
Abstract
Objective
To evaluate anion and osmolal gaps as diagnostic tools in methanol poisoning.
Design and setting
Clinical observational study.
Patients and methods
In a recent methanol outbreak, the initial triage and treatment decisions in 28 patients were based mainly upon the values of the osmolal and anion gaps on admission. Methanol and formate levels were later compared to these gaps by linear regression analysis.
Results
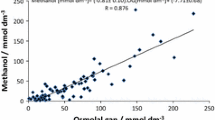
The correlation between the osmolal gaps and serum methanol concentrations on admission was linear (y = 1.03x+12.71, R2 = 0.94). The anion gaps correlated well with the serum formate concentrations (y = 1.12x+13.82, R2 = 0.86). Both gaps were elevated in 24 of the 28 subjects upon admission. Three patients had an osmolal gap within the reference area (because of low serum methanol), but elevated anion gap because of formate accumulation. One patient with probable concomitant ethanol ingestion had a high osmolal gap and a normal anion gap.
Conclusion
Osmolal and anion gaps are useful in the diagnosis and triage of methanol-exposed subjects. Confounders are low serum methanol and concomitant ethanol ingestion.




Similar content being viewed by others


References
Barceloux DG, Bond GR, Krenzelok EP, Cooper H, Vale JA (2002) American Academy of Clinical Toxicology practice guidelines on the treatment of methanol poisoning. J Toxicol Clin Toxicol 40:415–446
Jacobsen D, McMartin KE (1997) Antidotes for methanol and ethylene glycol poisoning. J Toxicol Clin Toxicol 35:127–143
Sejersted OM, Jacobsen D, Ovrebo S, Jansen H (1983) Formate concentrations in plasma from patients poisoned with methanol. Acta Med Scand 213:105–110
Hoffman RS, Smilkstein MJ, Howland MA, Goldfrank LR (1993) Osmol gaps revisited: normal values and limitations. J Toxicol Clin Toxicol 31:81–93
Aabakken L, Johansen KS, Rydningen EB, Bredesen JE, Ovrebo S, Jacobsen D (1994) Osmolal and anion gaps in patients admitted to an emergency medical department. Hum Exp Toxicol 13:131–134
Jacobsen D, Jansen H, Wiik-Larsen E, Bredesen JE, Halvorsen S (1982) Studies on methanol poisoning. Acta Med Scand 212:5–10
Hojer J (1996) Severe metabolic acidosis in the alcoholic: differential diagnosis and management. Hum Exp Toxicol 15:482–488
Jacobsen D, Webb R, Collins TD, McMartin KE (1988) Methanol and formate kinetics in late diagnosed methanol intoxication. Med Toxicol Adverse Drug Exp 3:418–423
Sulway MJ, Malins JM (1970) Acetone in diabetic ketoacidosis. Lancet 2:736–740
Cooperman MT, Davidoff F, Spark R, Pallotta J (1974) Clinical studies of alcoholic ketoacidosis. Diabetes 23:433–439
Sklar AH, Linas SL (1983) The osmolal gap in renal failure. Ann Intern Med 98:481–482
Boyd DR, Folk FA, Condon RE, Nyhus LM, Baker RJ (1970) Predictive value of serum osmolality in shock following major trauma. Surg Forum 21:32–33
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hovda, K.E., Hunderi, O.H., Rudberg, N. et al. Anion and osmolal gaps in the diagnosis of methanol poisoning: clinical study in 28 patients. Intensive Care Med 30, 1842–1846 (2004). https://doi.org/10.1007/s00134-004-2373-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-004-2373-7