
Abstract
Purpose
To present the clinical outcomes and magnetic resonance imaging (MRI) analysis of adjustable cortical suspensory fixation for the femur and tibia in hamstring autograft anterior cruciate ligament reconstruction.
Methods
A cohort of 233 sequential patients was analysed for graft failure rate and subjective IKDC, Tegner and Lysholm scores. 144 validated 1-year MRIs assessed and correlated graft healing and tunnel widening.
Results
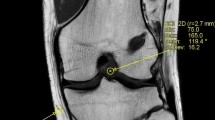
At mean follow-up of 28 months ± 8.2 [median 26, range 12–49], the graft failure rate was 4.7%. Significant improvements were seen in all clinical scores (p < 0.001). MRI analysis showed 71% with fully integrated grafts in the tibia and 24% in the femur, with the remainder all showing greater than 50% integration. Graft signal was low and homogenous in 67% in the tibia, 29% in the intra-articular portion and 20% in the femur. One patient had greater than 50% high signal in the tibial graft and one in the intra-articular graft, all others demonstrated greater than 50% low signal. Both graft integration and signal were significantly better in the tibia than the femur (p < 0.01). Tunnel widening was 2.2 ± 1.4 mm and 2.7 ± 1.3 mm in the tibia and femur, respectively. Comparison of individual MRI appearances and overall clinical outcome at the same 12-month point demonstrated no consistent significant correlation.
Conclusion
Adjustable cortical suspensory fixation in both femoral and tibial tunnels provides good clinical outcomes and a low graft rupture rate. Grafts demonstrate healing with comparatively low tunnel widening. There was no consistent significant correlation between the appearances on MRI and clinical outcome.
Level of evidence
Case–control study, Level III.




Similar content being viewed by others


References
Anderson AF, Irrgang JJ, Kocher MS, Mann BJ, Harrast JJ, International Knee Documentation Committee (2006) The International Knee Documentation committee subjective knee evaluation form: normative data. Am J Sports Med 34:128–135
Baumfeld JA, Diduch DR, Rubino LJ, Hart JA, Miller MD, Barr MS, Hart JM (2008) Tunnel widening following anterior cruciate ligament reconstruction using hamstring autograft: a comparison between double cross-pin and suspensory graft fixation. Knee Surg Sports Traumatol Arthrosc 16:1108–1113
Browning WM, Kluczynski MA, Curatolo C, Marzo JM (2017) Suspensory versus aperture fixation of a quadrupled hamstring tendon autograft in anterior cruciate ligament reconstruction: a meta-analysis. Am J Sports Med 45:2418–2427
Buck DC, Simonian PT, Larson RV, Borrow J, Nathanson DA (2004) Timeline of tibial tunnel expansion after single-incision hamstring anterior cruciate ligament reconstruction. Arthroscopy 20:34–36
Calvo R, Figueroa D, Figueroa F, Vaisman A, Schmidt-Hebbel A, Morales N, Izquierdo G (2017) Five-strand hamstring autograft versus quadruple hamstring autograft with graft diameters 8.0 millimeters or more in anterior cruciate ligament reconstruction: clinical outcomes with a minimum 2-year follow-up. Arthroscopy 33:1007–1013
Cavaignac E, Marot V, Faruch M, Reina N, Murgier J, Accadbled F, Berard E, Chiron P (2018) Hamstring graft incorporation according to the length of the graft inside tunnels. Am J Sports Med 46:348–356
Choi N-H, Yang B-S, Victoroff BN (2017) Clinical and radiological outcomes after hamstring anterior cruciate ligament reconstructions: comparison between fixed-loop and adjustable-loop cortical suspension devices. Am J Sports Med 45:826–831
Claes S, Verdonk P, Forsyth R, Bellemans J (2011) The “ligamentization” process in anterior cruciate ligament reconstruction: what happens to the human graft? A systematic review of the literature. Am J Sports Med 39:2476–2483
Clatworthy MG, Annear P, Bulow JU, Bartlett RJ (1999) Tunnel widening in anterior cruciate ligament reconstruction: a prospective evaluation of hamstring and patella tendon grafts. Knee Surg Sports Traumatol Arthrosc 7:138–145
Coats AC, Johnson DL (2012) Two-stage revision anterior cruciate ligament reconstruction: indications, review, and technique demonstration. Orthopedics 35:958–960
Colombet P, Graveleau N, Jambou S (2016) Incorporation of hamstring grafts within the tibial tunnel after anterior cruciate ligament reconstruction: magnetic resonance imaging of suspensory fixation versus interference screws. Am J Sports Med 44:2838–2845
Colombet P, Saffarini M, Bouguennec N (2018) Clinical and functional outcomes of anterior cruciate ligament reconstruction at a minimum of 2 years using adjustable suspensory fixation in both the femur and tibia: a prospective study. Orthop J Sports Med 6:2325967118804128
Conte EJ, Hyatt AE, Gatt CJ, Dhawan A (2014) Hamstring autograft size can be predicted and is a potential risk factor for anterior cruciate ligament reconstruction failure. Arthrosc J Arthrosc Relat Surg 30:882–890
Debieux P, Franciozi CES, Lenza M, Tamaoki MJ, Magnussen RA, Faloppa F, Belloti JC (2016) Bioabsorbable versus metallic interference screws for graft fixation in anterior cruciate ligament reconstruction. Cochrane Database Syst Rev 7:CD009772
Firat A, Catma F, Tunc B, Hacihafizoglu C, Altay M, Bozkurt M, Kapicioglu MIS (2014) The attic of the femoral tunnel in anterior cruciate ligament reconstruction: a comparison of outcomes of two suspensory femoral fixation systems. Knee Surg Sports Traumatol Arthrosc 22:1097–1105
Ge Y, Li H, Tao H, Hua Y, Chen J, Chen S (2015) Comparison of tendon-bone healing between autografts and allografts after anterior cruciate ligament reconstruction using magnetic resonance imaging. Knee Surg Sports Traumatol Arthrosc 23:954–960
Grasso S, Linklater J, Li Q, Parker DA (2018) Validation of an MRI protocol for routine quantitative assessment of tunnel position in anterior cruciate ligament reconstruction. Am J Sports Med 46:1624–1631
Grindem H, Eitzen I, Moksnes H, Snyder-Mackler L, Risberg MA (2012) A pair-matched comparison of return to pivoting sports at 1 year in anterior cruciate ligament-injured patients after a nonoperative versus an operative treatment course. Am J Sports Med 40:2509–2516
Howell SM, Clark JA, Blasier RD (1991) Serial magnetic resonance imaging of hamstring anterior cruciate ligament autografts during the first year of implantation. A preliminary study. Am J Sports Med 19:42–47
Jansson KA, Harilainen A, Sandelin J, Karjalainen PT, Aronen HJ, Tallroth K (1999) Bone tunnel enlargement after anterior cruciate ligament reconstruction with the hamstring autograft and endobutton fixation technique. A clinical, radiographic and magnetic resonance imaging study with 2 years follow-up. Knee Surg Sports Traumatol Arthrosc 7:290–295
Li H-Y, Li H, Wu Z-Y, Chen J-W, Chen S-Y (2018) MRI-based tendon bone healing is related to the clinical functional scores at the first year after anterior cruciate ligament reconstruction with hamstring tendon autograft. Knee Surg Sports Traumatol Arthrosc 26:615–621
L’Insalata JC, Klatt B, Fu FH, Harner CD (1997) Tunnel expansion following anterior cruciate ligament reconstruction: a comparison of hamstring and patellar tendon autografts. Knee Surg Sports Traumatol Arthrosc 5:234–238
Lopes OV, de Freitas Spinelli L, Leite LHC, Buzzeto BQ, Saggin PRF, Kuhn A (2017) Femoral tunnel enlargement after anterior cruciate ligament reconstruction using RigidFix compared with extracortical fixation. Knee Surg Sports Traumatol Arthrosc 25:1591–1597
Lui P, Zhang P, Chan K, Qin L (2010) Biology and augmentation of tendon-bone insertion repair. J Orthop Surg 5:59
Mayr R, Rosenberger R, Agraharam D, Smekal V, El Attal R (2012) Revision anterior cruciate ligament reconstruction: an update. Arch Orthop Trauma Surg 132:1299–1313
Mayr R, Smekal V, Koidl C, Coppola C, Fritz J, Rudisch A, Kranewitter C, Attal R (2017) Tunnel widening after ACL reconstruction with aperture screw fixation or all-inside reconstruction with suspensory cortical button fixation: volumetric measurements on CT and MRI scans. Knee 24:1047–1054
Muller B, Yabroudi MA, Lynch A, Lai C-L, van Dijk CN, Fu FH, Irrgang JJ (2016) Defining thresholds for the patient acceptable symptom state for the IKDC subjective knee form and KOOS for patients who underwent ACL reconstruction. Am J Sports Med 44:2820–2826
Otsuka H, Ishibashi Y, Tsuda E, Sasaki K, Toh S (2003) Comparison of three techniques of anterior cruciate ligament reconstruction with bone-patellar tendon-bone graft. Differences in anterior tibial translation and tunnel enlargement with each technique. Am J Sports Med 31:282–288
Pereira H, Pereira HMD, Correlo VM, Silva-Correia J, Oliveira JM, Reis RL, Reis Ceng RL, Espregueira-Mendes J (2013) Migration of “bioabsorbable” screws in ACL repair. How much do we know? A systematic review. Knee Surg Sports Traumatol Arthrosc 21:986–994
Rizer M, Foremny GB, Rush A, Singer AD, Baraga M, Kaplan LD, Jose J (2017) Anterior cruciate ligament reconstruction tunnel size: causes of tunnel enlargement and implications for single versus two-stage revision reconstruction. Skeletal Radiol 46:161–169
Rodeo SA, Kawamura S, Kim H-J, Dynybil C, Ying L (2006) Tendon healing in a bone tunnel differs at the tunnel entrance versus the tunnel exit: an effect of graft-tunnel motion? Am J Sports Med 34:1790–1800
Sabat D, Kundu K, Arora S, Kumar V (2011) Tunnel widening after anterior cruciate ligament reconstruction: a prospective randomized computed tomography–based study comparing 2 different femoral fixation methods for hamstring graft. Arthroscopy 27:776–783
Schultz WR, McKissick RC, DeLee JC (2007) Tibial tunnel widening after hamstring tendon anterior cruciate ligament reconstruction: the effect of supplemental aperture fixation with autogenous bone cores. Am J Sports Med 35:1725–1730
Smith PA, DeBerardino TM (2015) Tibial fixation properties of a continuous-loop ACL hamstring graft construct with suspensory fixation in porcine bone. J Knee Surg 28:506–512
Smith PA, Stannard JP, Pfeiffer FM, Kuroki K, Bozynski CC, Cook JL (2016) Suspensory versus interference screw fixation for arthroscopic anterior cruciate ligament reconstruction in a translational large-animal model. Arthroscopy 32:1086–1097
Takenaga T, Yoshida M, Albers M, Nagai K, Nakamura T, Fu FH, Onishi K (2019) Preoperative sonographic measurement can accurately predict quadrupled hamstring tendon graft diameter for ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 27(3):797–804
Tashiro Y, Gale T, Sundaram V, Nagai K, Irrgang JJ, Anderst W, Nakashima Y, Tashman S, Fu FH (2017) The graft bending angle can affect early graft healing after anterior cruciate ligament reconstruction: in vivo analysis with 2 years’ follow-up. Am J Sports Med 45:1829–1836
Tegner Y, Lysholm J (1985) Rating systems in the evaluation of knee ligament injuries. Clin Orthop 198:43–49
Tutkus V, Kluonaitis K, Silove S, Tutkuviene J (2018) ACL reconstruction using 5- or 6-strand hamstring autograft provides graft’s diameter bigger than 8 mm. Knee Surg Sports Traumatol Arthrosc 26:1349–1356
Webster KE, Feller JA, Hameister KA (2001) Bone tunnel enlargement following anterior cruciate ligament reconstruction: a randomised comparison of hamstring and patellar tendon grafts with 2-year follow-up. Knee Surg Sports Traumatol Arthrosc 9:86–91
Yamazaki S, Yasuda K, Tomita F, Minami A, Tohyama H (2006) The effect of intraosseous graft length on tendon-bone healing in anterior cruciate ligament reconstruction using flexor tendon. Knee Surg Sports Traumatol Arthrosc 14:1086–1093
Zantop T, Ferretti M, Bell KM, Brucker PU, Gilbertson L, Fu FH (2008) Effect of tunnel-graft length on the biomechanics of anterior cruciate ligament-reconstructed knees: intra-articular study in a goat model. Am J Sports Med 36:2158–2166
Funding
The authors declare that no direct funding was received for this study. Senior authors David Parker and Brett Fritsch receive institutional support from Arthrex.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
IRB ethical approval was received for this study by Northern Sydney Local Health District reference HREC/17/HAWKE/140.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Putnis, S., Neri, T., Grasso, S. et al. ACL hamstring grafts fixed using adjustable cortical suspension in both the femur and tibia demonstrate healing and integration on MRI at one year. Knee Surg Sports Traumatol Arthrosc 28, 906–914 (2020). https://doi.org/10.1007/s00167-019-05556-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-019-05556-6