Background
Nipple inversion is a relatively common problem in adolescent and adult women; however, most present surgical treatments are prone to injure the lactiferous ducts and impair the breast feeding function. A nipple retractor was developed by us in 2003 to correct nipple inversion to avoid lactiferous duct injury. The details and a 10-year evaluation of this technique were introduced in this paper.
Methods
The nipple retractor was made from the hollow end of single-use syringe, then eight holes were punctured for sutures crossing the base, and the height of retractor depended on the sizes of nipple-areola complex and breast volume. Two sutures were made to cross beneath the base of the nipple to elevate the nipple, and the hollow retractor was placed on the areola with the nipple and four ends of the sutures in the center, sutures then passed the prefabricated holes on the retractor base and were fixed with knots and suitable tension. The retractor was worn for 3–6 months and then could be removed.
Results
A total of 257 nipples in 136 patients with nipple inversion (unilateral: 15 patients; bilateral: 121 patients) received this operation from Jan 2003 to Dec 2012, among which 233 nipples were successfully corrected (90.7 %), and 24 nipples reoccurred in 2 years. The effective rates of grade I and grade II inversions were significantly higher than that of grade III (P < 0.01). Thirty-two patients with 56 treated nipples underwent labor and breastfeeding, and all the nipples were functional. The complications included fistula after suture removal (19 nipples, 7.4 %), breaking of suture (8 nipples, 3.1 %), erosion of nipple (28 nipples, 10.9 %), and chronic pain (10 nipples, 3.4 %), and all these complications were properly managed.
Conclusion
The nipple retractor technique is a feasible, effective, and safe method for correction of grade I and grade II nipple inversions, and could also be indicated for primary correction of grade III inversion. Its most significant advantage is that lactiferous duct injury can be avoided and the breast feeding function preserved.
Level of Evidence V
Nipple inversion is a common malformation in adolescent and adult women, which can be present unilaterally or bilaterally. It was generally initiated from the adolescent period and could be caused by primary hypogenesis of smooth muscle and supporting tissue of the nipple-areola complex or hypoplasia of lactiferous ducts [1] . Some other secondary factors such as chronic infection, tumor, and previous surgery could contribute to the fibrosis, and some of them were believed to be congenital and hereditary [2, 3]. Since the openings of lactiferous ducts are immersed, inversion might cause reoccurring infection and breast feeding difficulty, and the appearance of the breast would be affected as well, which would impact patients’ psychological health.
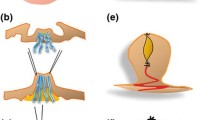
Nipple inversion can be clinically divided into three categories according to Han et al.’s grading rules. In grade I, the nipple is easily pulled out manually and maintains its projection quite well. In grade II, the nipples can be pulled out but cannot maintain projection and tend to go back again. In grade III, the nipple can hardly be pulled out manually. [4] The images of three grades of nipple inversion are present in Fig. 1.

Three categories of nipple inversion grade I inverted nipple(a), grade II inverted nipple(b), grade III inverted nipple(c)
Surgical interventions are the most effective treatments at present; however, injury to lactiferous ducts is inevitable in most surgical techniques [1, 5–10]. Some conservative nonoperative techniques have been developed in the last several years, such as a self-retraction and suction device, but only mild cases of grade I are indicated. Several suspension and retraction devices have been reported in recent years [10, 11], and the effect was acceptable, but long-term results were not reported.
To simplify the operation procedures and diminish the possibility of lactiferous duct injury, we developed a nipple retractor, which was made from a single-use syringe, to correct nipple inversion from 2003. The details of procedures and techniques are introduced in this paper, as well as a 10-year retrospective analysis.







Similar content being viewed by others


References
Schwager RG, Smith JW, Gray GF, Goulian D Jr (1974) Inversion of the human female nipple, with a simple method of treatment. Plast Reconstr Surg 54(5):564–569
Park HS, Yoon CH, Kim HJ (1999) The prevalence of congenital inverted nipple. Aesthet Plast Surg 23(2):144–146
Shafir R, Bonne-Tamir B, Ashbell S et al (1979) Genetic studies in a family with inverted nipple (mammillae invertita). Clin Genet 15:346–350
Han S, Hong YG (1999) The inverted nipple: its grading and surgical correction. Plast Reconstr Surg 104(2):389–395
Megumi Y (1991) Correction of inverted nipple with periductal fibrous flaps. Plast Reconstr Surg 88(2):342–346
Chandler PJ Jr, Hill SD (1990) A direct surgical approach to correct the inverted nipple. Plast Reconstr Surg 86(2):352–354
Teimourian B, Adham MN (1980) Simple technique for correction of inverted nipple. Plast Reconstr Surg 65(4):504–506
Hartrampe CR Jr, Schneider WJ (1976) A simple direct method for correction of inversion of the nipple. Plast Reconstr Surg 58(6):678–679
Caviggioli F, Ventura D, Andretto Amodeo C, Klinger F (2008) Inverted nipple: use of an effective and personalized splint after surgical correction with Pitanguy’s technique to avoid relapse of the inversion in 28 cases. Plast Reconstr Surg 121(3):139e–140e
Shiau JP, Chin CC, Lin MH, Hsiao CW (2011) Correction of severely inverted nipple with telescope method. Aesthet Plast Surg 35(6):1137–1142
Kolker AR, Torina PJ (2009) Minimally invasive correction of inverted nipples: a safe and simple technique for reliable, sustainable projection. Ann Plast Surg 62(5):549–553
Mcgeorge DD (1994) The “Niplette”: an instrument for the non-surgical correction of inverted nipples. Br J Plast Surg 47(1):46–49
Chin HHAT (2006) Usefulness of the nipple-suspension piercing device after correction of inverted nipples. Aesthetic Plast Surg 30(4):396–398
Zhao XLR (2011) Nipple retractor to correct inverted nipples. Breast Care 6:463–465
Mu D, Luan J, Mu L, **n MA (2012) Minimally invasive gradual traction technique for inverted nipple correction. Aesthet Plast Surg 36(5):1151–1154
Teng L, Wu GP, Sun XM, Lu JJ, Ding B, Ren M, Ji Y, ** XL (2005) Correction of inverted nipple: an alternative method using continuous elastic outside distraction. Ann Plast Surg 54:120–123
Li W, Wu Y, Deng Y et al (2016) An adjustable-traction technique for correction of inverted nipples. Ann Plast Surg 76(1):29–33
Persichetti P, Poccia I, Pallara T, Delle Femmine PF, Marangi GF (2011) A new simple technique to correct nipple inversion using 2 V-Y advancement flaps. Ann Plast Surg 67(4):343–345
Cabalag MS, Chui CH, Tan BK (2010) Correction of nipple inversion using a micro-knife and transverse to longitudinal skin closure. J Plast Reconstr Aesthet Surg 63(8):e627–e630
Szczerba SM, Paulius KL, Nadimi S, Maguina P (2009) Wire subcision as a treatment for nipple inversion. Plast Reconstr Surg 123(6):206e–207e
Kolker AR, Torina PJ (2009) Minimally invasive correction of inverted nipples: a safe and simple technique for reliable, sustainable projection. Ann Plast Surg 62(5):549–553
Caviggioli F, Ventura D, Andretto Amodeo C, Klinger F (2008) Inverted nipple: use of an effective and personalized splint after surgical correction with Pitanguy’s technique to avoid relapse of the inversion in 28 cases. Plast Reconstr Surg 121(3):139e–140e
Wu HL, Huang X, Zheng SS (2008) A new procedure for correction of severe inverted nipple with two triangular areolar dermofibrous flaps. Aesthet Plast Surg 32(4):641–644
Chen SH, Gedebou T, Chen PH (2007) The endoscope as an adjunct to correction of nipple inversion deformity. Plast Reconstr Surg 119(4):1178–1182
Teng L, Wu GP, Sun XM, Lu JJ, Ding B, Ren M, Ji Y, ** XL (2005) Correction of inverted nipple: an alternative method using continuous elastic outside distraction. Ann Plast Surg 54(2):120–123
Sakai S, Sakai Y, Izawa H (1999) A new surgical procedure for the very severe inverted nipple. Aesthetic Plast Surg 23(2):139–143
Huang WC (2003) A new method for correction of inverted nipple with three periductal dermofibrous flaps. Aesthet Plast Surg 27(4):301–304
Kim DY, Jeong EC, Eo SR, Kim KS, Lee SY, Cho BH (2003) Correction of inverted nipple: an alternative method using two triangular areolar dermal flaps. Ann Plast Surg 51(6):636–640
Stevens WG, Fellows DR, Vath SD, Stoker DA (2004) An integrated approach to the repair of inverted nipples. Aesthet Surg J 24(3):211–215
Gould DJ, Nadeau MH, Macias LH, Stevens WG (2015) Inverted nipple repair revisited: a 7-year experience. Aesthet Surg J 35(2):156–164
Karacaoglu E (2009) Correction of recurrent grade III inverted nipple with antenna dermoadipose flap: case report. Aesthet Plast Surg 33(6):843–848
Pribaz JJ, Pousti T (1998) Correction of recurrent nipple inversion with cartilage graft. Ann Plast Surg 40(1):14–17
Hii-Sun Jeong HL (2015) Correction of inverted nipple using subcutaneous turn-over flaps to create a tent suspension-like effect. PloS One 10(7):e0133588
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest to disclose.
Rights and permissions
About this article

Cite this article
Yukun, L., Ke, G. & Jiaming, S. Application of Nipple Retractor for Correction of Nipple Inversion: A 10-Year Experience. Aesth Plast Surg 40, 707–715 (2016). https://doi.org/10.1007/s00266-016-0675-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00266-016-0675-0