
Abstract
Summary
In this open population-based study from Northern Norway, there was no increase in hip fracture incidence in women and men from 1994 to 2008. Age-adjusted hip fracture rates was lower compared to reported rates from the Norwegian capital Oslo, indicating regional differences within the country.
Introduction
The aim of the present population-based study was to describe age- and sex-specific incidence of hip fractures in a Northern Norwegian city, compare rates with the Norwegian capital Oslo, describe time trends in hip fracture incidence, place of injury, seasonal variation and compare mortality after hip fracture between women and men.
Methods
Data on hip fractures from 1994 to 2008 in women and men aged 50 years and above were obtained from the Harstad Injury Registry.
Results
There were altogether 603 hip fractures in Harstad between 1994 and 2008. The annual incidenc rose exponentially from 5.8 to 349.2 per 10,000 in men, and from 8.7 to 582.2 per 10,000 in women from the age group 50–54 to 90+ years. The age-adjusted incidence rates were 101.0 and 37.4 in women and men, respectively, compared to 118.0 in women (p = 0.005) and 44.0 in men (p = 0.09) in Oslo. The age-adjusted incidence rates did not increase between 1994–1996 and 2006–2008. The majority of hip fractures occurred indoors and seasonal variation was significant in fractures occurring outdoors only. After adjusting for age at hip fracture, mortality after fracture was higher in men than in women 3, 6 and 12 months (p ≤ 0.002) after fracture.
Conclusions
There are regional differences in hip fracture incidence that cannot be explained by a north–south gradient in Norway. Preventive strategies must be targeted to indoor areas throughout the year and to outdoor areas in winter.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Hip fractures in the aged constitute a major health problem with substantial morbidity [1], mortality [2, 3], and, as the ageing population increases, an increasing burden on the health care system [4]. Fracture risk varies markedly between countries [5]. In a study by Kanis et al. [6], comparing 10-year probability of hip fracture, all countries except Norway had lower risk than Sweden. Other countries categorized at very high risk (>75% of the risk of Sweden) were Iceland, Denmark and the US. At the age of 80, the estimated probability of sustaining a hip fracture the next 10 years is 8.6% and 17.7% in Norwegian men and women, respectively [7], and a report from the Norwegian capital Oslo calculated an overall annual fracture rate of 118.0 in women and 44.0 in men per 10,000 [8].
Several recent studies are reporting declining fracture incidence [9–14]. Although the Norwegian hip fracture rates remain the highest reported in the world, data from Oslo in 1996–1997 indicated no increasing incidence rates compared to the 1988–1989 [8].Within Norway, considerable geographic differences have been reported, with substantially lower rates in smaller cities and rural areas compared to Oslo [7, 15]. However, these are reports based on sporadic studies in few regions and in limited time periods [16, 17].
From 1985 to 2003, the Norwegian Institute of Public Health commissioned four Norwegian hospitals, representing 10% of the population, to run a national injury registry [18]. The registry collected a variety of data connected to the actual injury itself and the event leading to the injury. In the city of Harstad in Northern Norway, the registration continued and has been running for more than 23 years. Throughout the years of the National Injury Registry, the injury rates in Harstad closely resembled the rates of the national registry [18]. With reference to the recent reports suggesting stabilizing hip fracture incidence internationally as well as nationally, and regional differences within Norway, we have used the hip fracture data in the Harstad Injury Registry to:
-
1.
Describe age- and sex-specific incidence of hip fractures in Harstad, Northern Norway and make comparison with rates from the Norwegian capital Oslo
-
2.
Describe time trends in hip fracture incidence in Harstad from 1994 to 2008
-
3.
Describe place of injury and seasonal variations in hip fracture incidence in Harstad
-
4.
Compare 3-month, 6-month, and 1-year mortality after hip fracture between women and men in Harstad
Materials and method
The municipality of Harstad, located 250 km north of the Arctic Circle, comprises with its 23,257 inhabitants (January 1, 2010), 0.5% of the Norwegian population. All injured persons, including hip fracture patients, entering the hospital emergency room are recorded in the Harstad Injury Registry. The local hospital, which is the only hospital in the area, has an X-ray department and access to orthopedic surgery, and all patients with hip fractures are treated locally with a minimal leakage to other hospitals. From 1985 to 1993, the registration of hip fractures was used for evaluation of an injury prevention program [18, 19]. Data from the period between 1985 and 1988 provided baseline information for a 5-year intensive community-based intervention program running between 1989 and 1993, which included removal of environmental hazards in homes, promotion of safe footwear used outdoors and reduction of slippery surfaces in traffic areas during winter. The results indicated a significant reduction of hip fracture rates related to falls indoors and in traffic areas in winter in men [18]. After 1993, the intervention program continued as an integrated part of the community health service and the present study encompasses the years from 1994 to 2008, after termination of the prevention study.
Registration of hip fractures
On admission in the hospital, the patient or someone accompanying him/her and the admitting doctor complete an injury registration form providing information concerning name, date of birth, sex, place of residence, activity during injury, time, place and type of injury as well as injury mechanism and body part injured. An open-ended question describes in free text the event leading to the injury. The admitting doctor registers the patient’s diagnosis to the injury registration form, usually based on the present clinical symptoms. The forms are collected and examined by a specially trained nurse who also assures that all incidents are registered by comparing with the admission list. She then enters the data into a common database. Hip fracture data from the Harstad Injury Registry are retrieved by a search combining body part and diagnosis.
Validation of the fracture registration
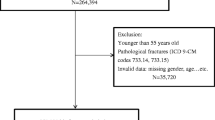
From the municipality of Harstad, altogether 639 hip fractures were recorded in the Harstad Injury Registry in persons aged 50 years and above during the 15 years from 1994 to 2008. In 2009, the medical records on every hip fracture event in the registry were retrieved for examination of X-ray description, operation and discharge report, the date and side of hip fracture. Patients with repeated entries, sequel from a previous fracture (e.g. caput necrosis, infection, failure of fixation materials), contusion of the hip without verified fracture, femur shaft or pelvic fractures and pathological fractures due to cancer metastasis were excluded from the analyses. Patients living outside the municipality were also excluded from the analyses. The validation procedures excluded 51 (8%) of 639 registered fractures. Searching the patient administrative system for the period between 2002 and 2008 identified additional 15 fractures, which are included in the incidence analyses (research questions 1 and 2) and the mortality analyses (research question 4), altogether 603 hip fractures in analyses. A complete dataset with 588 hip fractures and information concerning the fracture event was available for description of place of injury and seasonal variation (research question 3).
Statistical analyses
Age at fracture in women and men were compared using independent sample t-test. For each sex, we tested for time trends in age at fracture using linear regression.
Average incidence rates per 10,000 person years were calculated for each sex in 5-year age groups for the time period 1994–2008. The age- and sex-specific fracture rates were compared with the corresponding rates reported from Oslo in 1996–1997 [8], where hip fracture data was collected for the whole population through patient administrative data of the hospitals of the city [8]. For each sex, an age-adjusted rate was calculated for two 3-year time periods: 1994–1996 and 2006–2008, using the age distribution in Oslo in January 1, 1997 as reference [8]. Assuming a Poisson distribution of the number of hip fractures, 95% confidence limits for the rates were calculated and the difference between incidence rates was tested. Dividing the data in (age) groups, we performed several tests simultaneously and should adjust for simultaneous testing. We have chosen to use the false discovery rate (FDR) which controls the expected proportion of incorrectly rejected null hypotheses (type I errors) and is less conservative and has a higher power than the more traditionally used Bonferroni correction [20].
Potential time trends in incidence rates over the study period were analyzed using linear regression. Place of injury for each sex was compared using Chi-square testing. Seasonal variation in the number of hip fractures was analyzed by Cosinor analyses with month of the year as analytical units. A Cosinor analysis is essentially a regression where the independent variable represents a sine and a cosine transform of a time factor: \( {y_t} = {a_0} + {a_1}\cos \frac{{2\pi t}}{T} + {a_2}\sin \frac{{2\pi t}}{\hbox{T}} \), where t is the time step (month) and T the total time period (12 months). To test for significance of seasonality, we tested whether the model was statistically significant.
Mortality was analyzed by survival analysis using Cox’s proportional hazard rate including censoring. The follow-up time for one person was from the day the fracture occurred to death or the censoring date in January 1, 2009. The analyses were performed using the Statistical Package for Social Sciences version 15.0 (SPSS, Chicago, IL, USA), Microsoft Office Excel version 2007 and the statistical program R, version 2.11.0 (The R Foundation for Statistical Computing).
Results
Fracture incidence and time trends
Of the 603 fractures, 73% (95% CI: 69.5, 76.5) occurred in women providing a female:male ratio of 2.7. The mean age at fracture in this population (aged 50 years and above) was 80.0 years (95% CI: 79.1, 80.9) in women and 76.7 years (95% CI: 75.1, 78.3) in men (p < 0.001). The median age at hip fracture was 81.7 and 79.3 years in women and men, respectively. Age at fracture did not change during the 15 years, neither in women (p = 0.43) nor in men (p = 0.26). The incidence of hip fractures rose exponentially with increasing age from 5.8 to 349.2 per 10,000 in men, and from 8.7 to 582.2 per 10,000 in women (Table 1 and Fig. 1). The incidence rates differed significantly between the two sexes only in the age groups 75–79 (p = 0.01) and 80–84 (p = 0.005).

Hip fracture incidence rates pr 10,000 in women and men in Harstad (1994–2008) and Oslo (1996–1997), Norway
Table 2 displays the incidence rates in Harstad compared with reported rates from four studies from other parts of Norway. Compared to Oslo, the age-specific rates in Harstad were lower than those reported from Oslo in 1996–1997 (Fig. 1, Table 2). The crude incidence rate was 77.0 in women and 31.9 in men per 10,000 in Harstad. Using the age distribution of the Oslo population 01.01.1997 as the reference, the age adjusted incidence rates in Harstad were 101.0 and 37.4 per 10,000 in women and men, respectively, compared to 118.0 per 10,000 in women (p = 0.005) and 44.0 per 10,000 in men (p = 0.09) in Oslo [8]. Using the same reference, the age adjusted incidence rates in Harstad were 150.0 and 71.0 per 10,000 in women and men above the age of 65 years, respectively. The corresponding figures for Oslo were 192.0 per 10,000 in women (p < 0.001) and 85.5 per 10,000 in men (p = 0.07) [8].
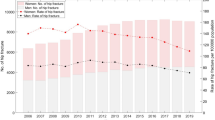
Fig. 2 displays the age-adjusted incidence of hip fractures in women and men in Harstad during 1994–2008 for three different age groups. There were indications of an increase in the incidence in men aged 65–79, but adjusting for multiple testing, the trend was no longer significant. The age-adjusted incidence rates for women were 97.3 and 105.2 per 10,000 in 1994–1996 and 2006–2008, respectively (p = 0.55). The corresponding incidence rates for men were 32.5 and 46.3 per 10,000, respectively (p = 0.12).

Incidence of hip fractures in three different age groups in women and men in Harstad, Northern Norway, from 1994 to 2008, adjusted using the age distribution of the Oslo population in January 1, 1997 as the reference
Place of injury, seasonal variation and mortality after fracture
Place of injury and the mean age when hip fracture occurred is displayed in Table 3. We had information about place of injury in 531 persons (90%), and among these, more than 70% were fall-related hip fractures occurring at different places indoors. Among outdoor fractures, only 3 of 103 occurring in transport areas were caused by traffic accidents, all the others were fall-related hip fractures, occurring on slippery or uneven surfaces. Age at fracture differed significantly between places of injury (p < 0.001; ANOVA), with highest mean age at fracture among those occurring in nursing homes and lowest fracture age among those happening in transport areas. Place of injury differed significantly between the sexes (p = 0.006), but after adjusting for age, the difference was no longer significant (p = 0.05).
The monthly distribution of hip fractures in women and men are displayed in Fig. 3. In the Cosinor analyses, including all hip fractures in the model, the seasonal variation was significant (p = 0.001) and seasonality explained >71% of the variation in hip fracture rate (R adj² 0.71), with the highest numbers of hip fractures occurring between December and March and the lowest between May and September. Stratifying on place of injury, the seasonal variation was significant only in the models including the fractures that occurred outdoors, at home or in traffic areas (p < 0.001; Fig. 3), not in the models including fractures occurring indoors, at home or in nursing homes.

Seasonal variation in hip fracture incidence. Total All fractures, Indoor fractures occurring indoors at home, in hospital or nursing home, Outdoor fractures occurring outdoors at home or in traffic areas
Total mortality after hip fracture was higher in men than in women 3 months after fracture (16 vs. 8%), after 6 months (19 vs. 13%) and after 12 months (25 vs. 19%). All comparisons were statistically significant (p ≤ 0.002) after adjustment for age at hip fracture.
Discussion
The main finding from this study with 15 years of population-based data is that the age-adjusted hip fracture incidence rates of women above 50 years are significantly lower in Harstad, Northern Norway, than in Oslo. The incidence rates in Harstad are comparable to the rates reported from two other cities, a city in the central [17] and south easternparts of Norway [16], in women, but higher than the rates in the more rural area in mid-Norway [15] (Table 2). Our results confirm that there is a great variation in hip fracture rates between different regions in Norway [7], as there is for distal forearm fractures [21]. Furthermore, the age-adjusted rates from Harstad are lower than both winter and summer rates in Oslo [8] and also lower than earlier reported rates from Copenhagen and Gothenburg, but they are higher than reported rates from the US [5].
International variations in hip fracture risk have displayed a north–south gradient [6] which has been linked to the importance of sunlight exposure [22]. A study using national data from France showed substantial heterogeneity of hip fracture risk within the country, with higher hip fracture risk in the Southern France [23]. Other studies reporting regional differences in hip fracture rates within countries explain the differences by an urban–rural gradient [24]. In a study from Australia, the age-adjusted incidence of hip fracture was 32% lower in rural compared to urban residents aged 60 years and above, 26% lower in women [25]. In comparison, the age-adjusted rates in women aged 65 years and above were 21% lower in Harstad than in the more urbanized capitol Oslo [8]. Unfortunately, with the registry data available, we do not have explanation for the indicated urban–rural difference, but another Norwegian study reported higher bone mineral density levels in rural versus urban dwellers at the hip [26], one factor which may explain differences in fracture risk. In a study by Ringsberg et al. [27], urban subjects had significantly poorer balance compared with their rural counterparts, a difference which increased with increasing age, affected gait performance and risk of falls. With an extensive prevention program running in Harstad between 1988 and 1993 [18, 19] and part of this program still integrated in the community health service, this may also explain the differences in fracture rates between Harstad and Oslo.
It could furthermore be expected that the extensive prevention program might have resulted in lower fracture rates especially in the first years after 1994. However, comparison of the two periods, 1994–1996 and 2006–2008, indicated no significant change in the age-adjusted incidence rates in any of the sexes during the time of the study. Interestingly, this stability of age-adjusted incidence rates is in accordance with data from Oslo [8] and reports from several other countries including Finland, Denmark, Norway, Switzerland, Canada, US and Australia [10, 12–15, 28]. There are studies reporting increasing numbers of hip fracture rates in women and men in Germany and Austria [29, 30], in men in Switzerland [28], in the oldest age groups in Swedish [31] and Swiss [32] women. Conflicting results are also reported within countries where, for example, a recent paper from the Australian Capital Territory reported significant declining hip fracture rates after 2001 in women [13], while other data from Australia indicate no change in incidence [33]. The Australian report suggests that the declining hip fracture rates may be explained by increased use of anti-osteoporotic treatments [13]. In the Danish study reporting declining hip fracture rates from 1997 to 2006, it is noted that the decrease is too large to be explained by the extent of anti-osteoporotic medication and therefore must be explained by other factors [11].
As reported from several other studies, both within Norway [17] and from other countries like UK [34] and the US [35], there was a significant seasonal variation in the occurrence of hip fractures in our study. In a study comparing and observing seasonal variation of hip fractures in Scotland, Hong Kong and New Zealand [36] as well as in Taiwan [ Bentler SE, Liu L, Obrizan M, Cook EA, Wright KB, Geweke JF, Chrischilles EA, Pavlik CE, Wallace RB, Ohsfeldt RL, Jones MP, Rosenthal GE, Wolinsky FD (2009) The aftermath of hip fracture: discharge placement, functional status change, and mortality. Am J Epidemiol 170:1290–1299 Center JR, Nguyen TV, Schneider D, Sambrook PN, Eisman JA (1999) Mortality after all major types of osteoporotic fracture in men and women: an observational study. Lancet 353:878–882 Johnell O, Kanis JA, Oden A, Sernbo I, Redlund-Johnell I, Petterson C, De Laet C, Jonsson B (2004) Mortality after osteoporotic fractures. Osteoporos Int 15:38–42 Azhar A, Lim C, Kelly E, O'Rourke K, Dudeney S, Hurson B, Quinlan W (2008) Cost induced by hip fractures. Ir Med J 101:213–215 Johnell O, Kanis JA (2004) An estimate of the worldwide prevalence, mortality and disability associated with hip fracture. Osteoporos Int 15:897–902 Kanis JA, Johnell O, De Laet C, Jonsson B, Oden A, Ogelsby AK (2002) International variations in hip fracture probabilities: implications for risk assessment. J Bone Miner Res 17:1237–1244 Falch JA, Kaastad TS, Bohler G, Espeland J, Sundsvold OJ (1993) Secular increase and geographical differences in hip fracture incidence in Norway. Bone 14:643–645 Lofthus CM, Osnes EK, Falch JA, Kaastad TS, Kristiansen IS, Nordsletten L, Stensvold I, Meyer HE (2001) Epidemiology of hip fractures in Oslo, Norway. Bone 29:413–418 Kannus P, Niemi S, Parkkari J, Palvanen M, Vuori I, Jarvinen M (2006) Nationwide decline in incidence of hip fracture. J Bone Miner Res 21:1836–1838 Melton LJ III, Kearns AE, Atkinson EJ, Bolander ME, Achenbach SJ, Huddleston JM, Therneau TM, Leibson CL (2009) Secular trends in hip fracture incidence and recurrence. Osteoporos Int 20:687–694 Abrahamsen B, Vestergaard P (2010) Declining incidence of hip fractures and the extent of use of anti-osteoporotic therapy in Denmark 1997–2006. Osteoporos Int 21:373–380 Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB (2009) Incidence and mortality of hip fractures in the United States. JAMA 302:1573–1579 Fisher AA, O'Brien ED, Davis MW (2009) Trends in hip fracture epidemiology in Australia: possible impact of bisphosphonates and hormone replacement therapy. Bone 45:246–253 Leslie WD, O'Donnell S, Jean S, Lagace C, Walsh P, Bancej C, Morin S, Hanley DA, Papaioannou A (2009) Trends in hip fracture rates in Canada. JAMA 302:883–889 Grønskag AB, Forsmo S, Romundstad P, Langhammer A, Schei B (2010) Incidence and seasonal variation in hip fracture incidence among elderly women in Norway. The HUNT Study. Bone 46:1294–1298 Bjorgul K, Reikeras O (2007) Incidence of hip fracture in southeastern Norway: a study of 1, 730 cervical and trochanteric fractures. Int Orthop 31:665–669 Finsen V, Johnsen LG, Trano G, Hansen B, Sneve KS (2004) Hip fracture incidence in central norway: a followup study. Clin Orthop Relat Res:173–178 Ytterstad B (1996) The Harstad injury prevention study: community based prevention of fall-fractures in the elderly evaluated by means of a hospital based injury recording system in Norway. J Epidemiol Community Health 50:551–558 Ytterstad B (1999) The Harstad injury prevention study: the characteristics and distribution of fractures amongst elders—an eight year study. Int J Circumpolar Health 58:84–95 Hochberg Y, Benjamini Y (1990) More powerful procedures for multiple significance testing. Stat Med 9:811–818 Sogaard AJ, Gustad TK, Bjertness E, Tell GS, Schei B, Emaus N, Meyer HE (2007) Urban–rural differences in distal forearm fractures: Cohort Norway. Osteoporos Int 18:1063–1072 Johnell O, Borgstrom F, Jonsson B, Kanis J (2007) Latitude, socioeconomic prosperity, mobile phones and hip fracture risk. Osteoporos Int 18:333–337 Barbier S, Ecochard R, Schott AM, Colin C, Delmas PD, Jaglal SB, Couris CM (2009) Geographical variations in hip fracture risk for women: strong effects hidden in standardised ratios. Osteoporos Int 20:371–377 Sanders KM, Seeman E, Ugoni AM, Pasco JA, Martin TJ, Skoric B, Nicholson GC, Kotowicz MA (1999) Age- and gender-specific rate of fractures in Australia: a population-based study. Osteoporos Int 10:240–247 Sanders KM, Nicholson GC, Ugoni AM, Seeman E, Pasco JA, Kotowicz MA (2002) Fracture rates lower in rural than urban communities: the Geelong osteoporosis study. J Epidemiol Community Health 56:466–470 Omsland TK, Gjesdal CG, Emaus N, Tell GS, Meyer HE (2008) Regional differences in hip bone mineral density levels in Norway: the NOREPOS study. Osteoporos Int 20:631–638 Ringsberg KA, Gardsell P, Johnell O, Jonsson B, Obrant KJ, Sernbo I (1998) Balance and gait performance in an urban and a rural population. J Am Geriatr Soc 46:65–70 Chevalley T, Guilley E, Herrmann FR, Hoffmeyer P, Rapin CH, Rizzoli R (2007) Incidence of hip fracture over a 10-year period (1991–2000): reversal of a secular trend. Bone 40:1284–1289 Icks A, Haastert B, Wildner M, Becker C, Meyer G (2008) Trend of hip fracture incidence in Germany 1995–2004: a population-based study. Osteoporos Int 19:1139–1145 Mann E, Meyer G, Haastert B, Icks A (2010) Comparison of hip fracture incidence and trends between Germany and Austria 1995–2004: an epidemiological study. BMC Public Health 10:46 Bergstrom U, Jonsson H, Gustafson Y, Pettersson U, Stenlund H, Svensson O (2009) The hip fracture incidence curve is shifting to the right. Acta Orthop 80:520–524 Guilley E, Chevalley T, Herrmann F, Baccino D, Hoffmeyer P, Rapin CH, Rizzoli R (2008) Reversal of the hip fracture secular trend is related to a decrease in the incidence in institution-dwelling elderly women. Osteoporos Int 19:1741–1747 Chang KP, Center JR, Nguyen TV, Eisman JA (2004) Incidence of hip and other osteoporotic fractures in elderly men and women: Dubbo Osteoporosis Epidemiology Study. J Bone Miner Res 19:532–536 Crawford JR, Parker MJ (2003) Seasonal variation of proximal femoral fractures in the United Kingdom. Injury 34:223–225 Bischoff-Ferrari HA, Orav JE, Barrett JA, Baron JA (2007) Effect of seasonality and weather on fracture risk in individuals 65 years and older. Osteoporos Int 18:1225–1233 Douglas S, Bunyan A, Chiu KH, Twaddle B, Maffulli N (2000) Seasonal variation of hip fracture at three latitudes. Injury 31:11–19 Lin HC, **raxagar S (2006) Seasonality of hip fractures and estimates of season-attributable effects: a multivariate ARIMA analysis of population-based data. Osteoporos Int 17:795–806 Bliuc D, Nguyen ND, Milch VE, Nguyen TV, Eisman JA, Center JR (2009) Mortality risk associated with low-trauma osteoporotic fracture and subsequent fracture in men and women. JAMA 301:513–521 Kannegaard PN, van der MS, Eiken P, Abrahamsen B (2010) Excess mortality in men compared with women following a hip fracture. National analysis of comedications, comorbidity and survival. Age Ageing 39:203–209 Forsen L, Sogaard AJ, Meyer HE, Edna T, Kopjar B (1999) Survival after hip fracture: short- and long-term excess mortality according to age and gender. Osteoporos Int 10:73–78 Haentjens P, Magaziner J, Colon-Emeric CS, Vanderschueren D, Milisen K, Velkeniers B, Boonen S (2010) Meta-analysis: excess mortality after hip fracture among older women and men. Ann Intern Med 152:380–390 Bischoff-Ferrari HA, Willett WC, Wong JB, Giovannucci E, Dietrich T, wson-Hughes B (2005) Fracture prevention with vitamin D supplementation: a meta-analysis of randomized controlled trials. JAMA 293:2257–2264 Kanis JA, Johnell O, Oden A, Johansson H, De Laet C, Eisman JA, Fujiwara S, Kroger H, McCloskey EV, Mellstrom D, Melton LJ, Pols H, Reeve J, Silman A, Tenenhouse A (2005) Smoking and fracture risk: a meta-analysis. Osteoporos Int 16:155–162 De Laet C, Kanis JA, Oden A, Johanson H, Johnell O, Delmas P, Eisman JA, Kroger H, Fujiwara S, Garnero P, McCloskey EV, Mellstrom D, Melton LJ III, Meunier PJ, Pols HA, Reeve J, Silman A, Tenenhouse A (2005) Body mass index as a predictor of fracture risk: a meta-analysis. Osteoporos Int 16:1330–1338References
Acknowledgements
We are greatly thankful for the commitment of the study nurse Ellen Nikolaisen in the Harstad Injury Registry.
Conflicts of interest
None.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Emaus, N., Olsen, L.R., Ahmed, L.A. et al. Hip fractures in a city in Northern Norway over 15 years: time trends, seasonal variation and mortality. Osteoporos Int 22, 2603–2610 (2011). https://doi.org/10.1007/s00198-010-1485-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-010-1485-x