
Abstract
Background
High empathy levels in health professionals represent an important factor in patient satisfaction and compliance, reducing patient anxiety and pain, enhancing diagnostic and clinical results and strengthening patient empowerment. Our purpose was to determine empathy level and to identify which of the socioeconomic status (SES) and psychological factors were able to predict highest empathy levels in a Romanian sample of community nurses.
Methods
Community nurses were invited in January-February 2023 to provide an answer to an online survey, using an advertisement in a professional network. 1580 participants voluntarily agreed to take part in this study, with a response rate of 85.8%. The survey included the Toronto Empathy Questionnaire, the Reading the Mind in the Eyes Test and socio-economic status items. A multivariate model for the prediction of belonging to the highest quartile of empathy as opposed to lowest quartile was constructed using SES and psychological variables as factors.
Results
The mean (SD) empathy level was 49.1 (6.7), with 74.7% of participants over the threshold of high empathy level. In the multivariate analysis, predictors of belonging to the highest quartile of TEQ, as opposed to the lowest quartile were: low self-perceived stress level (OR = 2.098, 95%CI 1.362–3.231), higher experience as a community nurse (OR = 1.561, 95%CI 1.120–2.175) and higher levels of the theory of mind (OR = 1.158, 95%CI 1.118–1.199), when controlling for gender, age, relationship status, presence of children in families, education, and income.
Conclusions
Training programs targeting to increase emotional competences, reduce levels of stress and encourage personnel retention have the potential to increase the quality of community nursing in Romania.
Similar content being viewed by others


Background
Individual emotional characteristics are inborn, however emotional competences can be taught and trained in familial environments and in schools [1]. While practiced in social and cultural contexts, emotional skills have a positive impact on workplace performance, interpersonal relations, stress management and promotion of healthy lifestyles [2].
Empathy is an important part of our human interaction, allowing the connection with others, with positive effects both in professional and personal life. Empathy is a critical skill in the medical profession, especially in nurses, because it is the base of good communication with patients. In a systematic review [3], empathy of health professionals was found to be an important factor in patient satisfaction and compliance, reducing patient anxiety and pain, enhancing diagnostic and clinical results and strengthening patient empowerment.
It has been reported that health professionals can be psychologically affected by dehumanization. Dehumanization was associated with several factors such emotional exhaustion and stress, as well as to work related factors such as staff ratios and patient care automation. The effect of dehumanization on health professionals is determining them to practice medicine mechanically, with moral disengagement and without empathy [2, 4, 5] .
It is considered that adequate empathic social behavior is due to the perfect balance between mentalizing, involving cognitive and affective theory of mind and simulation processing, represented by emotional empathy. Since these emotional experiences are mediated by different neural networks: amygdala and insula for emotional experiences and ventromedial prefrontal cortex for the theory of mind, it has been proposed that empathy and the theory of mind are multidimensional [6].
Since aspects of empathy have not been measured in a Romanian national representative sample of community nurses so far, our research hypothesis was to determine empathy level and to identify which of the socioeconomic status (SES) and psychological factors were able to predict highest levels of empathy in this cohort.
Methods
Participants
Community nurses provide medical and nursing care to patients outside of traditional hospital settings. In Romania, their aim is to increase the access of the population and, in particular, of vulnerable groups to quality medico-social services. Their job includes preventive, curative, and recovery medical services, including case management in complex cases of chronic diseases and rare diseases. Of 1840 community nurses employed in Romania in January—February 2023, 1580 participants agreed to take part in this study, with a response rate of 85.8%.
Procedure
The sample was recruited by an advertisement in a professional network in January—February 2023. The project was shortly advertised on a national work platform for community nurses from Romania to participate in a research project. The questionnaire was set online on the Google Forms platform and the link to the questionnaire was provided in the advertisement. The first page of the questionnaire included the purpose of the study, the estimated completion time, and some information on the instrument used and the result of the questionnaire. The agreement to participate was included in this introductory page and only those who gave their consent were allowed to access the questionnaire. All questions were required and participants who provided answers to all questions were allowed to submit the form. As retribution for their involvement, at the moment of questionnaire completion, the participants received a report describing their perception of emotions ability. The Research Ethics Committee of Victor Babes University of Medicine and Pharmacy approved the study protocol (no Nr. 30/31.03.2022). Participants voluntarily agreed to participate and gave informed consent. The study was conducted in accordance with the Helsinki declaration.
Materials
Toronto Empathy Questionnaire (TEQ)
TEQ was developed by Spreng et al. [7] and is a self-report questionnaire measuring a person’s emotional ability to understand and respond to others. This test includes 16 questions, half of which are positively worded (items 1, 3, 5, 6, 8, 9, 13, 16) and the other half are negatively worded (items 2, 4, 7, 10, 11, 12, 14, 15). For each item, answers must be chosen from the following options: Never; Rarely; Sometimes; Often; Always. Positive items are scored Never = 0; Rarely = 1; Sometimes = 2; Often = 3; Always = 4 and negative items are scored Never = 4; Rarely = 3; Sometimes = 2; Often = 1; Always = 0. Total TEQ score was obtained by adding the individual item scores. For this study, the validated Romanian version [8] of TEQ was used. The score ranges from 0 to 64. Individuals scoring 45 or higher are considered with high levels of empathy.
The ‘reading the mind in the eyes’ test (RMET)
This test includes 36 black and white photographs of actors, taken from movies, of male and female eyes depicting different emotional states. Participants are asked to choose the best description of four possible emotions that fits the eyes’ emotions. For this test, the performance of the participants was calculated as the total points of correct answers of 36 images. We used the Romanian version of the Reading the Mind in the Eyes Test [9].
SES related questions
Besides the questionnaires described above, the survey also included questions about gender, age, relationship status, presence of children in family, school (3 levels, equivalent to ISCED3 or 4, ISCED 5 or 6, ISCED 7 or 8), income (5 levels), years of experience as a community nurse and self-perceived stress levels. Stress levels were quantified on a 10 points scale, with higher levels indicating higher levels of stress.
Data management and statistics
The questionnaire was set online using the Google Forms platform and the invitees were provided a link to the questionnaire. The first section of the questionnaire included a presentation of the survey and a consent form. IBM SPSS version 21 was used to perform data transformations and statistics. Kolmogorov-Smirnoff test was used to test normal distribution, and the main outcome variables (scores of TEQ and RMET) were all normally distributed. Continuous variables are presented as mean and standard deviation (SD). The categorical variables are presented as absolute and relative frequencies. A p-value < 0.05 was considered statistically significant. To compare means, the t-test and ANOVA were used. SES and psychological characteristics of community nurses were used to predict belonging to the highest quartile, as compared to the lowest quartile of the TEQ score, in a regression analysis model.
Results
The demographic characteristics of the study population are presented in Table 1. Women represented 93.9% (1483) and the mean (SD) age of the group was 42.8 (8.2) years with a range from 22 to 65. Most of the responders, 85.3% (1347) are in a relationship and 86.3% (1364) have at least one child, while 21.7% (343) of them reported having at least a university degree—The International Standard Classification of Education (ISCED 5). On the experience as a community nurse, 46.1% (511) have experience of 5 years or less and more than half of all 58.2% (920) declare income below 3000 lei (equivalent to 611 euro, the minimum income level in January 2023 in Romania). 13.4% (211) have quantified their stress level as 7 points or more out of a scale of 10, qualifying as high levels of stress. For RMET, the mean score was 22.1 (4.7).
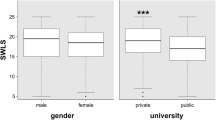
The mean scores for TEQ by SES factors are presented in Table 2. For TEQ, the mean score was 49.1 (6.7). The score was significantly higher 49.5 (6.6) for community nurses with more than 6 years of experience, as compared to those with 6 years or less 48.6 (6.8). No significant difference was found for the other SES factors tested: gender, relationship status, presence of children, education, income and age categories. Also, TEQ levels were significantly higher in participants reporting low levels of stress 49.5 (6.4), as compared with those reporting high levels of stress 46.1 (7.7). Per tertiles of RMET score, a significant positive trend is observed, and correlation between RMET score and TEQ score r = 0.282, p < 0.001, sharing 8% of variance.
Using only participants from the lowest and highest quartile of TEQ scores, we created a prediction model using SES and psychological variables. The OR and the 95% confidence intervals of the OR of each predictor fitted into the model are presented in Table 3. Highest OR (2.098, 95%CI 1.362–3.231) to pertain to the top quartile of TEQ was achieved by the low levels of stress. Higher experience as a community nurse had the OR = 1.561, 95%CI 1.120–2.175. RMET score contributed to the model with an OR = 1.158, 95%CI 1.118–1.199. The other social demographic factors did not significantly contribute to the model, yet are accounted for in the model.
Dependent variable: highest vs. lowest quartile of TEQ; Independent variables: gender (2 categories), Age (years), Relationship status (2 categories), Children (2 categories), education (2 categories), experience (2 categories), income (2 categories), Self-perceived stress levels (2 categories), RMET score (discrete units of score).
Discussion
The nurse-patient relationship is modulated by emotional competences. To be empathetic to patients and to have the capacity to read emotions is a fundamental aspect of care. These capacities can be regulated by other emotional abilities as well as technical skills in order to acknowledge the patient’s needs and offer therapeutically appropriate response [10]. To the best of our knowledge, empathy was not studied in a Romania national sample of community nurses. Our study improves the understanding of the emotional competences of this professional group.
As required by roles played by these professionals, the mean levels of empathy are increased, with 74.7% of the sample being over the threshold of high empathy level (scoring > = 45), while the mean (SD) reported score was 49.1 (6.7). A recent study investigating the empathy among senior medical students from Romania has found a similar mean (SD) level of empathy of 48.76 (5.65) [8]. Using the same instrument, when studying nurses that work in psychiatric wards, Alhadidi et al. [11] have identified lower levels of empathy, reporting a mean (SD) of 46.07 (6.7). Conversely, Cosper [12] found similar levels of empathy 49.8 (4.3) in nurses working in the Intensive Care Unit (ICU).
Our results indicate that as experience as a community nurse accumulates, the empathy level increases: nurses with more than 6 years of experience had 56% more chances to be in the higher quartile of empathy, suggesting that job or field retention is a key factor for increased empathy. Observing the tertiles of years of experience, the empathy level increases steadily. A publication on the 10 year trend of empathy in intensive care units from China [21]. In medical students, several studies have discovered a decline in empathy at the beginning of the clinical phase of medical education [18, 22, 23]. Several studies looked into the reasons for this decline and found that its co** mechanism for distress [24] and was caused by school related factors such as lack of time, physical and psychological fatigue, competitiveness, performance demands, cramming, stress, high workload [25, 26], some of these factors belonging to the hidden curriculum to become a medical professional [27].
Possible explanations on the differences between our study and studies on nurses working in high demanding positions like in ICU, oncology or psychiatry or while in training, lie in the job description of community nurses, which are engaged in a diverse and challenging health landscape, providing care is different settings from patient’s own houses, nursing homes, family doctor practices, or other types of clinics.
High levels of self-perceived stress are a good predictor of low levels of empathy, both in univariate and multivariate models. Others have also reported negative associations between stress/anxiety and empathy, with stress/anxiety management having a positive effect on empathy levels [2, 28, 29]. Extensive prior research [30] has shown how anxiety reduces empathy, suggesting that experiencing emotions associated with uncertainty, increases egocentric perspectives when perceiving the mental states of others.
Cognitive empathy—the capacity to understand other people by ascertaining their mental state, also known as the theory of mind, quantified in our study by the RMET, shows a positive association with the TEQ score, sharing 8% of variance. In the multivariate model, by each one point increase in the RMET score, the chances to be in the high quartile of TEQ as opposed to the low quartile grow by 16.5%. In a recent study [2] on nurses, cognitive empathy was a mediator between emotional intelligence and humanization of care, with 18% shared variance between cognitive empathy and humanization of care. In another study [31], performed in general population, using a prediction model for the RMET score by components of the emotional intelligence, have found that the highest contributor is the understanding subscale (β = 0.28, p < 0.001), followed by perceiving (β = 0.09, p < 0.01), and managing subscales (β = 0.08, p < 0.05). The variance shared between emotional and cognitive intelligence was 8.4%, similar to our results. Using subgroup analysis from the general population, Baron-Cohen et al. [32] have found lower shared variance, at about 2%, between cognitive empathy and empathy quotient.
Our study did not find significant differences in empathy levels between genders in this population, similar to several studies on nursing students [13] or psychiatric ward nurses [11] or ICU nurses [12]. Also, education level, familial background and income levels did not influence the empathy level in our sample. Others have found that empathy was higher in nurses with higher education, albeit those nurses were working in ICU [33] or were students with a previous degree before enrolling in studying nursing [34]. Studies performed to capture empathy in family dynamics have shown that positive family environments are positively related to empathy levels in adolescents [35]. In a longitudinal study [36], high compassion for others in adulthood predicted, after a 10-year follow-up, higher adulthood social-economic status, although not vice versa.
Considering that high levels of empathy are critically needed for nursing, it is important to acknowledge that empathy can be learned and taught. Making a review of European training programs for emotional competencies in vocational training, Sauli et al. [1] have found four types of training available in Europe, however they lacked a rigorous scientific approach, proposing a set of guidelines for program development. Using an educational program designed by patient and family advisers, Cosper [12] demonstrated an increase in empathy levels of nurses, higher in those younger than 30 years, as compared to their counterparts. Thus recognizing the benefit of early career educational programs.
Two of the strengths of this study are the large number of participants and the high response rate of 85.8%, leading to the assessment of a representative national sample of community nurses from Romania. Looking into the response rate of different organizational research based on questionnaires, Baruch et al. [37] found that the response rate in public/state sector varied from a minimum of 27.0% to a maximum of 82.8% with a mean (SD) of 54.5 (16.7) and in Health care from a minimum of 17.4% to a maximum of 94.0% with a mean (SD) of 53.8 (20.0). By comparison, our results sit in the highest quartile. If this high response rate, which was obtained without reminders is used as a proxy for empathy, the result is concordant to high scores in TEQ, where 74.7% of responders had a high empathy score. If we would use this proxy, it might be that the non-responders would have lower empathy levels, inducing a selection bias, because people interested in participation usually have a genuine interest in the subject of the research.
Conclusion
The analysis of empathy in a large sample of Romanian community nurses showed good levels of empathy, since almost three quarters of them scored high empathy levels. The capacity of reading emotions (theory of mind abilities) and higher experience, along with low levels of stress, led to higher levels of empathy. Future early-career training programs targeting to increase emotional competences, reduce levels of stress and encourage personnel retention could promote increased quality of community nursing in Romania.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Sauli F, Wenger M, Fiori M. Emotional competences in vocational education and training: state of the art and guidelines for interventions. Empir Res Vocat Educ Train. 2022;14(1):4.
Pérez-Fuentes MDC, Herrera-Peco I, Molero Jurado MDM, Oropesa Ruiz NF, Ayuso-Murillo D, Gázquez Linares JJ. A cross-sectional study of Empathy and emotion management: key to a work environment for Humanized Care in nursing. Front Psychol. 2020;11:706. https://doi.org/10.3389/fpsyg.2020.00706. PMID: 32477202; PMCID: PMC7237745.
Derksen F, Bensing J, Lagro-Janssen A. Effectiveness of empathy in general practice: a systematic review. Br J Gen Pract. 2013;63(606):e76–84.
Haque OS, Waytz A. Dehumanization in Medicine: causes, solutions, and functions. Perspect Psychol Sci. 2012;7(2):176–86.
Głębocka A. Stress and Dehumanizing Behaviors of Medical Staff Toward Patients. In: Pokorski M, editor. Advances in Medicine and Medical Research [Internet]. Cham: Springer International Publishing; 2019 [cited 2023 Feb 24]. p. 97–104. (Advances in Experimental Medicine and Biology). https://doi.org/10.1007/5584_2018_308.
Dvash J, Shamay-Tsoory SG. Theory of mind and empathy as multidimensional constructs: neurological foundations. Top Lang Disord. 2014;34:282–95.
Spreng RN, McKinnon MC, Mar RA, Levine B. The Toronto Empathy Questionnaire: scale development and initial validation of a factor-analytic solution to multiple empathy measures. J Pers Assess. 2009;91(1):62–71. PMID: 19085285; PMCID: PMC2775495.
Ursoniu S, Serban CL, Giurgi-Oncu C, Rivis IA, Bucur A, Bredicean AC et al. Validation of the Romanian Version of the Toronto Empathy Questionnaire (TEQ) among Undergraduate Medical Students. Int J Environ Res Public Health. 2021;18(24).
Eyes Test (Adult).—Autism Research Centre [Internet]. Accessed 2023 Feb 11. Available from: https://www.autismresearchcentre.com/tests/eyes-test-adult/.
Brunero S, Cowan D, Chaniang S, Lamont S. Empathy education in post-graduate nurses: an integrative review. Nurse Educ Today. 2022;112:105338.
Alhadidi MMB, Abdalrahim MS, Al-Hussami M. Nurses’ caring and empathy in Jordanian psychiatric hospitals: a national survey. Int J Ment Health Nurs. 2016;25(4):337–45.
Cosper P, Kaplow R, Moss J. The impact of patient and family advisors on critical care nurses’ Empathy. JONA J Nurs Adm. 2018;48(12):622.
Yi X, Sicheng X, Lihui Z, Jianhui X, Zhenhui S, **ang D, et al. Changes in empathy of nurses from 2009 to 2018: a cross-temporal meta-analysis. Nurs Ethics. 2021;28(5):776–90.
Reid-Ponte P. Distress in cancer patients and primary nurses’ empathy skills. Cancer Nurs. 1992;15(4):283.
Ward J, Cody J, Schaal M, Hojat M. The Empathy Enigma: an empirical study of decline in Empathy among undergraduate nursing students. J Prof Nurs. 2012;28(1):34–40.
Sedaghati Kesbakhi M, Rohani C. Changes in the level of nursing students’ Empathy during Four Years Education. J Med Educ. 2020;19(2).
Coulmas MC. A study of the effect of clinical experience on nursing empathy (Doctoral dissertation, Capella University). Available from: https://www.proquest.com/openview/bed867ce8e8223ebcfa298586917190a/1?pq-origsite=gscholar&cbl=18750&diss=y Accessed 2023 Feb 23.
Hojat M, Vergare MJ, Maxwell K, Brainard G, Herrine SK, Isenberg GA, et al. The devil is in the third year: a longitudinal study of erosion of empathy in medical school. Acad Med J Assoc Am Med Coll. 2009;84(9):1182–91.
Hunsaker S, Chen HC, Maughan D, Heaston S. Factors that influence the development of compassion fatigue, burnout, and compassion satisfaction in emergency department nurses. J Nurs Scholarsh off Publ Sigma Theta Tau Int Honor Soc Nurs. 2015;47(2):186–94.
Håkansson Eklund J, Holmström IK, Ollén Lindqvist A, Sundler AJ, Hochwälder J. Marmstål Hammar L. Empathy levels among nursing students: a comparative cross-sectional study. Nurs Open. 2019;6(3):983–9.
Samra R. Empathy and Burnout in Medicine—Acknowledging risks and opportunities. J Gen Intern Med. 2018;33(7):991–3.
Chen D, Lew R, Hershman W, Orlander J. A cross-sectional measurement of medical student empathy. J Gen Intern Med. 2007;22(10):1434–8. https://doi.org/10.1007/s11606-007-0298-x.
Hojat M, Shannon SC, DeSantis J, Speicher MR, Bragan L, Calabrese LH. Does Empathy decline in the clinical phase of Medical Education? A Nationwide, Multi-Institutional, cross-sectional study of students at DO-Granting medical schools. Acad Med. 2020;95(6):911.
Neumann M, Edelhäuser F, Tauschel D, Fischer MR, Wirtz M, Woopen C, et al. Empathy decline and its reasons: a systematic review of studies with Medical students and residents. Acad Med. 2011;86(8):996.
Brodahl KØ, Storøy HLE, Finset A, Pedersen R. Medical students’ experiences when empathizing with patients’ emotional issues during a medical interview – a qualitative study. BMC Med Educ. 2022;22(1):145.
Costa-Drolon E, Verneuil L, Manolios E, Revah-Levy A, Sibeoni J. Medical students’ perspectives on Empathy: a systematic review and Metasynthesis. Acad Med. 2021;96(1):142.
Eikeland HL, Ørnes K, Finset A, Pedersen R. The physician’s role and empathy – a qualitative study of third year medical students. BMC Med Educ. 2014;14(1):165.
Molero Jurado M, del M, Pérez-Fuentes M, del Oropesa Ruiz C. Simón Márquez M Del M, Gázquez Linares JJ. Self-efficacy and Emotional Intelligence as predictors of Perceived stress in nursing professionals. Med (Mex). 2019;55(6):237.
Ayuso-Murillo D, Colomer-Sánchez A, Santiago-Magdalena CR, Lendínez-Mesa A, De Benítez E, López-Peláez A, et al. Effect of anxiety on Empathy: an observational study among nurses. Healthcare. 2020;8(2):140.
Todd AR, Forstmann M, Burgmer P, Brooks AW, Galinsky AD. Anxious and egocentric: how specific emotions influence perspective taking. J Exp Psychol Gen. 2015;144(2):374–91.
Megías-Robles A, Gutiérrez-Cobo MJ, Cabello R, Gómez-Leal R, Baron-Cohen S, Fernández-Berrocal P. The ‘Reading the mind in the eyes’ test and emotional intelligence. R Soc Open Sci. 2020;7(9):201305.
Baron-Cohen S, Bowen DC, Holt RJ, Allison C, Auyeung B, Lombardo MV, et al. The reading the mind in the eyes test: complete absence of typical sex difference in ~ 400 men and women with autism. PLoS ONE. 2015;10(8):e0136521.
Watt-Watson J, Garfinkel P, Gallop R, Stevens B, Streiner D. The impact of nurses’ empathic responses on patients’ Pain Management in Acute Care. Nurs Res. 2000;49(4):191.
Ward J, Schaal M, Sullivan J, Bowen ME, Erdmann JB, Hojat M. Reliability and validity of the Jefferson Scale of Empathy in undergraduate nursing students. J Nurs Meas. 2009;17(1):73–88.
Silke C, Brady B, Boylan C, Dolan P. Factors influencing the development of empathy and pro-social behaviour among adolescents: a systematic review. Child Youth Serv Rev. 2018;94:421–36.
Saarinen AI, Keltner D, Dobewall H, Lehtimäki T, Keltikangas-Järvinen L, Hintsanen M. The relationship of socioeconomic status in childhood and adulthood with compassion: a study with a prospective 32-year follow-up. PLoS ONE. 2021;16(3):e0248226.
Baruch Y, Holtom BC. Survey response rate levels and trends in organizational research. Hum Relat. 2008;1(8):1139–60. https://doi.org/10.1177/0018726708094863.
Acknowledgements
This work was generated within the project “Expansion of medical and community services for people affected by genetic and rare diseases, acronym MEDI.COM-RARE”, Contract no. AR 19076/26.10.2022, Funded within the Iceland, Liechtenstein and Norway grants.
This work has been generated within The European Reference Network on Rare Congenital Malformations and Rare Intellectual Disability (ERN-ITHACA) [EU Framework Partnership Agreement ID: 3HP-HP-FPA ERN-01-2016/739516].
Funding
None.
Author information
Authors and Affiliations
Contributions
LO, CLS, ACE, MP designed the study. LO and RMJ recruited the participants. LO, RMJ and MP designed the online collection tool. RMJ exported the database and performed initial quality checks. CLS and ACE performed data management and statistical analysis. LO and CLS drafted the manuscript. ACE and MP critically reviewed the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Research Ethics Committee of Victor Babes University of Medicine and Pharmacy approved the study protocol (no Nr. 30/31.03.2022). Participants voluntarily agreed to participate and gave informed consent. The study was conducted in accordance with the Helsinki declaration.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Onofrei, L., Serban, C.L., Chirita-Emandi, A. et al. The impact of theory of mind, stress and professional experience on empathy in Romanian community nurses—a cross-sectional study. BMC Nurs 22, 400 (2023). https://doi.org/10.1186/s12912-023-01569-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12912-023-01569-2