
Abstract
Background
Loss of synaptic functionality has been recently identified as an early-stage indicator of neurological diseases. Consequently, monitoring changes in synaptic protein levels may be relevant for observing disease evolution or treatment responses in patients. Here, we have studied the relationship between fluid biomarkers of neurodegeneration and synaptic dysfunction in patients with Alzheimer’s disease (AD), frontotemporal dementia (FTD), and subjective cognitive decline (SCD).
Methods
The exploratory cohort consisted of cerebrospinal fluid (CSF) samples (n = 60) from patients diagnosed with AD (n = 20), FTD (n = 20), and SCD (n = 20) from the Amsterdam Dementia Cohort. We developed two novel immunoassays for the synaptic proteins synaptosomal-associated protein-25 (SNAP25) and vesicle-associated membrane protein-2 (VAMP2). We measured the levels of these biomarkers in CSF, in addition to neuronal pentraxin-2 (NPTX2), glutamate ionotropic receptor-4 (GluR4), and neurogranin (Ng) for this cohort. All in-house immunoassays were validated and analytically qualified prior to clinical application. CSF neurogranin (Ng) was measured using a commercially available ELISA.
Results
This pilot study indicated that SNAP25, VAMP2, and Ng may not be specific biomarkers for AD as their levels were significantly elevated in patients with both AD and FTD compared to SCD. Moreover, the strength of the correlations between synaptic proteins was lower in the AD and FTD clinical groups compared to SCD. SNAP25, VAMP2, and Ng correlated strongly with each other as well as with total Tau (Tau) and phosphorylated Tau (PTau) in all three clinical groups. However, this correlation was weakened or absent with NPTX2 and GluR4. None of the synaptic proteins correlated to neurofilament light (NfL) in any clinical group.
Conclusion
The correlation of the synaptic biomarkers with CSF Tau and PTau but the lack thereof with NfL implies that distinct pathological pathways may be involved in synaptic versus axonal degeneration. Our results reflect the diversity of synaptic pathology in neurodegenerative dementias.
Similar content being viewed by others


Background
Alzheimer’s disease (AD) and frontotemporal dementia (FTD) are two of the most prevalent causes of dementia among the elderly. AD is a slow-progressing neurodegenerative disorder that is primarily characterized by memory and cognitive impairments while FTD is a largely heterogeneous disorder that manifests as behavioral changes, language impairment, motor symptoms, or even psychiatric disorders [1,2,3]. The pathological signature of AD is amyloid beta (Aβ) plaque accumulation in the neocortex of the brain, while in FTD, there is degeneration of the frontal and temporal lobes, including in para-limbic areas [4, 5].
Synaptic dysfunction and loss of synaptic plasticity are fundamental processes that underlie several neurodegenerative disorders from early stages. In fact, synaptic pathology has been identified in pre-clinical stages of AD, FTD, dementia with Lewy bodies, and Parkinson’s disease, as well as certain psychiatric disorders [5,6,1–2 and Supplementary Figs. 1–4.
VAMP2 ELISA
The VAMP2 CSF sandwich ELISA had an LLOQ of 127 pg/mL. The mean intra-assay and inter-assay %CV were 4.1% and 4.8% respectively; thus, the assay is highly precise. The mean dilutional linearity of the three CSF samples was 110%, which was well within the acceptability criteria. Furthermore, mean parallelism of 103% with a 7% standard deviation (SD) was observed, thereby indicating minimal CSF matrix effects in the assay. Lastly, the CSF samples had a percentage recovery within 80 to 120% up to four freeze–thaw cycles, implying that the analyte remains stable with multiple freeze-thaws (Supplementary Fig. 5A).
SNAP25 Simoa
The SNAP25 CSF Simoa assay had an LLOQ of 2.91 pg/mL. The mean intra-assay and inter-assay %CV were 10.2% and 10.9% respectively, both being well within the accepted limit. Three CSF samples were spiked with 200 pg of calibrator protein and serially diluted up to a dilution factor of 98. The mean dilutional linearity of the samples was found to be 106%, which is within the acceptability criteria. The mean parallelism for five CSF samples was 89% which represents minimal matrix effects in the assay. A minor 0.6% negative drift effect was observed for the CSF signals after 3 h 45 min of sample incubation, indicating potential instability of the analyte upon long incubation periods (Supplementary Fig. 5B). This was mitigated by limiting the sample incubation time to 20 min and placing calibrators and run-validation samples at the beginning and end of the immunoassay well plates.
Levels of synaptic proteins SNAP25, VAMP2, and Ng are elevated in CSF of patients with AD and FTD
As expected, the core neuronal biomarkers in CSF: Tau, PTau, and NfL, were able to differentiate significantly between the clinical groups of AD, FTD, and SCD (Supplementary Fig. 6B–D). CSF Aβ42 was significantly decreased in patients with AD compared to FTD and SCD, but could not differentiate between the clinical groups FTD and SCD (Supplementary Fig. 6A).
Patients in both the AD and FTD groups had significantly higher levels of CSF SNAP25, VAMP2, and Ng compared to the SCD group (Fig. 2A–C). Among these, SNAP25 levels alone were significantly elevated in AD compared to FTD. Furthermore, FTD patients had significantly lower NPTX2 levels than the SCD group (Fig. 2D). However, we did not find a differential expression of the synaptic biomarker GluR4 in any clinical group within this cohort (Fig. 2E). All patients in this cohort had CSF SNAP25, VAMP2, Ng, NPTX2, and GluR4 levels above the detection limit of the immunoassays used.

Scatter plot of the synaptic CSF fluid biomarkers in the three diagnostic groups AD (n = 20), FTD (n = 20), and SCD (n = 20). The biomarker values were log-transformed to fit a normal distribution and the model corrected for age and sex prior to conducting pairwise multiple comparisons. A SNAP25, B VAMP2, C Ng, D NPTX2, and E GluR4. *P < 0.05, **P < 0.01, ***P < 0.001
Diagnostic potential of the synaptic biomarkers and selection of panels for differential diagnosis
We have visualized the diagnostic value of each synaptic biomarker for differentiating between the clinical group AD vs SCD, FTD vs SCD, and AD vs FTD (Fig. 3A–C; Table 3). SNAP25 (AUC = 0.99) had the greatest diagnostic value for differentiating AD vs SCD patients, followed by Ng (AUC = 0.87) and VAMP2 (AUC = 0.82). No significant AUC was observed for NPTX2 (AUC = 0.62) or GluR4 (AUC = 0.60). The biomarker panel selection consisted of SNAP25 alone (AUC = 0.99). A similar trend was observed for the biomarkers while comparing the clinical groups FTD vs SCD where the synaptic proteins had significant diagnostic values as follows: SNAP25 (AUC = 0.83), Ng (AUC = 0.79), VAMP2 (AUC = 0.77), NPTX2 (AUC = 0.70). The selected synaptic biomarker panel with the highest AUC consisted of VAMP2 and NPTX2 (AUC = 0.97). Interestingly, between the clinical group AD vs FTD, none of the synaptic biomarkers except SNAP25 (AUC = 0.75) showed significant diagnostic value. The identified biomarker panel consisted of SNAP25 and VAMP2 and had a higher AUC than the individual biomarkers (AUC = 0.84).

ROC curves and AUC values of the synaptic CSF biomarkers among the clinical groups. A AD versus SCD. B FTD versus SCD. C AD versus FTD. ROC, receiver operating characteristics, AUC, area under the curve. *P < 0.05, **P < 0.01, ***P < 0.001
Synaptic biomarkers revealed a differential association with classical fluid biomarkers
The correlation matrix of the CSF biomarkers is presented in Fig. 4. In the SCD group, synaptic proteins were all well correlated (Pearson, r = 0.92–0.49), although no significant correlations were found between GluR4 and Ng or NPTX2. However, the strength of these correlations were reduced (Pearson, r = 0.73–0.58) and often not significant in the AD and FTD clinical groups. Furthermore, we did not find a correlation of the axonal biomarker NfL to any synaptic biomarker within this cohort.

Correlation matrix of the CSF biomarkers. Pearson’s correlation was used as all the biomarkers were log-transformed to fit a normal distribution. The significant correlations are indicated in bold. *P < 0.05, **P < 0.01, ***P < 0.001
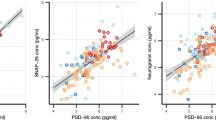
The presynaptic vesicle proteins, SNAP25 and VAMP2, correlated with each other as well as with Tau, PTau, and Ng (Pearson, r = 0.94–0.55) in all three clinical groups. Moreover, the postsynaptic biomarker Ng correlated with SNAP25, VAMP2, and NPTX2 (Pearson, r = 0.73–0.49) in all the clinical groups. In the SCD group, GluR4 had a significant association with SNAP25 and VAMP2 (Pearson, r = 0.60–0.59), although this association was not present in the AD or FTD clinical groups. Interestingly, all CSF biomarkers (except NfL) had a significant correlation with Aβ42 in the SCD group (Pearson, r = 0.73–0.46), although this correlation was lost in the other clinical groups.
Association of the synaptic biomarkers with cognitive scores of patients
The correlation matrix of the CSF biomarkers with the cognitive (MMSE) scores of patients is presented in Fig. 5, and the scatter plots of these correlations are shown in Supplementary Fig. 8. We found that in the overall cohort, the biomarkers SNAP25 (Spearman, r = − 0.57, P < 0.001), VAMP2 (Spearman, r = − 0.48, P < 0.001), and Ng (Spearman, r = − 0.52, P < 0.001) were negatively correlated with the MMSE scores of the patients, indicating that an increase in these synaptic protein concentrations in CSF was associated with decreasing cognition. Upon stratification for clinical diagnosis, NPTX2 in AD patients correlated moderately with their MMSE scores (Spearman, r = 0.55, P = 0.012). No other associations of the synaptic biomarkers with cognitive scores were detected in the stratified cohort.

Correlation matrix of the CSF biomarkers with MMSE scores in the entire cohort and upon stratification into the clinical groups. Spearman’s correlation was used as MMSE scores were not normally distributed even after log transformation. The significant correlations are indicated in bold. *P < 0.05, **P < 0.01, ***P < 0.001
Discussion
We measured the concentration of the synaptic proteins SNAP25, VAMP2, Ng, NPTX2, and GluR4 in the CSF of patients with AD, FTD, and SCD. We have shown that both AD and FTD patients have an elevated expression of SNAP25, VAMP2, and Ng compared to SCD, while NPTX2 levels are lower in FTD compared to SCD. Herein, we also reported the development and clinical validation of two novel immunoassays for the SNARE complex proteins SNAP25 and VAMP2. Synaptic proteins involved in diverse functional aspects and localizations were assessed in this cohort as a first attempt to highlight the diversity in synaptic pathology and overlap** pathologies in patients with AD and FTD. Additionally, we observed a differential degree of correlation among the synaptic proteins in AD, FTD, and SCD, which provides proof of concept that synaptic protein levels and their co-expressions are altered in different disease states. The association of each synaptic protein with the classical fluid biomarkers Aβ42, Tau, PTau, and NfL as well as with the cognitive scores of patients was investigated.
To our knowledge, this is the first clinical cohort to report that the CSF synaptic proteins SNAP25 and VAMP2 are elevated in FTD patients and are not specific to AD. In a recent study consisting of neuropathology-confirmed FTD patients, VAMP2 was not found to be significantly increased for FTD compared to controls, although an increasing trend was detected [29]. Although Ng is primarily known to be an AD-specific biomarker, we found that Ng levels, compared to SCD patients, were also significantly elevated in both AD and FTD patients but failed to significantly distinguish these two clinical groups. Similar results have been reported in a previous cohort consisting of AD and FTD patients [30]. The plausible reasons for the lack of differential CSF profiles of synaptic proteins in the two disease groups could be the heterogeneity of FTD as a disease, its co-pathologies with AD and other dementias, or the sheer underrepresentation of FTD in clinical cohorts due to misclassification [10, 31,32,33]. Furthermore, it has been suggested that the implied AD specificity of Ng could be a result of selection bias in cohorts. This is because clinical samples are often stratified based on their Tau levels, and Ng is a biomarker that consistently correlates to high Tau and PTau levels, as we see in our cohort too [34].
NPTX2 reportedly has predictive value for patients with genetic FTD [33, 34]. In this cohort, the NPTX2 levels were significantly lower in FTD patients compared to SCD. However, the FTD patients were not stratified based on their genetic diversity or disease severity, and the lack of differential expression of NPTX2 between AD and FTD could possibly be due to the heterogeneity of these FTD patients. Another notable outcome was that the CSF GluR4 levels were comparable across the clinical groups in this cohort. GluR4 was recently identified as a biomarker that demonstrates preclinical changes in AD patients before neurodegeneration and Tau pathology, although the diagnostic and prognostic value of this AMPA receptor complex protein remains to be evaluated in depth [5, 8, 9, 11]. Herein, we found proof of concept that synaptic pathology is diverse and individual synaptic proteins reflect different aspects of synaptic dysfunction, which is distinct from broad-spectrum neurodegeneration as reflected by changes in Tau, PTau, and NfL. Although limitations of this cohort could arise from the small sample size of each clinical group as well as the heterogeneity within the FTD group, our findings warrant further explorations of synaptic proteins in larger and more diverse clinical cohorts, using immunoassay technologies.
Conclusions
This pilot study indicated that the synaptic biomarkers SNAP25, VAMP2, and Ng were not specific for AD, as they were also elevated in the heterogeneous FTD group compared to SCD. The stronger correlations of the CSF biomarkers in the SCD group compared to the disease groups implied distinct synaptic pathology that may be characteristic of the AD and FTD disease states. Our study also re-iterated recent findings suggesting that CSF synaptic biomarkers reveal neuropathologies that are possibly distinct from broad-spectrum axonal degeneration as exhibited by NfL. In conclusion, these diverse synaptic biomarkers hold promise for understanding the pathophysiological states of different dementias.
Availability of data and materials
Anonymized data can be made available upon reasonable request and upon consultation with the involved biobanks. Additional datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- Aβ:
-
Amyloid beta
- AD:
-
Alzheimer’s disease
- CSF:
-
Cerebrospinal fluid
- FTD:
-
Frontotemporal dementia
- GluR4:
-
Glutamate ionotropic receptor-4
- MMSE:
-
Mini-mental state examination
- NfL:
-
Neurofilament light
- Ng:
-
Neurogranin
- NPTX2:
-
Neuronal pentraxin-2
- PTau:
-
Phosphorylated Tau
- SCD:
-
Subjective cognitive decline
- SNAP25:
-
Synaptosomal associated protein-25
- Simoa:
-
Single molecular array
- Tau:
-
Total Tau
References
Sogorb-Esteve A, Nilsson J, Swift IJ, Heller C, Bocchetta M, Russell LL, et al. Differential impairment of cerebrospinal fluid synaptic biomarkers in the genetic forms of frontotemporal dementia. Alzheimers Res Ther. 2022;14(1):118-.
Jagust W. Integrating events in the disintegration of Alzheimer's disease. Brain. 2021;144(1):11–4. https://doi.org/10.1093/brain/awaa402.
Mantzavinos V, Alexiou A. Biomarkers for Alzheimer’s disease diagnosis. Curr Alzheimer Res. 2017;14(11):1149–54.
Breijyeh Z, Karaman R. Comprehensive review on Alzheimer's disease: causes and treatment. Molecules. 2020;25(24):5789. https://doi.org/10.3390/molecules25245789.
Lleó A, Núñez-Llaves R, Alcolea D, Chiva C, Balateu-Paños D, Colom-Cadena M, et al. Changes in synaptic proteins precede neurodegeneration markers in preclinical Alzheimer’s disease cerebrospinal fluid*. Mol Cell Proteomics. 2019;18(3):546–60.
Lleó A, Parnetti L, Belbin O, Wiltfang J. Has the time arrived for cerebrospinal fluid biomarkers in psychiatric disorders? Clin Chim Acta. 2019;491:81–4.
Van Der Ende EL, **ao M, Xu D, Poos JM, Panman JL, Panman JL, et al. Neuronal pentraxin 2: a synapse-derived CSF biomarker in genetic frontotemporal dementia. J Neurol Neurosurg Psychiatry. 2020;91(6):612–21.
Shimohama S, Kamiya S, Taniguchi T, Akagawa K, Kimura J. Differential involvement of synaptic vesicle and presynaptic plasma membrane proteins in Alzheimer’s disease. 1997.
Kivisäkk P, Carlyle BC, Sweeney T, Quinn JP, Ramirez CE, Trombetta BA, et al. Increased levels of the synaptic proteins PSD-95, SNAP-25, and neurogranin in the cerebrospinal fluid of patients with Alzheimer’s disease. Alzheimers Res Ther. 2022;14(1):58-.
Clarke MTM, Brinkmalm A, Foiani MS, Woollacott IOC, Heller C, Heslegrave A, et al. CSF synaptic protein concentrations are raised in those with atypical Alzheimer’s disease but not frontotemporal dementia. Alzheimers Res Ther. 2019;11(1):105.
Brinkmalm G, Sjödin S, Simonsen AH, Hasselbalch SG, Zetterberg H, Brinkmalm A, Blennow K. A parallel reaction monitoring mass spectrometric method for analysis of potential CSF biomarkers for Alzheimer's disease. Proteomics Clin Appl. 2018;12(1):1700131. https://doi.org/10.1002/prca.201700131.
Blennow K, Zetterberg H. Biomarkers for Alzheimer’s disease: current status and prospects for the future. J Intern Med. 2018;284(6):643–63 Blackwell Publishing Ltd.
Molinuevo JL, Ayton S, Batrla R, Bednar MM, Bittner T, Cummings J, et al. Current state of Alzheimer’s fluid biomarkers. Acta Neuropathol. 2018;136(6):821–85.
Clare R, King VG, Wirenfeldt M, Vinters HV. Synapse loss in dementias. J Neurosci Res. 2010;88:2083–90 Wiley-Liss Inc.
Wang C, Tu J, Zhang S, Cai B, Liu Z, Hou S, et al. Different regions of synaptic vesicle membrane regulate VAMP2 conformation for the SNARE assembly. Nat Commun. 2020;11(1):1531.
Cervantes González A, Belbin O. Fluid markers of synapse degeneration in synucleinopathies. J Neural Transm. 2022;129(2):187–206 Springer.
Nilsson J, Gobom J, Sjödin S, Brinkmalm G, Ashton NJ, Svensson J, et al. Cerebrospinal fluid biomarker panel for synaptic dysfunction in Alzheimer’s disease. Alzheimers Dement. 2021;13(1):e12179.
Andreasson U, Perret-Liaudet A, van Waalwijk van Doorn LJC, Blennow K, Chiasserini D, Engelborghs S, et al. A practical guide to immunoassay method validation. Front Neurol. 2015;6:179.
Van Der Flier WM, Scheltens P. Amsterdam dementia cohort: performing research to optimize care. J Alzheimers Dis. 2018;62(3):1091–111.
Willemse EAJ, van Maurik IS, Tijms BM, Bouwman FH, Franke A, Hubeek I, et al. Diagnostic performance of Elecsys immunoassays for cerebrospinal fluid Alzheimer’s disease biomarkers in a nonacademic, multicenter memory clinic cohort: the ABIDE project. Alzheimers Dement (Amst). 2018;10:563–72.
del Campo M, Peeters CFW, Johnson ECB, Vermunt L, Hok-A-Hin YS, van Nee M, et al. CSF proteome profiling across the Alzheimer’s disease spectrum reflects the multifactorial nature of the disease and identifies specific biomarker panels. Nature Aging. 2022;2(11):1040–53.
van Engelen ME, Gossink FT, de Vijlder LS, Meursing JRA, Scheltens P, Dols A, et al. End stage clinical features and cause of death of behavioral variant frontotemporal dementia and young-onset Alzheimer’s disease. J Alzheimers Dis. 2020;77(3):1169–80.
Vijverberg EG, Dols A, Krudop WA, Del Campo MM, Kerssens CJ, Gossink F, et al. Cerebrospinal fluid biomarker examination as a tool to discriminate behavioral variant frontotemporal dementia from primary psychiatric disorders. Alzheimers Dement (Amst). 2017;7:99–106.
Percie du Sert N, Hurst V, Ahluwalia A, Alam S, Avey MT, Baker M, et al. The ARRIVE guidelines 2.0: Updated guidelines for reporting animal research. PLoS Biol. 2020;18(7):e3000410. https://doi.org/10.1371/journal.pbio.3000410.
Das S, Dewit N, Jacobs D, Pijnenburg YAL, In’t Veld SGJG, Coppens S, et al. A novel neurofilament light chain ELISA validated in patients with Alzheimer’s disease, frontotemporal dementia, and subjective cognitive decline, and the evaluation of candidate proteins for immunoassay calibration. Int J Mol Sci. 2022;23(13):7221.
Jacobs D, Delacourt J, Vanbrabant J, Dewit N, Galasko D, Vanmechelen E. A monoconal antibody based immunoassay for Neuronal Pentraxin2 in CSF. AnnuRevImmunol. 2017;6(2):337–66.
GómezdeSanJosé N, Goossens J, Al Shweiki MR, Halbgebauer S, Oeckl P, Steinacker P, et al. Glutamate receptor 4 as a fluid biomarker for the diagnosis of psychiatric disorders. J Psychiatr Res. 2022;156:390–7.
Faul F, Erdfelder E, Lang A-G, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–91.
Cervantes González A, Irwin DJ, Alcolea D, McMillan CT, Chen-Plotkin A, Wolk D, et al. Multimarker synaptic protein cerebrospinal fluid panels reflect TDP-43 pathology and cognitive performance in a pathological cohort of frontotemporal lobar degeneration. Mol Neurodegener. 2022;17(1):29.
Wellington H, Paterson RW, Portelius E, Törnqvist U, Magdalinou N, Fox NC, et al. Increased CSF neurogranin concentration is specific to Alzheimer disease. Neurology. 2016;86(9):829–35. https://doi.org/10.1212/WNL.0000000000002423.
Ratnavalli E, Brayne C, Dawson K, Hodges JR. The prevalence of frontotemporal dementia. Neurology. 2002;58(11):1615–21. https://doi.org/10.1212/wnl.58.11.1615.
Ducharme S, Dols A, Laforce R, Devenney E, Kumfor F, Van Den Stock J, et al. Recommendations to distinguish behavioural variant frontotemporal dementia from psychiatric disorders. Brain. 2020;143(6):1632–50.
Falgàs N, Ruiz-Peris M, Pérez-Millan A, Sala-Llonch R, Antonell A, Balasa M, et al. Contribution of CSF biomarkers to early-onset Alzheimer’s disease and frontotemporal dementia neuroimaging signatures. Hum Brain Mapp. 2020;41(8):2004–13.
Willemse EAJ, Sieben A, Somers C, Vermeiren Y, De Roeck N, Timmers M, et al. Neurogranin as biomarker in CSF is non-specific to Alzheimer’s disease dementia. Neurobiol Aging. 2021;108:99–109.
Acknowledgements
Clinical CSF samples were transferred from the Amsterdam Dementia Cohort Biobank located at the Amsterdam University Medical Centre, Amsterdam, The Netherlands, to the ADx Biobank located at ADx NeuroSciences, Gent, Belgium, following a contract established between the two involved parties (contract number BBI2021-002). The human whole-brain extracts and human synaptosome extracts were graciously provided by Dr. Alberto Lléo and Dr. Olivia Belbin from the Hospital de la Santa Creu I Sant Pau, Barcelona, Spain. The authors would like to thank Dr. Olivia Belbin and Charlotte De Rocker for their critical review of the manuscript.
Funding
The research discussed herein has received funding from the European Union’s Horizon 2020 research and innovation program under grant agreement number 860197. Part of the data used in this article has been collected as a part of the 18HLT09 NeuroMET2 project which received funding from the EMPIR program co-financed by the Participating States and from the European Union’s Horizon 2020 research and innovation program.
Author information
Authors and Affiliations
Contributions
S.D. performed analytical validations of the immunoassays, clinical sample measurements, data analysis, and figure preparation and wrote the first draft of the manuscript. J.G. contributed to the immunization strategies for the generation of novel antibodies; performed analytical validations of the immunoassays, clinical sample measurements, and data analysis; and reviewed and critiqued the manuscript. N.D. contributed to the immunization strategies for the generation of novel antibodies, performed analytical validations of the immunoassays and clinical sample measurements, and provided a review and critique of the manuscript. D.J. contributed to the immunization strategies for the generation of novel antibodies, performed analytical validations of the immunoassays, and provided a review and critique of the manuscript. Y.P., S.V., and C.T. provided the clinical samples and patient demographic data and reviewed and critiqued the manuscript. E.V.M. initiated the strategies for the generation of novel antibodies, contributed to the data analysis, and also reviewed and critiqued the manuscript. C.T. and E.V.M. have also been responsible for securing the project funding. All authors have approved the submission of this manuscript and consent to its publication.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All animal experiments were performed in accordance with the ARRIVE guidelines, following good laboratory practices and ethical regulations. All clinical CSF samples were procured as a part of the Amsterdam Dementia Cohort Biobank agreement.
Consent for publication
Not applicable.
Competing interests
S.D., J.G., and D.J. are employees of ADx NeuroSciences, Gent, Belgium. S.D. is also enrolled as a Ph.D. candidate at the Amsterdam University Medical Centre, Amsterdam, Netherlands. E.V.M. is the co-founder of ADx NeuroSciences. C.T. has a collaboration contract with ADx NeuroSciences, Quanterix, and Eli Lilly and has performed contract research or received grants from AC-Immune, Axon Neurosciences, Bioconnect, Bioorchestra, Brainstorm Therapeutics, Celgene, EIP Pharma, Eisai, Grifols, Novo Nordisk, PeopleBio, Roche, Toyama, and Vivoryon. She serves on editorial boards of Medidact Neurologie/Springer, Alzheimer Research and Therapy, Neurology: Neuroimmunology & Neuroinflammation, and is the editor of a Neuromethods book Springer. All the other authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Supplementary Tables. Supplementary Figures.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Das, S., Goossens, J., Jacobs, D. et al. Synaptic biomarkers in the cerebrospinal fluid associate differentially with classical neuronal biomarkers in patients with Alzheimer’s disease and frontotemporal dementia. Alz Res Therapy 15, 62 (2023). https://doi.org/10.1186/s13195-023-01212-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13195-023-01212-x