
Abstract
Rationale
Despite decades of research specifying harmful effects produced by 3,4-methylenedioxymethamphetamine (MDMA; a principal component of ‘ecstasy’ pills), young people (and adults) continue to use it. In an attempt to model human MDMA consumption patterns, preclinical investigators have sought to establish reliable patterns of intravenous MDMA self-administration in rodents.
Objective
The objective of this report is to offer a critical review of published data (including our own novel findings) that reveal MDMA self-administration in rodents.
Results
The data indicate that MDMA serves as a reinforcer in rodents, though the responses are not similar to those previously reported for psychostimulants (i.e., cocaine). Important differences between rodent models and human use patterns include frequency of dosing and dosage exposure, routes of administration, tolerance that develops to MDMA after repeated exposure, polydrug use in humans but not by rodents, limits on the repertoire of behaviors that can be exhibited by rodents undergoing IV self-administration procedures, and the question of neurotoxicity as it relates to models of self-administration.
Conclusions
While MDMA is not as potent a reinforcer as other drugs of abuse, the fact remains that young people and adults continue to use the drug, and therefore, additional research is needed to determine why drugs with low reinforcing effects continue to be abused.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
3,4-methylenedioxymethamphetamine (MDMA) is a principal component of ‘ecstasy’ pills and is the second most frequently used illicit drug following marijuana. Among casual ecstasy users, 20% reported ecstasy-related problems and met criteria for abuse or dependence (Schuster et al. 1998).
The unpredictable content of MDMA found in ecstasy pills (discussed below) has contributed to the challenge of characterizing users, though Parrot and colleagues have defined users as either light, moderate or heavy based on lifetime exposure (and frequency of use per week; Parrott 2005). In humans, dependence on MDMA (Jansen 1999) appears to be the exception, not the rule, since the majority of individuals who abuse the drug do so intermittently.
The fact that patterns of MDMA abuse differ from other drugs, such as cocaine and methamphetamine, raises important questions regarding the design of preclinical models of MDMA self-administration, especially those utilizing rodents. An advantage of preclinical research is that the approach facilitates greater experimental control and presumably, permits researchers to offer more definitive conclusions regarding the effects of MDMA on brain and behavior. A common assumption is that preclinical findings can be used to model human consumption patterns and addictive potential of a drug. If this assumption is inaccurate, then it may be worthwhile for preclinical researchers to reconsider the manner in which they conceptualize rodent models of MDMA reinforcement.
To address this important issue, the principal objective of this review is to offer an analysis of published reports of rodent MDMA self-administration.
Drug discrimination, conditioned place preference (CPP), intracranial self-stimulation (ICSS)
The interoceptive stimulus effects of drugs have been predicted to be relevant to their reinforcing effects and have been measured in drug discrimination assays. MDMA reinforcement has been inferred on the basis of performance in CPP and ICSS paradigms. This information has been expertly reviewed elsewhere (Cole and Sumnall 2003), though a brief summary is provided below.
MDMA engenders a discriminative stimulus and available data specify a role for both serotonin (5-HT) and dopamine (DA) systems in its effects. For example, the DA D1 receptor antagonist SCH 23390, but not the DA D2 antagonist eticlopride, attenuated MDMA drug discrimination (Bubar et al. 2004). The latter result confirmed the outcomes observed in a three-choice discrimination paradigm in which the DA D2 antagonist haloperidol did not alter MDMA drug discrimination (Goodwin and Baker 2000). In the same study, the authors found that the hallucinogen lysergic acid diethylamide (LSD) produced a near complete substitution for the MDMA stimulus, and that the 5-HT2 antagonist MDL-100,907 partially blocked the MDMA cue (Goodwin and Baker 2000). Of interest, a recent report demonstrated that stimulus generalization to MDMA occurred in the presence of cocaine (Khorana et al. 2004), and these data may help to explain why MDMA is self-administered in animals previously exposed to cocaine (Ratzenboeck et al. 2001).
MDMA has been shown to readily establish CPP in rodents (Bilsky et al. 1991, 1990, 1998). 5-HT and DA systems appear critical for this response since it is blocked by a DA uptake inhibitor (Bilsky et al. 1998) as well as the 5-HT3 antagonist ondansetron (Bilsky and Reid 1991). Other neurotransmitter systems may be important since the nonspecific opioid receptor antagonist naltrexone prevented acquisition of MDMA CPP (Reid et al. 1996).
MDMA has been shown to dose-dependently lower the threshold and increase the response rate of medial forebrain bundle and nucleus accumbens electrical self-stimulation (Hubner et al. 1988; Lin et al. 1997; Reid et al. 1996; Rosecrans and Glennon 1987). The nonspecific 5-HT receptor antagonist methysergide blocked the self-stimulation response-rate-increasing effects, but not the threshold lowering effects of MDMA (Lin et al. 1997). In addition, the δ-opioid receptor antagonist naltrindole prevented the increase in MDMA-induced self-stimulation response rate (Reid et al. 1996).
Drug discrimination, CPP, and ICSS assays are useful for determining some of the behavioral and rewarding effects produced by MDMA. Notwithstanding, intravenous (IV) self-administration is considered the most valid model predictive of the reinforcing effects of drugs and has been used with success to determine the abuse potential and pharmacological properties of several drugs of abuse in animals, including cocaine, heroin, morphine, and nicotine (Koob et al. 1994; Schuster and Thompson 1969). As such, IV self-administration is the major focus of the current review.
IV self-administration of MDMA
Preclinical investigators have sought to establish reliable patterns of IV MDMA self-administration in monkeys (Fantegrossi et al. 2002, 2004b) and rodents. In this section, we review all published data (including our own novel findings) that reveal MDMA self-administration in rodents.
Zernig and colleagues
In the first report of MDMA self-administration in rodents (Ratzenboeck et al. 2001), animals had to fulfill acquisition criteria for food-reinforced responding (100+responses/23 h on an fixed ratio (FR)-1 schedule) before implantation with IV catheters and being advanced to MDMA testing. MDMA was reported to be a reinforcer in 63% of animals tested. While novel, the report did not engender much enthusiasm since animals took only three to four infusions of MDMA during a 2-h session. The reinforcing effects produced by MDMA did not differ between drug-naive and cocaine-trained rats. Additional data suggested that MDMA and cocaine produced distinct interoceptive stimuli in these rats.
De La Garza and colleagues
In 2002, we initiated a series of experiments in an effort to replicate and extend the findings of Zernig and colleagues. The outcome of these studies has been described previously in preliminary form (De La Garza 2004).
Animals and surgery
The animal care and use committee of the Albert Einstein College of Medicine (AECOM) approved all protocols, and all experiments were conducted at AECOM. The experiments were conducted in accordance with the National Institute of Mental Health—“Methods and Welfare Considerations in Behavioral Research with Animals” report. AECOM is fully accredited by the Association for Assessment and Accreditation of Laboratory Animal Care.
Male Wistar rats (300–375 g; Charles River Labs, Charles River, NC) were individually housed and maintained on a 12-h light/dark cycle, with the light phase being 7:00 a.m. to 7:00 p.m. Room temperature was maintained at 23–25°C, and rats were allowed free access to food and water throughout all experiments. Animals were first trained to press a lever for sucrose pellets on an FR-1 schedule of reinforcement and subsequently scheduled for IV catheter implant surgery. The self-administration apparatus and experimental parameters have been described in detail elsewhere (De La Garza 2005).
Results: experiment 1
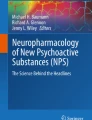
In the first experiment, male, Wistar rats (N=5; Charles River Labs), were trained to press a lever for MDMA (0.75 mg/kg, IV) using an FR-2 schedule of reinforcement. Animals were tested for self-administration behavior once daily (Monday–Friday) for 3 h per session over a period of 5 weeks (24 sessions). The data revealed that average responding for the group was 3.6±0.4 infusions (inf) per session, with an average MDMA exposure of 2.7±0.4 mg per session per rat (Fig. 1). Inactive lever pressing was of similar or greater magnitude to that of the active lever (data not shown).

MDMA (0.75 mg/kg, IV) self-Administration in Wistar rats. Data represent Mean (±S.E.M.) of total infusions taken during daily 3-h acquisition and maintenance sessions (filled circles) for four (sessions 20–14) or five (sessions 1–19) subjects at each time point. Substitution tests (open circles) with MDMA (0.1875 mg/kg, IV) are shown at sessions 14 and 16
Individual responses were consistently low in four of five rats. In contrast, responding that was initially low for rat W-1 increased considerably over time (Fig. 2). In this animal, challenge with a lower dose of MDMA (0.375 mg/kg) on session 25 resulted in a 100% increase in responding, and challenge with a higher dose of MDMA (1.5 mg/kg) on session 27 resulted in a 50% reduction in responding. On the basis of evidence showing that MDMA inhibits neuronal firing in raphe nuclei by stimulating 5-HT1A autoreceptors (Sprouse et al. 1989), and that MDMA generalized to a 8-OH-DPAT (5-HT1A agonist) discriminative stimulus (Glennon and Young 2000), we investigated the effects of 8-OH-DPAT on MDMA responding. 8-OH-DAT preexposure (30 min prior to test) on session 31 completely eliminated responding at 0.1 mg/kg, s.c., and was without effect at 0.01 mg/kg, s.c. on session 33. The potential role of 5-HT1A receptors in mediating this reinforcement behavior is questionable since the 0.1 mg/kg dose altered baseline locomotor activity and is predicted to have interfered with responding. Given that this experiment consisted of only one animal, this cannot be considered adequate for establishing the role of 5-HT1A receptors in MDMA-mediated reinforcement. Recent evidence suggests that the reinforcing effects produced by MDMA are more likely mediated through 5-HT2A receptors (Fantegrossi et al. 2002), though we were unable to test that hypothesis in this group of animals.

MDMA (0.75 mg/kg, IV) self-administration in Wistar rat W-1 only. Data represent total infusions taken during daily 3-h sessions (filled circles). Substitution tests (open symbols) include MDMA (0.1875 mg/kg, IV; circles), MDMA (0.375 mg/kg, IV; square), MDMA (1.50 mg/kg, IV; up triangle), and DPAT (0.1 mg/kg, s.c.; down triangle) or DPAT (0.01 mg/kg, s.c.; diamond) administered 30 min prior to the training dose of MDMA (0.75 mg/kg, IV; down triangle) are shown
Discussion: experiment 1
A number of important findings emerged from this preliminary study. First, we replicated, to some extent, the findings in the original rodent study (Ratzenboeck et al. 2001), showing that rats self-administered approximately three infusions of MDMA per session (group average over time). Second, in one animal, MDMA served as a reinforcer. Overall, however, the pattern of responding for MDMA in this group of rats was not consistent with that observed for drugs like cocaine.
Experiment 2
We noted somewhat profound behavioral effects of the 0.75 mg/kg IV dose, including flat body posture and forward locomotion, which prompted us to consider a lower dose of MDMA that might prove more efficacious as a reinforcer and less prone to disrupt behavior.
In the second experiment, male Wistar rats (N=15, 300–375 g) were trained to press a lever for MDMA at 0.375 mg/kg, IV. For sessions 1–8, animals were tested during the inactive phase of their light/dark cycle (Fig. 3, cycle: light). During this time period, the mean MDMA exposure was 1.1±0.3 mg per session per rat. The individual data revealed a range of responding from high (10.3/session) to very low (0.5/session). Responding that exceeded five responses per session was observed in only 2 of the 15 animals tested (<15%). Rats were classified as high or low responders based on a median split of average infusions administered per session (data not shown), though this analysis did not reveal unique profiles of responding.

MDMA (0.375 mg/kg, IV) self-administration in Wistar rats. Data represent Mean (±S.E.M.) of total infusions taken during daily 3-h sessions for 13–15 rats during the inactive portion of the dark/light cycle (cycle: light, sessions 1–8: open circles), or during the active portion of the dark/light cycle (cycle: dark, sessions 9–27: filled circles). Substitution tests with MDMA (0.1875 mg/kg, IV: gray square) and saline (1 mg/ml, IV: gray circles) are also shown
We also tested animals during the active phase of their light/dark cycle (Fig. 3, cycle: dark) and extended the duration of access from 3 h to include the entire 12-h cycle. Beginning on session 9, responding increased to 9.3±1.3 inf/session during the next 7 sessions. A substitution test with a lower dose of MDMA (0.1875 mg/kg) on session 16 elicited approximately 50% of previous responding (5.3±0.7), contrary to our expectation that it would result in increased responding. Responding for the full dose of MDMA never returned to pretest levels. On sessions 24 and 25, substitution tests with saline engendered mean responses of 4.5±0.9 and 1.8±0.6, respectively. Animals did not return to pretest level responding during subsequent sessions (sessions 26 and 27). Attrition occurred during the experiment and was largely the result of blocked catheters. As a whole, responses during the active portion of the light/dark cycle (sessions 9–27) were greater in magnitude (5.5±0.6/session) though the rate of responding (∼0.5 inf/h) was lower than the shorter session specified in Experiment 1 (∼1.2 inf/h). Because of the longer access period, the mean dose exposure was higher for these animals (2.1±0.3 mg per session per rat). Inactive lever pressing in this experiment was of similar or greater magnitude to that of the active lever (data not shown).
Discussion: experiment 2
The end result of this experiment was largely similar to the first, with responding for MDMA that did not exceed saline and therefore does not provide conclusive evidence establishing MDMA as a potent reinforcer in rodents. Overall, this outcome is in agreement with other researchers who have stated that MDMA has rewarding properties but is only a weak reinforcer (Cole and Sumnall 2003).
Schenk and colleagues
In 2003, Schenk and colleagues published a report demonstrating MDMA self-administration in drug-naïve and cocaine-exposed rodents, highlighting the addictive potential of MDMA (Schenk et al. 2003). Similar to our approach, drug-naïve rats received 26 daily tests, and group sizes and doses tested were comparable. Halving of the training dose (in an effort to increase responding) was used by these researchers, as in our experiment, though with dissimilar outcomes. The outcomes of this study included very low inactive lever responding, and dose-dependent responding for MDMA.
In a subsequent report, Schenk and colleagues reported on the role of DA in MDMA self-administration and hyperactivity (Daniela et al. 2004). In this report, the training dose of MDMA was 1.0 mg/kg and experiments were conducted daily during 2-hr tests sessions. As before, the outcomes of this study revealed dose-dependent responding for MDMA.
The experimental procedures described by Schenk and colleagues are distinct from those specified in the current report, and these may contribute to the unique profiles of responding (Table 1). These include a long infusion time, no time out, and sessions that are generally long during acquisition (6 hr). These procedural differences might not be trivial. For example, it is well-established that cocaine self-administration is dependent on infusion time, with shorter infusions being associated with increased self-administration behavior in animals and increased subjective effects in humans (as compared to long infusions) (Nelson et al. 2005; Samaha and Robinson 2005). While rapid infusion rates may increase self-administration of cocaine, it is possible that slower delivery of MDMA is integral to its ability to serve as a reinforcer in rodents.
McGregor and colleagues
In 2003, a novel report highlighted the importance of temperature on the reinforcing effects produced by self-administered MDMA (Cornish et al. 2003). The authors reported a shallow dose response for MDMA responding, and inactive lever pressing data and acquisition data were not shown. The principal finding was that hot temperature (30°C as opposed to 21°C) increased the number of MDMA infusions self-administered by rats. The data indicate that hot temperatures altered both the social and reinforcing effects of MDMA.
Other approaches to measure reinforcement
In a recent report, Zernig and colleagues highlighted the limited data available on the reinforcing effects of MDMA provided in lever-pressing operant conditioning procedures (Wakonigg et al. 2003). They specified that “we have been approached by several colleagues who tried, in vain, to replicate our [previous] results (Ratzenboeck et al. 2001)...” [and that] “this was a matter of concern for us.” As a result, they investigated MDMA reinforcement in rats using a runway procedure, originally developed by Ettenberg (Geist and Ettenberg 1990). In this paradigm, the faster that a rat runs to obtain an injection is predicted to reflect the reinforcing effects of the drug. In the report, MDMA (1 mg/kg, IV) served as a positive reinforcer in male Sprague–Dawley and Long Evans rats, though differences were apparent in the onset and offset of effects between strains. In Sprague–Dawley rats, by the fifth trial (after exposure to five doses of 1 mg/kg MDMA), the reinforcing effects had diminished and approached levels similar to that produced by saline (which may reflect tolerance that developed as a result of repeated exposure). In contrast, at this point, Long Evans rats continued to respond for MDMA.
Concerns about current models of rodent MDMA self-Administration
No animal model of self-administration can ever be expected to be a perfect replica of the human disease condition (abuse or dependence). Yet, it is important to address and eliminate as many potential differences to obtain as accurate a representation as possible. Differences between rodent models and human use patterns include frequency of dosing and dosage exposure, routes of administration, tolerance that develops to MDMA after repeated exposure, polydrug use in humans but not by rodents, limits on the repertoire of behaviors that can be exhibited by rodents undergoing IV self-administration procedures, and the question of neurotoxicity as it relates to models of self-administration.
Frequency of dosing and dosage exposure
Unlike rodent models that routinely employ once daily self-administration sessions, humans do not typically consume MDMA with the same predictable frequency. Parrott (2005) has separated users into three broad categories: Novice, Moderate or Heavy. These categories distinguish users on the basis of average dose of ecstasy consumption on a given occasion and highest number of ecstasy tablets used in 1 week. This effort is an extension of previous work which separated users according to lifetime use: Low (1–99), Medium (100–499), and High (500+; Fox et al. 2001). The newest data reveal that the significant majority of all users [novice (100%), moderate (84%), and heavy (62%)] consume 1–2 tablets of ecstasy on any given occasion. This corroborates a previous report indicating a mean consumption of 1.8 tablets on a Saturday night (Parrott and Lasky 1998). Based on the assumption that ecstasy pills contain 70 mg MDMA on average (see below), the mean consumption by a 70-kg human is approximated to be 1.8 mg/kg. This estimation raises an important question: How does this value compare with the results of rodent models of MDMA self-administration?
The data in Table 1 reveal that studies by Zernig, De La Garza, and McGregor resulted in daily dosage exposure comparable to a dose of MDMA (1.5 mg/kg) which has been shown to produce a number of subjective effects in humans (Liechti et al. 2000) and is the same dose self-administered by monkeys (Fantegrossi et al. 2004b). In contrast, the daily infusion quantities reported by Schenk and colleagues (17.5–25 mg/kg; Daniela et al. 2004; Schenk et al. 2003) are 10–15 times greater than other rodent studies (and that observed in monkey studies and in humans) and are similar to dosage exposure for paradigms previously demonstrated to induce neurotoxicity (see below). Importantly, studies by Zernig, De La Garza, and McGregor resulted in daily dosage exposure comparable to the dose of MDMA used in CPP and drug discrimination studies in rodents (1.5 mg/kg; Glennon et al. 1992; Schechter 1987, 1991).
MDMA pill content
Chemical analyses of ecstasy pills reveal considerable variability in MDMA content, and the World Health Organization has concluded that ecstasy is a generic term for a wide range of compounds. In one report, researchers showed that 63% of ecstasy pills contained some MDMA or 3,4-methylenedioxyamphetamine (MDA), 29% pills contained drugs other than MDMA or MDA (including dextromethorphan, caffeine, ephedrine, pseudoephedrine, and salicylates), and 8% pills contained no identifiable drug (Baggott et al. 2000). MDMA content in ecstasy pills range from 0 to >140 mg. Of interest, average MDMA content per pill has dropped during the past three decades from >100 to ∼70 mg (Parrott 2005). Attempts to equate human ecstasy consumption with IV MDMA self-administration in rodents is plagued by the uncertainty of the impact of other compounds on the propensity of humans to self-administer the drug, potential neurotoxicity, tolerance, and other factors.
Route of administration
One potential concern is that the route of administration used in self-administration studies (IV) is dissimilar to the conventional route of consumption used by humans (oral). In fact, parenteral administration (a manner other than through the digestive tract, including IV or intraperitoneal injection) of MDMA has been predicted to increase toxicity two to three times as opposed to oral intake, and the importance of route and frequency for MDMA has been discussed previously (Ricaurte et al. 1988). For example, 2.5 mg/kg MDMA given orally once every 2 weeks for 4 months did not alter 5-HT and its primary metabolite (5-HIAA) in monkeys, though similar doses given intraperitoneally have been clearly associated with neurotoxicity (Vollenweider et al. 1999). The importance of route remains questionable, however, since it has been specified that these two routes of administration produce comparable effects in rodents (Ricaurte et al. 1988).
Of interest, there is evidence that MDMA is abused via the IV route in humans. For example, 28% of an IV drug-abusing sample reported that they started injecting MDMA because they developed significant tolerance to MDMA via the oral route (Zernig et al. 2003).
Tolerance to MDMA
Tolerance is a common response to repeated use and can be defined as a reduction in response to the drug after repeated administration. This holds true for the subjective effects of MDMA, which have been reported to diminish after repeated exposure in humans (Parrott 2005; von Sydow et al. 2002; Cornish et al. 2003). The characteristic reduction in subjective efficacy upon repeated exposure has led some to predict that MDMA would not become a drug of abuse (Shulgin 1986).
Tolerance has also been reported in preclinical models, including studies performed in monkeys, in which the reinforcing effects of MDMA were attenuated as a result of chronic MDMA self-administration (Fantegrossi et al. 2004b). In contrast, cocaine-maintained behavior remained stable over equivalent time periods, indicating that tolerance after repeated MDMA is not simply a non-selective response decrement. In one model of MDMA self-administration (Ratzenboeck et al. 2001), maximum response rates for MDMA were reported to be higher during a second dose response determination as opposed to the initial dose response determination. In these distinct cases (and likely applicable to the human condition), tolerance may be manifest as decreased responding when a drug loses its reinforcing effects and desire for the drug diminishes, or increased responding as a compensation for these changes in an effort to obtain equivalent positive reinforcing effects.
In the study by Zernig and colleagues (Ratzenboeck et al. 2001), the dose at which maximum responding occurred remained the same for individual animals, and only the rate of responding increased. On the basis of pharmacological considerations detailed elsewhere (Zernig et al. 2004), the change in shape of the MDMA dose–response curve is suggestive of tolerance to the rate-decreasing effects of MDMA (i.e., not due to a reduction in reinforcing effects produced by the drug).
Limits on the repertoire of behaviors that can be exhibited
Humans that exhibit tolerance to ecstasy (greater doses of the drug are needed to achieve the same effects) are more likely than not to switch to other drugs. In the absence of an alternative reinforcer (e.g., cocaine on a third lever) or increased cost (more lever pressing) animals are, for all practical purposes, limited in the repertoire of behaviors they can elicit (animals simply choose to administer the drug or not). Moreover, in rodent MDMA models used to date, there are no negative consequences associated with continued use. This information would be very valuable since it would indicate persistent drug-taking behavior in the presence of environmental adversity (compulsive behavior; Vanderschuren and Everitt 2004).
Polydrug use history in humans
An important difference between preclinical studies and human patterns of ecstasy consumption is polydrug use (Cole and Sumnall 2003). A number of reports indicate that college-aged ecstasy users are more likely to use marijuana, engage in binge drinking, and smoke cigarettes (Gross et al. 2002; Strote et al. 2002). Marijuana exposure likely contributes to a number of prevalent psychobiological symptoms, including psychosis, reported by MDMA users (Milani et al. 2005; Parrott 2004, 2005). For alcohol, a recent preclinical report revealed that MDMA–ethanol interactions may have specific long-term consequences on presynaptic modulation of hippocampal 5-HT release, which is not necessarily related to MDMA-induced depletion of 5-HT (Cassel et al. 2005). The authors speculated that the psychopathological problems reported by ecstasy users drinking alcohol are unlikely to be the sole result of the consumption of MDMA.
Given this information, self-administration models in nonhuman primates are especially advantageous (and very likely preferential) for use since these animals are more likely than not to have extensive drug self-administration histories, including past exposure to other stimulants (Fantegrossi et al. 2002, 2004b; Lile et al. 2005).
Schedules of drug delivery
As specified previously, drugs with high reinforcing efficacy should be expected to maintain behavior across several distinct operant conditioning schedules [progressive ratio (PR), fixed and variable intervals, etc.] and behavioral paradigms. It is well-established that FR schedules provide information regarding the potency of a drug as a reinforcer (Woolverton and Johanson 1984), and when using (pseudo)irreversible antagonists, drug efficacy can also be determined (Zernig et al. 1997). While this procedure has been used with success in models examining other stimulants (e.g., cocaine and amphetamine), MDMA self-administration has not been tested using PR schedules (or other operant conditioning schedules) in rodents.
An additional, and more stringent, test will determine if animals that self-administer MDMA exhibit behaviors that resemble key diagnostic criteria for addiction. This has recently been addressed in rodents that self-administer cocaine, and “addiction-like behavior” was present only in a small proportion of subjects (Deroche-Gamonet et al. 2004). In this study, addiction criteria included difficulty stop** drug use or limiting drug intake measured as persistence of cocaine seeking during a period of signaled nonavailability, motivation to take the drug measured using a progressive-ratio schedule, and continued use of the substance despite harmful consequences measured as the persistence of the animals’ responding for the drug when drug delivery was associated with a punishment. The data showed that while all rats consumed similar quantities of cocaine during self-administration sessions (∼25 mg/kg), the number of animals that met zero, one, two, or all three criteria for addiction-like behavior was 41, 28, 14, and 17%, respectively.
Ecstasy is not a prototypical stimulant
Available evidence indicates that acute MDMA stimulates DA release, repeated MDMA induces behavioral sensitization and cross-sensitization to cocaine, MDMA substitutes for cocaine in a drug discrimination task, and that MDMA preexposure facilitates cocaine CPP and IV self-administration (Cole and Sumnall 2003). Despite these findings, MDMA is not a prototypical stimulant and does not possess the same addictive potential as stimulants like cocaine (Cole and Sumnall 2003). This has been restated recently in work performed in monkeys, in which cocaine and MDMA functioned as reinforcers, but self-administration of MDMA occurred at fewer doses suggesting that the reinforcing efficacy of MDMA was less than cocaine (Lile et al. 2005). Similar outcomes have been reported in rodents. For example, the maximum response produced by MDMA was only 35% of a dose of cocaine that previously engendered maximum rates of responding in rats under the same experimental conditions (Ratzenboeck et al. 2001). In addition, McGregor and colleagues also reported that MDMA maintained lower rates of self-administration than cocaine (Cornish et al. 2003).
The question of neurotoxicity
Young people use drugs for purposes of experimentation, and a majority report that they use drugs to feel good and enhance social activities (Parks and Kennedy 2004). A number of preclinical reports using MDMA have utilized regimens demonstrated to induce 5-HT or DA neurotoxicity. This is a flawed rationale, as the most relevant models of MDMA exposure should be based as closely as possible to known usage patterns in humans. As specified above, this estimate is ∼1.8 mg/kg/session.
In monkeys, a recent report revealed no significant differences in 5-HT, 5-HIAA, DA, or DOPAC between animals that self-administered the drug and control animals (Fantegrossi et al. 2004b). Unfortunately, there are no equivalent reports of neurochemical or neurobiological changes associated with IV MDMA self-administration in rodents. Individual doses of MDMA (10 mg/kg, i.p.) have been shown to decrease 5-HT and [3H]-paroxetine binding sites (which label the 5-HT transporter) in rats, while 5 mg/kg was without effect (Colado et al. 1995). Similarly, a single dose of MDMA (4–15 mg/kg, i.p.) dose-dependently decreased 5-HT and [3H]-paroxetine binding sites in Dark Agouti rats, though lower doses (4 mg/kg, i.p.) were ineffective in inducing similar changes (O’Shea et al. 1998). Also, recent evidence demonstrated that a dosing regimen of MDMA (7.5 mg/kg i.p., every 2 h × 3 doses) that depletes brain 5-HT did not alter 5-HT transporter protein expression or the distribution of 5-HT transporter between endosomes and the plasma membrane and did not produce detectable evidence for neurotoxicity (Wang et al. 2005).
These studies serve as important references and indicate that the self-administration doses in the studies by Zernig, De La Garza, and McGregor are unlikely to have been associated with neurotoxicity, though this may have been the case in studies by Schenk and colleagues.
Summary and conclusions
The available evidence indicates that MDMA serves as a positive reinforcer in rodents, yet the absolute number of animals that exhibit this behavior are a small minority of all subjects tested.
While MDMA is not as potent a reinforcer as other drugs of abuse, the fact remains that young people and adults continue to abuse the drug. This begs the question of why a drug with low reinforcing effects would continue to be used at all. This behavioral output may reflect similar outcomes observed with other drugs (e.g., LSD), which do not have marked reinforcing effects, yet are still abused intermittently (Fantegrossi et al. 2004a). Like LSD, MDMA has direct agonist effects at 5-HT2 receptors, which contributes to its hallucinogenic properties (Aghajanian and Marek 1999), as well as its reinforcing effects (Fantegrossi et al. 2002). Similarly, tetrahydrocannabinnol (THC) is not readily self-administered in animal models, yet is abused by humans. The “transient reinforcing properties” of MDMA and similar drugs are a challenge for preclinical researchers who attempt to model human consumption patterns. Indeed, the sporadic nature of responding (with what appears to be tolerance and reduced responding) may reflect what Fantegrossi et al. (2004a) have dubbed, “mixed reinforcing and aversive effects” produced by the drug.
References
Aghajanian GK, Marek GJ (1999) Serotonin and hallucinogens. Neuropsychopharmacology 21:16S–23S
Baggott M, Heifets B, Jones RT, Mendelson J, Sferios E, Zehnder J (2000) Chemical analysis of ecstasy pills. JAMA 284:2190
Bilsky EJ, Reid LD (1991) MDL72222, a serotonin 5-HT3 receptor antagonist, blocks MDMA’s ability to establish a conditioned place preference. Pharmacol Biochem Behav 39:509–512
Bilsky EJ, Hui YZ, Hubbell CL, Reid LD (1990) Methylenedioxymethamphetamine’s capacity to establish place preferences and modify intake of an alcoholic beverage. Pharmacol Biochem Behav 37:633–638
Bilsky EJ, Hubbell CL, Delconte JD, Reid LD (1991) MDMA produces a conditioned place preference and elicits ejaculation in male rats: a modulatory role for the endogenous opioids. Pharmacol Biochem Behav 40:443–447
Bilsky EJ, Montegut MJ, Nichols ML, Reid LD (1998) CGS 10746B, a novel dopamine release inhibitor, blocks the establishment of cocaine and MDMA conditioned place preferences. Pharmacol Biochem Behav 59:215–220
Bubar MJ, Pack KM, Frankel PS, Cunningham KA (2004) Effects of dopamine D1- or D2-like receptor antagonists on the hypermotive and discriminative stimulus effects of (+)-MDMA. Psychopharmacology (Berl) 173:326–336
Cassel JC, Riegert C, Rutz S, Koenig J, Rothmaier K, Cosquer B, Lazarus C, Birthelmer A, Jeltsch H, Jones BC, Jackisch R (2005) Ethanol, 3,4-methylenedioxymethamphetamine (Ecstasy) and their combination: long-term behavioral, neurochemical and neuropharmacological effects in the rat. Neuropsychopharmacology 30:1870–1882
Colado MI, Williams JL, Green AR (1995) The hyperthermic and neurotoxic effects of ‘Ecstasy’ (MDMA) and 3,4 methylenedioxyamphetamine (MDA) in the Dark Agouti (DA) rat, a model of the CYP2D6 poor metabolizer phenotype. Br J Pharmacol 115:1281–1289
Cole JC, Sumnall HR (2003) The pre-clinical behavioural pharmacology of 3,4-methylenedioxymethamphetamine (MDMA). Neurosci Biobehav Rev 27:199–217
Cornish JL, Shahnawaz Z, Thompson MR, Wong S, Morley KC, Hunt GE, McGregor IS (2003) Heat increases 3,4-methylenedioxymethamphetamine self-administration and social effects in rats. Eur J Pharmacol 482:339–341
Daniela E, Brennan K, Gittings D, Hely L, Schenk S (2004) Effect of SCH 23390 on (+/−)-3,4-methylenedioxymethamphetamine hyperactivity and self-administration in rats. Pharmacol Biochem Behav 77:745–50
De La Garza IR (2004) Neurobiological consequences of MDMA exposure: a 21st century framework. In: Invited mini-symposium presented at the annual meeting of the Society for Neuroscience, San Diego, CA
De La Garza R II (2005) Wistar Kyoto rats exhibit reduced sucrose pellet reinforcement behavior and intravenous nicotine self-administration. Pharmacol Biochem Behav 82:330–337
Deroche-Gamonet V, Belin D, Piazza PV (2004) Evidence for addiction-like behavior in the rat. Science 305:1014–1017
Fantegrossi WE, Ullrich T, Rice KC, Woods JH, Winger G (2002) 3,4-Methylenedioxymethamphetamine (MDMA, “ecstasy”) and its stereoisomers as reinforcers in rhesus monkeys: serotonergic involvement. Psychopharmacology (Berl) 161:356–364
Fantegrossi WE, Woods JH, Winger G (2004a) Transient reinforcing effects of phenylisopropylamine and indolealkylamine hallucinogens in rhesus monkeys. Behav Pharmacol 15:149–157
Fantegrossi WE, Woolverton WL, Kilbourn M, Sherman P, Yuan J, Hatzidimitriou G, Ricaurte GA, Woods JH, Winger G (2004b) Behavioral and neurochemical consequences of long-term intravenous self-administration of MDMA and its enantiomers by rhesus monkeys. Neuropsychopharmacology 29:1270–1281
Fox HC, Parrott AC, Turner JJ (2001) Ecstasy use: cognitive deficits related to dosage rather than self-reported problematic use of the drug. J Psychopharmacol 15:273–281
Geist TD, Ettenberg A (1990) A simple method for studying intravenous drug reinforcement in a runaway. Pharmacol Biochem Behav 36:703–706
Glennon RA, Young R (2000) MDMA stimulus generalization to the 5-HT(1A) serotonin agonist 8-hydroxy-2-(di-n-propylamino)tetralin. Pharmacol Biochem Behav 66:483–488
Glennon RA, Higgs R, Young R, Issa H (1992) Further studies on N-methyl-1(3,4-methylenedioxyphenyl)-2-aminopropane as a discriminative stimulus: antagonism by 5-hydroxytryptamine-3 antagonists. Pharmacol Biochem Behav 43:1099–1106
Goodwin AK, Baker LE (2000) A three-choice discrimination procedure dissociates the discriminative stimulus effects of d-amphetamine and (+/−)-MDMA in rats. Exp Clin Psychopharmacol 8:415–423
Gross SR, Barrett SP, Shestowsky JS, Pihl RO (2002) Ecstasy and drug consumption patterns: a Canadian rave population study. Can J Psychiatry 47:546–551
Hubner CB, Bird M, Rassnick S, Kornetsky C (1988) The threshold lowering effects of MDMA (ecstasy) on brain-stimulation reward. Psychopharmacology (Berl) 95:49–51
Jansen KL (1999) Ecstasy (MDMA) dependence. Drug Alcohol Depend 53:121–124
Khorana N, Pullagurla MR, Young R, Glennon RA (2004) Comparison of the discriminative stimulus effects of 3,4-methylenedioxymethamphetamine (MDMA) and cocaine: asymmetric generalization. Drug Alcohol Depend 74:281–287
Koob GF, Caine B, Markou A, Pulvirenti L, Weiss F (1994) Role for the mesocortical dopamine system in the motivating effects of cocaine. NIDA Res Monogr 145:1–18
Liechti ME, Baumann C, Gamma A, Vollenweider FX (2000) Acute psychological effects of 3,4-methylenedioxymethamphetamine (MDMA, “Ecstasy”) are attenuated by the serotonin uptake inhibitor citalopram. Neuropsychopharmacology 22:513–521
Lile JA, Ross JT, Nader MA (2005) A comparison of the reinforcing efficacy of 3,4-methylenedioxymethamphetamine (MDMA, “ecstasy”) with cocaine in rhesus monkeys. Drug Alcohol Depend 78:135–140
Lin HQ, Jackson DM, Atrens DM, Christie MJ, McGregor IS (1997) Serotonergic modulation of 3,4-methylenedioxymethamphetamine (MDMA)-elicited reduction of response rate but not rewarding threshold in accumbal self-stimulation. Brain Res 744:351–357
Milani RM, Parrott AC, Schifano F, Turner JJ (2005) Pattern of cannabis use in ecstasy polydrug users: moderate cannabis use may compensate for self-rated aggression and somatic symptoms. Hum Psychopharmacol 20(4):249–261
Nelson RA, Boyd SJ, Ziegelstein RC, Herning R, Cadet JL, Henningfield JE, Schuster CR, Contoreggi C, Gorelick DA (2005) Effect of rate of administration on subjective and physiological effects of intravenous cocaine in humans. Drug Alcohol Depend (in press)
O’Shea E, Granados R, Esteban B, Colado MI, Green AR (1998) The relationship between the degree of neurodegeneration of rat brain 5-HT nerve terminals and the dose and frequency of administration of MDMA (‘ecstasy’). Neuropharmacology 37:919–926
Parks KA, Kennedy CL (2004) Club drugs: reasons for and consequences of use. J Psychoactive Drugs 36:295–302
Parrott AC (2004) MDMA and the loss of reinforcement in Fantegrossi et al (2004). Neuropsychopharmacology 29:1940–1941 (author reply 1942)
Parrott AC (2005) Chronic tolerance to recreational MDMA (3,4-methylenedioxymethamphetamine) or ecstasy. J Psychopharmacol 19:71–83
Parrott AC, Lasky J (1998) Ecstasy (MDMA) effects upon mood and cognition: before, during and after a Saturday night dance. Psychopharmacology (Berl) 139:261–268
Ratzenboeck E, Saria A, Kriechbaum N, Zernig G (2001) Reinforcing effects of MDMA (“ecstasy”) in drug-naive and cocaine-trained rats. Pharmacology 62:138–144
Reid LD, Hubbell CL, Tsai J, Fishkin MD, Amendola CA (1996) Naltrindole, a delta-opioid antagonist, blocks MDMA’s ability to enhance pressing for rewarding brain stimulation. Pharmacol Biochem Behav 53:477–480
Ricaurte GA, DeLanney LE, Irwin I, Langston JW (1988) Toxic effects of MDMA on central serotonergic neurons in the primate: importance of route and frequency of drug administration. Brain Res 446:165–168
Rosecrans JA, Glennon RA (1987) The effect of MDA and MDMA (“Ecstasy”) isomers in combination with pirenpirone on operant responding in mice. Pharmacol Biochem Behav 28:39–42
Samaha AN, Robinson TE (2005) Why does the rapid delivery of drugs to the brain promote addiction? Trends Pharmacol Sci 26:82–87
Schechter MD (1987) MDMA as a discriminative stimulus: isomeric comparisons. Pharmacol Biochem Behav 27:41–44
Schechter MD (1991) Effect of MDMA neurotoxicity upon its conditioned place preference and discrimination. Pharmacol Biochem Behav 38:539–544
Schenk S, Gittings D, Johnstone M, Daniela E (2003) Development, maintenance and temporal pattern of self-administration maintained by ecstasy (MDMA) in rats. Psychopharmacology (Berl) 169:21–27
Schuster CR, Thompson T (1969) Self-administration of and behavioral dependence on drugs. Annu Rev Pharmacol 9:483–502
Schuster P, Lieb R, Lamertz C, Wittchen HU (1998) Is the use of ecstasy and hallucinogens increasing? Results from a community study. Eur Addict Res 4:75–82
Shulgin AT (1986) The background and chemistry of MDMA. J Psychoactive Drugs 18:291–304
Sprouse JS, Bradberry CW, Roth RH, Aghajanian GK (1989) MDMA (3,4-methylenedioxymethamphetamine) inhibits the firing of dorsal raphe neurons in brain slices via release of serotonin. Eur J Pharmacol 167:375–383
Strote J, Lee JE, Wechsler H (2002) Increasing MDMA use among college students: results of a national survey. J Adolesc Health 30:64–72
Vanderschuren LJ, Everitt BJ (2004) Drug seeking becomes compulsive after prolonged cocaine self-administration. Science 305:1017–1019
Vollenweider FX, Gamma A, Liechti M, Huber T (1999) Is a single dose of MDMA harmless? Neuropsychopharmacology 21:598–600
von Sydow K, Lieb R, Pfister H, Hofler M, Wittchen HU (2002) Use, abuse and dependence of ecstasy and related drugs in adolescents and young adults—a transient phenomenon? Results from a longitudinal community study. Drug Alcohol Depend 66:147–159
Wakonigg G, Sturm K, Saria A, Zernig G (2003) Methylenedioxymethamphetamine (MDMA, ‘ecstasy’) serves as a robust positive reinforcer in a rat runway procedure. Pharmacology 69:180–182
Wang X, Baumann MH, Xu H, Morales M, Rothman RB (2005) ({+/−})-3,4-Methylenedioxymethamphetamine (MDMA) administration to rats does not decrease levels of the serotonin transporter protein or alter its distribution between endosomes and the plasma membrane. J Pharmacol Exp Ther 314:1002–1012
Woolverton WL, Johanson CE (1984) Preference in rhesus monkeys given a choice between cocaine and d,l-cathinone. J Exp Anal Behav 41:35–43
Zernig G, Lewis JW, Woods JH (1997) Clocinnamox inhibits the intravenous self-administration of opioid agonists in rhesus monkeys: comparison with effects on opioid agonist-mediated antinociception. Psychopharmacology (Berl) 129:233–242
Zernig G, Giacomuzzi S, Riemer Y, Wakonigg G, Sturm K, Saria A (2003) Intravenous drug injection habits: drug users’ self-reports versus researchers’ perception. Pharmacology 68:49–56
Zernig G, Wakonigg G, Madlung E, Haring C, Saria A (2004) Do vertical shifts in dose–response rate relationships in operant conditioning procedures indicate “sensitization” to “drug wanting”? Psychopharmacology (Berl) 171:349–351 (author reply 352–363)
Acknowledgements
The authors wish to thank Drs. Thomas Newton and Ari Kalechstein for insightful scientific discussions on this topic. Support for this research provided by the National Institute on Drug Abuse (DA 15126-01).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
De La Garza, R., Fabrizio, K.R. & Gupta, A. Relevance of rodent models of intravenous MDMA self-administration to human MDMA consumption patterns. Psychopharmacology 189, 425–434 (2007). https://doi.org/10.1007/s00213-005-0255-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-005-0255-5