
Abstract
The distribution and quantity of adipose tissue are markers of morbidity risk in children and adults. Poor intrauterine growth and accelerated postnatal growth are believed to add to these risks. The aim of this study was to assess adipose tissue content and distribution at birth and 6 wk in relation to intrauterine growth restriction, postnatal growth, and infant diet. We measured weight, length, and head circumference and adipose content and distribution using magnetic resonance imaging at 6 wk of age in appropriately grown for gestational age (AGA) and growth-restricted (GR) infants and compared this with birth data. By 6 wk, GR infants showed complete catch-up in comparison to AGA infants in relation to head growth and adiposity. Catch-up in length and weight was not complete. Accelerated linear growth, but not accelerated weight gain, was associated with a highly significant increase in adiposity (r = 0.57, p = 0.001) regardless of AGA/GR status. The highest adiposity at 6 wk, allowing for baseline variables and linear growth, was seen in exclusively breast-fed GR infants (mean, 95% confidence interval: 33.5%, 29.51–37.5). Adipose tissue distribution remained constant and was unrelated to growth and diet. Reduced birth adiposity (B = –0.185, p = 0.003), but not low birth head size (B = 0.32, p = 0.093), was a significant predictor of accelerated postnatal head growth (R2 = 0.29, adjusted R2 = 0.23, p = 0.012). Increasing adiposity appears to be an inevitable accompaniment of accelerated linear growth. Low total adipose tissue quantity at birth appears to direct nutrition toward head growth. Adipose tissue may be involved in the signaling of catch-up growth.
Similar content being viewed by others

Main
Epidemiologic observations suggest that small size at birth and accelerated postnatal growth are risk factors for obesity in later life (1,2), but how this is mediated is unknown (3). We have shown that MR imaging can be used in the assessment of AT content and distribution in neonates (4–6). We have previously presented data on AT content and distribution in healthy full-term newborns (4). We now present the results of follow-up examinations to 6 wk of age in the same cohort of infants. Our primary aim was to assess the change in AT content and distribution in relation to intrauterine growth restriction, postnatal growth, and infant diet
METHODS
Mothers receiving antenatal care at Queen Charlotte's & Chelsea Maternity Hospital, London, UK, were invited to consider joining the study. Written, informed parental consent was sought after the birth of the infant. Infants were considered eligible for inclusion if healthy and born at term. The study was approved by the Hammersmith Hospitals Trust and Imperial College Faculty of Medicine Research Ethics Committee.
Infants were imaged in the first week after birth and again at 6 wk of age. Weight (kg), length (cm), and head circumference (cm) were recorded at each examination by one of two trained observers. Each infant was weighed naked on an electronic scale (Marsden Professional Baby Scale, Oxfordshire, U.K.; precision ±2 g). Crown-heel length was measured on a recumbent infant board with a sliding footboard (Rollametre, Raven Equipment Ltd, Dunmow, U.K.). Head circumference was measured using a plastic tape measure and the mean of three measurements was calculated. Anthropometric measurements were expressed as SDS calculated using commercially available software based upon the UK 1990 Growth Reference data (http://www.childgrowthfoundation.org/). Growth rate between birth and 6 wk was expressed as weight SDS Gain and length SDS Gain calculated using the same software. SDS Gain is the change in SDS adjusted for sex and correlations between measurements at two time points (7). A SDS Gain of zero indicates that the infant has remained on the same growth centile and a positive SDS Gain indicates accelerated growth. Infant diet was coded at 6 wk as exclusively breast-fed, breast-and formula-fed, and exclusively formula-fed.
MR imaging.
Infants were imaged in a 1.5T Marconi Medical System Eclipse scanner (Philips Medical Systems, Reigate, U.K.) using a T1-weighted spin-echo image sequence. No sedation was used and infants were positioned supine during natural sleep. The serial isocenter technique is used in which the infant is moved through the magnet on a mobile platform for full body imaging. Images are obtained with a slice and interslice thickness of 5 mm. Image analysis has been described previously (4). The image segmentation software program employs a threshold range and a contour following algorithm with an interactive image editing facility. SCAT and internal adipose tissue (IAT) depots were quantified and summated to derive total AT volume. Internal adipose tissue was subdivided into IAIAT and nonabdominal internal compartments. IAIAT content was that contained in the slices from the sacrum to the top of the liver or base of the lungs. Adipose tissue volume derived from the analysis of the MR images was converted to adipose tissue mass (ATM) (4). We calculated LBM as body weight – ATM. Adipose tissue distribution was expressed at the ratio of IAIAT to SCAT.
Statistical analyses.
Data were analyzed using SPSS, version 13 (http://www.spss.com/). Unless otherwise stated, values are presented as mean and SD. Data were analyzed for the group as a whole and in relation to clinical assignment at birth as either AGA or GR, with the latter as previously defined (4), namely with evidence of deceleration in growth in utero, together with clinical signs at birth suggestive of fetal malnutrition (loose thin skin with prominent ribs, a scaphoid abdomen, and muscle wasting over the cheeks, arms, buttocks, and thighs) and a birth weight at or below the 9th centile. Residuals were tested for normality and to detect the presence of outliers. The independent samples t test was used to examine between group differences in adiposity and adipose tissue distribution. ANOVA was used to allow for size at birth, postnatal growth, and infant diet. Multiple regression analysis was used to explore the determinants of adiposity and adipose tissue distribution at 6 wk. Evidence of an interaction between AGA/GR status and exclusive breast-feeding on adiposity at 6 wk was sought.
Expression of total body adiposity.
Traditionally total adiposity has been expressed as a percentage of body weight (W). Although easily comprehensible, the validity of this index (ATM/W) has been criticized (8). The aim of expressing one variable in relation to another is to remove the effect of the latter, so that the derived index is independent of the denominator. It is also important to select a denominator that is appropriate for the numerator to be adjusted against. As ATM appears in the numerator and in the denominator, the index ATM/W will be highly correlated with W. In addition, the best way to indicate the metabolic load presented by a given ATM might be to express it in relation to LBM. We therefore also used the method recommended by Wells and Victora (8) to minimize the correlation between any index A/B and the raw denominator B. We performed log-log (natural log to the base e) regression analysis of the variables ATM on LBM, and W on length (L). The regression coefficients were significantly different from unity and were therefore used to calculate the indices ATM/LBMp and W/Lp, where p is the relevant regression coefficient. We used linear and multiple regression to determine the effect of length SDS Gain and weight SDS Gain on these indices at 6 wk, allowing for the index at birth.
RESULTS
Thirty-five singleton infants were imaged within 5 d of birth (25 AGA and 10 GR) and, of these, 29 (21 AGA, 8 GR) of whom 16 were boys and 13 were girls, were imaged again at 6 wk of age. Of the remaining six infants, three did not settle for the follow-up imaging and, for three, their parents declined to return for repeat assessment. Twelve infants were exclusively breast-fed (9 AGA, 3 GR), 9 were exclusively formula-fed (6 AGA, 3 GR), and 8 received mixed breast/formula feeds (6 AGA, 2 GR).
Birth data in relation to GR and AGA phenotypes for the 29 infants assessed at 6 wk are presented in Table 1. At birth, the GR infants were lighter, shorter, had smaller head circumferences (HC), and had less adipose tissue than the AGA infants. Differences in anthropometric indices were still evident at 6 wk of age when GR infants remained significantly lighter and shorter than the AGA infants (Table 2). However, the highly significant difference in HC and %ATM present at birth was no longer evident. Adipose tissue distribution (IAIAT/SCAT) did not differ between AGA and GR infants at birth or at 6 wk.
We found a highly significant correlation between %ATM at 6 wk and length SDS Gain (r = 0.71, p < 0.001). Adipose tissue distribution (IAIAT/SCAT) was uninfluenced by length SDS Gain (r = –0.31, p = 0.103).
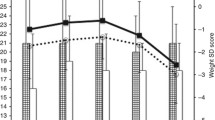
The regression coefficient (95% CI), p, for ATM/LBMp was 1.9 (1.6 to 2.1), and for W/Lp, 3.7 (3.3 to 4.0). Linear regression analysis showed a highly significant relationship between the index ATM/LBM1.9 at 6 wk and length SDS Gain (Fig. 1, r = 0.57, p = 0.001), but not with weight SDS Gain (r = 0.27, p = 0.16). The relationship between ATM/LBM1.9 at 6 wk and length SDS Gain remained significant following adjustment for the baseline index, ATM/LBM1.9, at birth (B = 0.016, p < 0.001, adjusted R2 = 0.45). The index of weight for length at 6 wk, W/L3.7, showed no significant relationship to length SDS Gain (r = –0.21, p = 0.29).

ATM/LBM1.9 by length SDS Gain at 6 wk. ATM/LBM1.9 = 0.12 + length SDS Gain * 0.015 (r = 0.57; adjusted R2 = 0.30; p = 0.001).
Greater than 80% of the variance in %ATM at 6 wk (R2 = 0.876, adjusted R2 = 0. 826, p < 0.001) was explained by length SDS Gain (B = 2.58, p < 0.001, R2 = 0.393), %ATM at birth (B = 0.44, p = 0.002, R2 = 0.289), and the interaction between GR status and exclusive breast-feeding (B = 11.08, p < 0.001, R2 = 0.158), having allowed for length SDS at birth, growth status, and feed type, with these latter three variables contributing only 3.6% to the total variance. The highest % ATM at 6 wk (mean, 95% CI: 33.5%, 29.5 to 37.5), allowing for length SDS Gain, %ATM at birth and length SDS at birth was seen in GR infants who were exclusively breast-fed (Table 3).
Reduced birth %ATM (B = –0.185, p = 0.003), but not low birth head size (B = 0.32, p = 0.093), was a significant predictor of accelerated postnatal head growth (R2 = 0.29, adjusted R2 = 0.23, p = 0.012).
These conclusions were unaltered when the analyses were repeated expressing adiposity as ATM/LBM1.9.
DISCUSSION
We have shown by direct measurement in healthy human infants that the rate of deposition of AT exceeds that of LBM during accelerated linear growth. We showed this using the traditional means of expressing adiposity, namely as a percentage of body weight. We then confirmed this relationship when we utilized a robust method of analysis that minimized any correlation between the numerator (ATM) and the denominator (LBM). To our knowledge, this study provides the first longitudinal data on total adiposity and AT distribution in early infancy.
Accelerated weight gain has been linked with increasing adiposity in epidemiologic research, but the methods of analysis used previously have precluded the ability to separate out the influence of accelerated weight gain and accelerated length gain. Our analysis has clearly shown that the relationship is with length.
Although it is not known how accelerated growth is signaled, our data indicate that as an infant accelerates in linear growth s/he will inevitably become more adipose. This does not equate with becoming “fat” in the popular sense of the word, as weight for length did not increase with accelerated growth. It is not generally appreciated that whole body adiposity can vary widely in nonobese subjects (9). However, a more adipose body composition is likely to increase susceptibility to the subsequent superimposition of dietary and life style factors that lead to metabolic ill health. Our unique observation thus suggests an explanation for the known association between accelerated or “catch-up” growth and later insulin resistance, dyslipidemia, and other components of the metabolic syndrome (10).
The physiologic and cellular determinants of catch-up growth have not been elucidated. Two hypotheses have been proposed. In the neuroendocrine hypothesis, proposed by Tanner (11), it is suggested that a CNS-based mechanism exists that compares actual size against an age-appropriate set point and then alters growth rate accordingly. A second model (12) suggests that during growth inhibition there is decreased proliferation of growth plate stem cells, thus delaying senescence and preserving their potential for future growth. Firm supportive experimental data are inadequate for either of these hypotheses. Our results suggest a new hypothesis, namely that the deposition of adipose tissue is fundamentally involved in the signalling of catch-up growth.
GR infants remained shorter and lighter at 6 wk than AGA infants. This was in marked contrast to head growth and adiposity where the highly significant differences present at birth were no longer evident at 6 wk. “Head sparing,” where brain growth is conserved during nutrient restriction, is well recognized. These data demonstrate the converse, namely that catch-up in brain growth takes precedence over somatic growth. What is intriguing is that catch-up in adiposity also appeared to take precedence over restoration of weight and length. Accelerated head growth was predicted by reduced adiposity at birth but, surprisingly, not by low birth head size. These findings also lead us to suggest that the deposition of AT, a metabolically active organ, may be critical to the regulation of growth in infancy. The deposition of AT during intrauterine development is an almost uniquely human phenomenon (13), not even occurring in nonhuman primates. Our observations suggesting a crucial role for AT during early development are in accord with the argument that human evolution was driven by the emergence of genes that favored the deposition of AT, providing a reliable, stable source of energy to support the development of the metabolically demanding modern human brain (14).
Our data also indicate an effect of exclusive breast-feeding in favor of increased adiposity in the GR infant. Breast-feeding is associated with improved metabolic outcomes in later life (15,16), and it has been suggested that this may be a consequence of reduced adiposity (17). Our study is small and our observations require confirmation. However, if increased total adiposity in GR, exclusively breast-fed infants is confirmed, the causal pathway linking breast-feeding and metabolic health must be mediated by other factors yet to be understood.
Our data have wider potential implications. There has been a secular increase in height over successive generations in the last century (18). To achieve a greater adult height, childhood growth must be faster. Our data raise a possibility never previously considered: namely, that there has also been a secular change in body composition accompanying the secular increase in height over the last decades. If there has been a shift toward an increasingly adipose body composition as population height has moved upward, this may have increased susceptibility to lifestyle and dietary antecedents that have in turn underpinned the present-day epidemic of obesity-related morbidities.
Accelerated growth implies escape from previous restraint. If our inferences are correct, improved conditions in fetal life and infancy will in time reverse this trend and, in countries where trans-generational increases in height have stabilized, the rise in the prevalence of obesity and related disorders should be slowing. There is some evidence that this is indeed occurring (19). Further, children who have achieved a given height for weight without a period of accelerated growth would have a less adipose body composition than those who have achieved the same height for weight after a period of accelerated growth. Although our inferences are speculative, the hypotheses raised can be tested. Our data open up new directions for epidemiologic research.
Abbreviations
- AT:
-
adipose tissue
- AGA:
-
appropriate for gestational age
- GR:
-
growth restricted
- IAIAT:
-
intra-abdominal adipose tissue
- LBM:
-
lean body mass
- MR:
-
magnetic resonance
- SCAT:
-
subcutaneous adipose tissue
- SDS:
-
standard deviation score
- SDS Gain:
-
standard deviation score gain
- W:
-
weight
References
Ong KK, Ahmed ML, Emmett PM, Preece MA, Dunger DB 2000 Association between postnatal catch-up growth and obesity in childhood: prospective cohort study. BMJ 320: 967–971
Reilly JJ, Armstrong J, Dorosty AR, Emmett PM, Ness A, Rogers I, Steer C, Sherriff A 2005 Avon Longitudinal Study of Parents and Children Study Team. Early life risk factors for obesity in childhood: cohort study. BMJ 330: 1357–1363
Ozanne SE, Hale CN 2004 Lifespan: catch-up growth and obesity in male mice. Nature 427: 411–412
Harrington TA, Thomas EL, Frost G, Modi N, Bell J 2004 Distribution of adipose tissue in the newborn. Pediatr Res 55: 437–441
Harrington TA, Thomas EL, Modi N, Frost G, Coutts GA, Bell JD 2002 Fast and reproducible method for the direct quantitation of adipose tissue in newborn infants. Lipids 37: 95–100
Uthaya S, Thomas EL, Hamilton G, Bell J, Modi N 2005 Altered adiposity after extremely preterm birth. Pediatr Res 57: 211–215
Cole TJ 1995 Conditional reference charts to assess weight gain in British infants. Arch Dis Child 73: 8–16
Wells JC, Victora CG 2005 Indices of whole-body and central adiposity for evaluating the metabolic load of obesity. Int J Obes (Lond) 29: 483–489
Thomas EL, Saeed N, Hajnal JV, Brynes A, Goldstone AP, Frost G, Bell JD 1998 Magnetic resonance imaging of total body fat. J Appl Physiol 85: 1778–1785
Jaquet D, Deghmoun S, Chevenne D, Collin D, Czernichow P, Levy-Marchal C 2005 Dynamic change in adiposity from fetal to postnatal life is involved in the metabolic syndrome associated with reduced fetal growth. Diabetologia 48: 849–855
Tanner JM 1963 Regulation of growth in size in mammals. Nature 199: 845–850
Baron J, Klein KO, Colli MJ, Yanovski JA, Novosad JA, Bacher JD, Cutler GB Jr 1994 Catch-up growth after glucocorticoid excess: a mechanism intrinsic to the growth plate. Endocrinology 135: 1367–1371
Widdowson EM 1974 Changes in body proportion and composition during growth. In: Davies JA, Dobbing J (eds) Scientific Foundations of Pediatrics. Heinemann, London, pp 153–163
Cunnane SC, Crawford MA 2003 Survival of the fattest: fat babies were the key to evolution of the large human brain. Comp Biochem Physiol A Mol Integr Physiol 136: 17–26
Ravelli AC, van der Meulen JH, Osmond C, Barker DJ, Bleker OP 2000 Infant feeding and adult glucose tolerance, lipid profile, blood pressure, and obesity. Arch Dis Child 82: 248–252
Singhal A, Cole TJ, Fewtrell M, Lucas A 2004 Breast-milk feeding and lipoprotein profile in adolescents born preterm: follow-up of a prospective randomised study. Lancet 363: 1571–1578
Dewey KG 2003 Is breastfeeding protective against child obesity?. J Hum Lact 19: 9–18
Cole TJ 2003 The secular trend in human physical growth: a biological view. Econ Hum Biol 1: 161–168
Heitmann BL, Stroger U, Mikkelsen KL, Holst C, Sorensen TI 2004 Large heterogeneity of the obesity epidemic in Danish adults. Public Health Nutr 7: 453–460
Acknowledgements
The authors thank Wilfredo Quiroz Pereira for assistance in this study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported by the Medical Research Council (UK).
Rights and permissions
About this article
Cite this article
Modi, N., Thomas, E., Harrington, T. et al. Determinants of Adiposity during Preweaning Postnatal Growth in Appropriately Grown and Growth-Restricted Term Infants. Pediatr Res 60, 345–348 (2006). https://doi.org/10.1203/01.pdr.0000232732.93000.52
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/01.pdr.0000232732.93000.52
- Springer Nature America, Inc.
This article is cited by
-
Growth of exclusively breastfed small for gestational age term infants in the first six months of life: a prospective cohort study
BMC Pediatrics (2022)
-
Impact of very preterm birth and post-discharge growth on cardiometabolic outcomes at school age: a retrospective cohort study
BMC Pediatrics (2021)
-
The mysterious values of adipose tissue density and fat content in infants: MRI-measured body composition studies
Pediatric Research (2021)
-
Early postnatal alteration of body composition in preterm and small-for-gestational-age infants: implications of catch-up fat
Pediatric Research (2015)
-
Height, adiposity and hormonal cardiovascular risk markers in childhood: how to partition the associations?
International Journal of Obesity (2014)