
Abstract
Background
Cardiac involvement in patients with immunoglubin light-chain amyloidosis (AL) is a major determinant of treatment choice and prognosis, and early identification of high-risk patients can initiate intensive treatment strategies to achieve better survival. This study aimed to investigate the prognostic value of native T1 and ECV in patients with AL-cardiac amyloidosis (CA).
Methods
A total of 38 patients (mean age 59 ± 11 years) with AL diagnosed histopathologically from July 2017 to October 2021 were collected consecutively. All patients were performed 3.0-T cardiac magnetic resonance (CMR) including cine, T1 map**, and late gadolinium enhancement (LGE). Pre- and post-contrast T1 map** images were transferred to a dedicated research software package (CVI42 v5.11.3) to create parametric T1 and ECV values. In addition, clinical and laboratory data of all patients were collected, and patients or their family members were regularly followed up by telephone every 3 months. The starting point of follow-up was the time of definitive pathological diagnosis, and the main endpoint was all-cause death. Kaplan-Meier analysis and Cox proportional risk model were used to evaluate the association between native T1 and ECV and death in patients with CA.
Results
After a median follow-up of 27 (16, 37) months, 12 patients with CA died. Kaplan-Meier analysis showed that elevated native T1 and ECV were closely associated with poor prognosis in patients with CA. The survival rate of patients with ECV > 44% and native T1 > 1389ms were significantly lower than that of patients with ECV ≤ 44% and native T1 ≤ 1389ms (Log-rank P < 0.001), and was not associated with the presence of LGE. After adjusting for clinical risk factors and CMR measurements in a stepwise multivariate Cox regression model, ECV [risk ratio (HR):1.37, 95%CI: 1.09–1.73, P = 0.008] and native T1 (HR:1.01, 95%CI: 1.00-1.02, P = 0.037) remained independent predictors of all-cause mortality in patients with CA.
Conclusions
Both native T1 and ECV were independently prognostic for mortality in patients with CA, and can be used as important indicators for clinical prognosis assessment of AL.
Similar content being viewed by others


Introduction
Immunoglobulin light-chain amyloidosis (AL) is the most common systemic amyloidosis results from the deposition of protein derived from fragments of clonal immunoglobulin light chain by abnormally functioning plasma cells. Cardiac involvement is described in up to 70% of AL patients during the course of the disease. Previous studies have shown that cardiac damage is the most important determinant of prognosis in AL patients [1, 2]. In these patients, aggressive chemotherapy and autologous stem cell transplantation (ASCT) can significantly improve the clinical prognosis [3, 4]. Therefore, early recognition of cardiac amyloidosis (CA) may potentially alter prognosis by prompting early aggressive treatment.
In current clinical practice, endomyocardial biopsy (EMB) is considered as the “gold standard” for the diagnosis of cardiac amyloidosis, however, the invasive methodology and complicate sampling processing and assessment are the major disadvantages for EMB [5]. Moreover, some non-invasive techniques, such as cardiac biomarkers, electrocardiograph (ECG), and echocardiography can assist physicians with the diagnosis of CA. In previous study, echocardiography was frequently used to diagnostic and prognosticate CA [2, 6], but coexisting causes of left ventricular hypertrophy may affect explanation. Low limb lead voltages, or fragmented QRS complexes on the ECG was also can be used to predict CA [7, 8], but was puzzled by conduction abnormalities and pericardial effusions. Nevertheless, current prognostic predictors of CA rely on surrogate measurements rather than direct markers of interstitial expansion.
In recent years, cardiac magnetic resonance examination (CMR) has emerged as a non-invasive technique for CA diagnosis, because it can provide unique information about tissue composition with late gadolinium enhancement (LGE), which shows a typical pattern of diffuse subendocardial or transmural enhancement rarely seen in other cardiomyopathies [9]. Moreover, Native T1 representing the intrinsic signal of the myocardium and myocardial extracellular volume (ECV) can quantitatively measure the progression of cardiac amyloid infiltration from early infiltration to diffuse transmural involvement [10, 11]. As our previous study has reported [12], native T1 and ECV have good diagnostic accuracy in the diagnosis of CA, especially could detect early disease, and have been shown to correlate with disease burden. Here, the aim of this study was to investigate the prognostic value of native T1 and ECV in patients with AL-cardiac amyloidosis.
Methods
Participants
38 AL patients were consecutively recruited from Department of Radiology, the First Affiliated Hospital of Soochow University from July 2017 to October 2021. All these patients were confirmed with systemic AL by Congo red and immunohistochemical staining using specimens of subcutaneous abdominal fat (n = 20), bone marrow (n = 10), kidney (n = 7), and upper gastrointestinal tract (n = 1). The diagnostic criteria for cardiac involvement in AL patients [13]: echocardiography showed a ventricular septal thickness of > 12 mm (without other causes) or NT-proBNP > 332ng/L (without renal insufficiency).
Clinical data
Clinical and laboratory data were collected from all patients, including: gender, age, clinical symptoms and signs, organs involved, ECG manifestations, cardiac biomarkers (NT-proBNP and Troponin T), serum free light chain (sFLC), the difference between involved and uninvolved sFLC (dFLC), Mayo stage and treatment methods, etc. A blood sample was obtained from all these subjects for biochemical examination and hematocrit at about 30 min before the CMR scan. The study was approved by the Ethics Committee of the First Affiliated Hospital of Soochow University (No: 2,019,112) and written informed consent was obtained from all participants.
CMR protocol
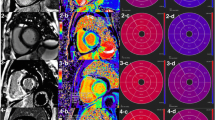
All participants underwent a standard CMR examination with a 3.0-T clinical scanner (Magnetom Skyra, Siemens AG, Healthcare Sector, Erlangen, Germany). A balance steady-state free precession (SSFP) sequence was used to obtain cine images, including multiple slice short-axis images, 2-chamber and 4-chamber long-axis images. The cine image parameters were as follows: repetition time (TR) 39.2 ms, echo time (TE) 1.4 ms, slice thickness 8 mm, field of view (FOV) 174 × 208 mm, matrix 256 × 256. LGE images was performed 10 min after a cumulative dose of 0.1 mmol/kg of gadolinium-based contrast agent (Magnevist, Bayer Healthcare, Berlin, Germany), using the phase-sensitive inversion recovery (PSIR) sequence for acquirement of the same multiple short-axis and long-axis images as cine images. Parameters for LGE images were TR 700 ms, TE 1.5ms, slice thickness 8 mm, flip angle 20º, FOV 256 × 192 mm, matrix 256 × 256, inversion time 300 ms. Native and post-contrast T1 map** images, including basal, mid-ventricular and apical short-axis images were acquired using the shortened modified look-locker inversion recovery sequence (shMOLLI) before and 15 min after administration of contrast agent. Parameters for T1 map** study were TR 277.9 ms, TE 1.1 ms, slice thickness 8 mm, flip angle 35 º, FOV 256 × 192 mm, matrix 192 × 144.
CMR image analysis
The cine images were transferred to a dedicated research software (CVI42 v5.11.3, Circle Cardiovascular Imaging, Alberta, Canada) to calculate left ventricular ejection fraction (LVEF), left ventricular end-diastolic volume index (LVEDVi), left ventricular end-systolic volume index (LVESVi), left ventricular myocardial mass index (LVMI), left ventricular output per wave (LVSV) and cardiac output (CO). Pre- and post-contrast shMOLLI sequence generated images with varying inversion times were transferred to software to create parametric T1 and ECV pixel maps and corresponding values. The LGE images were visually analyzed for the presence or absence of enhancement.
Follow-up and outcome
The primary outcome for this study was all-cause mortality. Follow-up information was obtained by telephone interviews of the patient or his or her family every 3 months. Patients were followed up until 31 October 2021, or censored if they were alive.
Statistical analysis
SPSS Statistics Version.22.0 (IBM, Chicago, IL, USA) was used for statistical analysis. Continuous data were expressed as mean ± SD or median and interquartile range according to whether normal distribution or not. Categorical data were expressed as frequencies and percentages. The independent sample t-test or non-parametric Mann-Whitney U test was used to compare the measurement data according to whether they were in accordance with normal distribution. Group count data were analyzed by χ2 test or exact probability method. Kaplan-Meier method was used for survival analysis, and log-rank was used to compare the differences between groups. Cox proportional hazard model was used for univariate and multivariate analysis. Statistical significance was defined as P < 0.05.
Results
Clinical and biochemical markers
The mean age of 38 patients was 59 years (range, 29–78 years), 74% were men. The clinical manifestations, underlying diseases, other organ involvement and ECG findings are shown in Table 1. In this study, according to 2012 clinical staging standard of Mayo Clinic [14], there were 8 (21%), 11 (29%), 10 (26%) and 9 (24%) patients in Mayo stage I, II, III and IV, respectively. Among them, 23 patients received chemotherapy or ASCT, and the remaining 15 patients received expectant treatment (Table 2).
CMR structural and functional parameters
According to the median ECV (44%) as the critical reference value, patients with CA were divided into ECV ≤ 44% group and ECV > 44% group. As shown in Table 2, NT-proBNP, Troponin T, dFLC, native T1 and LVMI in ECV > 44% group were higher than those in ECV ≤ 44% group, while LVEF and LVSV were lower than ECV ≤ 44% group (P < 0.05).
Survival analysis
After a median follow-up of 27 (16, 37) months, 12 patients with CA died. Kaplan-Meier survival curves demonstrated that the survival time of ECV > 44% group was shorter than that of ECV ≤ 44% group (median survival time, 10 months vs. 22 months, P < 0.001) (Fig. 1). According to the median native T1 (1389ms) as the critical reference value, patients were divided into native T1 > 1389ms group and native T1 ≤ 1389ms group. As shown in Fig. 2, the survival time of native T1 > 1389ms group was shorter than that of native T1 ≤ 1389ms group (median survival time, 10.5 months vs. 26.5 months, P < 0.001). However, Kaplan-Meier survival curves showed that there was no significant difference in the survival time of patients between LGE-positive group and LGE-negative group (P = 0.139) (Fig. 3).

Kaplan-Meier survival curves for patients with ECV > 44% and ECV ≤ 44%

Kaplan-Meier survival curves for patients with native T1 > 1389ms and native T1 ≤ 1389ms

Kaplan-Meier survival curves for patients with LGE-positive and LGE-negative
In the univariate Cox regression analysis (Table 3), NT-ProBNP, Troponin T, Mayo stage III to IV, native T1, ECV and LVMI were demonstrated as univariate predictors. After adjusting for clinical risk factors and CMR measurements in a stepwise multivariate Cox regression model, only ECV [Hazard ratio (HR): 1.37, 95%CI: 1.09–1.73, P = 0.008] and native T1 (HR: 1.01, 95%CI: 1.00-1.02, P = 0.037) were independent predictors for the primary endpoint (Table 3).
Discussion
Cardiac involvement is the main determinant of treatment choice and prognosis in patients with AL. Early identification of high-risk patients can begin to strengthen treatment strategies to achieve a better survival rate [15, 16]. Cardiac serum biomarkers NT-proBNP and troponin T are commonly used to evaluate the prognosis of patients with CA. Palladini G et al. [17] reported that NT-proBNP was a sensitive marker for cardiac involvement and a prognostic marker for patients with AL. Dispenzieri A et al. [18] found that the increase of troponin T level in patients with CA was related to low survival rate. Mayo clinic staging based on these biomarkers has become an important clinical tool for risk stratification of AL patients [14, 19]. In this study, in the univariate Cox proportional hazard model, NT-ProBNP (HR = 1.00, 95%CI: 1.00–1.00, P < 0.001), troponin T (HR = 1.02, 95%CI: 1.00-1.04, P = 0.032) and Mayo stage III to IV (HR = 7.26, 95%CI: 1.59–33.27, P = 0.011) were risk factors affecting the survival of patients with CA.
In recent years, noninvasive imaging based on cardiac morphology and function has attracted extensive attention in the prognostic assessment of CA [9, 10, 20, 21]. CMR-LGE is not only a diagnostic marker for patients with CA, but also a powerful predictor of mortality [4, 22, 23]. Fontana M et al. [24] reported that patients with CA without LGE had the best prognosis, while those with diffuse transmural LGE had the worst prognosis. In our previous study, we found that nativeT1 and ECV were more sensitive than LGE in the early diagnosis of CA, and the degree of amyloid infiltration in the myocardium could be indirectly reflected by nativeT1 and ECV [12]. In this study, we used nativeT1 and ECV to evaluate the prognostic of patients with CA. The results showed that the increase of nativeT1 and ECV were closely related to the poor prognosis of patients. The survival rate of patients in ECV > 44% group and native T1 > 1389ms group were significantly lower than that in ECV ≤ 44% group and native T1 ≤ 1389ms group, and it was not related to the presence of LGE. In the stepwise multivariable Cox regression model, after adjusting for age, gender, cardiac biomarkers, Mayo stage, and LGE, ECV and native T1 were independent predictors of all-cause mortality in patients with CA. Banypersad SM et al. [21] found that the increase of native T1 and ECV were associated with cardiac biomarkers and poor prognosis, and ECV > 45% was associated with decreased survival in patients with AL. Agha AM et al. [25] reported that ECV ≥ 50% was associated with increased mortality in patients with CA. In this study, ECV > 44% is related to the decreased survival rate in patients with CA, which is basically consistent with previous studies. Lin L et al. [26] demonstrated that compared with other clinical and imaging parameters, ECV ≥ 44% and LGE could independently predict the mortality in patients with CA, and in subgroups with the same LGE pattern, ECV ≥ 44% could still predict prognosis, while native T1 could not predict mortality. However, our results showed that LGE was not a predictor of death in patients with CA, and there was no significant difference in survival time between LGE-positive and LGE-negative patients, while native T1 could independently predict mortality in patients with CA.
Native T1 can be affected by different research institutions, machine types, magnetic field intensity, pulse sequence and other factors [27,28,29], however, ECV is based on the ratio of myocardial T1 value before and after enhancement, which can correct the influence of various technical factors mentioned above. Therefore, ECV is a relatively stable reference indicators. However, the kidney is also one of the most common organs involved in AL patients [30, 31], and renal insufficiency is a contraindication for the use of contrast media, which will limit the use of ECV in this population. Native T1 is the myocardial T1 value measured without contrast medium, therefore, it can be used as a supplementary means of ECV to evaluate the prognosis of patients with renal insufficiency.
However, this study has some limitations. Firstly, this study is a single-center study, which limits the generality of the results and increases the possibility of selection bias. Secondly, the study has a small sample size and a low incidence of end-point events, the sample size needs to be further expanded to verify the results of the study. Thirdly, the number of patients in the LGE-positive group (76%) is much higher than that in the LGE-negative group, which may bias our results. Finally, only all-cause mortality was used to observe end events.
Conclusion
This study supports the importance of CMR in addition to cardiac biomarkers in predicting outcomes among patients at risk of having AL CA. Our results demonstrate that native T1 and ECV are independent predictors of mortality in patients with CA, and native T1 can be used to predict the prognosis of patients with renal insufficiency.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Lee MH, Lee SP, Kim YJ, et al. Diagnosis and prognosis of cardiac amyloidosis. Korean Circ J. 2013;43(11):752.
Bellavia D, Pellikka PA, Al-Zahrani GB, et al. Independent predictors of survival in primary systemic (AL) amyloidosis, including cardiac biomarkers and left ventricular strain imaging: an observational cohort Study. J Am Soc Echocardiogr. 2010;23(6):643–52.
Adam RD, Coriu D, Jercan A, et al. Progress and challenges in the treatment of cardiac amyloidosis: a review of the literature. ESC Heart Fail. 2021;8(4):2380–96.
Patel RK, Fontana M, Ruberg FL. Cardiac amyloidosis: multimodal imaging of disease activity and response to treatment. Circ Cardiovasc Imaging. 2021;14(6):e009025.
Cooper LT, Baughman KL, Feldman AM, American Heart Association; American College of Cardiology; European Society of Cardiology; Heart Failure Society of America; Heart Failure Association of the European Society of Cardiology, et al. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology. Circulation. 2007;116:2216–33.
Koyama J, Falk RH. Prognostic significance of strain doppler imaging in light-chain amyloidosis. JACC Cardiovasc Imaging. 2010;3:333–42.
Sperry BW, Vranian MN, Hachamovitch R, et al. Are classic predictors of voltage valid in cardiac amyloidosis? A contemporary analysis of electrocardiographic findings. Int J Cardiol. 2016;214:477–81.
Cyrille NB, Goldsmith J, Alvarez J, et al. Prevalence and prognostic significance of low QRS voltage among the three main types of cardiac amyloidosis. Am J Cardiol. 2014;114(7):1089–93.
Vidal-Perez R, Vázquez-García R, Barge-Caballero G, et al. Diagnostic and prognostic value of cardiac imaging in amyloidosis. World J Cardiol. 2020;12(12):599–614.
Martinez-Naharro A, Kotecha T, Norrington K, et al. Native T1 and extracellular volume in transthyretin amyloidosis. JACC Cardiovasc Imaging. 2019;12(5):810–9.
Banypersad SM, Sado DM, Flett AS, et al. Quantification of myocardial extracellular volume fraction in systemic AL amyloidosis: an equilibrium contrast cardiovascular magnetic resonance study. Circ Cardiovasc Imaging. 2013;6(1):34–9.
Yumeng L, **gfen Z, Meng C, et al. 3.0T cardiac magnetic resonance quantification of native T1 and myocardial extracellular volume for the diagnosis of late gadolinium enhancement-negative cardiac amyloidosis. Ann Transl Med. 2022;10(14):794.
Comenzo RL, Reece D, Palladini G, et al. Consensus guidelines for the conduct and reporting of clinical trials in systemic lightchain amyloidosis. Leukemia. 2012;26(11):2317–25.
Kumar S, Dispenzieri A, Lacy MQ, et al. Revised prognostic staging system for light chain amyloidosis incorporating cardiac biomarkers and serum free light chain measurements. J Clin Oncol. 2012;30(9):989–95.
Garcia-Pavia P, Rapezzi C, Adler Y, et al. Diagnosis and treatment of cardiac amyloidosis: a position statement of the ESC working group on myocardial and pericardial diseases. Eur Heart J. 2021;42(16):1554–68.
Kim D, Choi JO, Kim K et al. Untangling amyloidosis: recent advances in cardiac amyloidosis. Int J Heart Fail. 2020;(4).
Palladini G, Campana C, Klersy C, et al. Serum N-terminal pro–brain natriuretic peptide is a sensitive marker of myocardial dysfunction in AL amyloidosis. Circulation. 2003;107(19):2440–5.
Dispenzieri A, Kyle RA, Gertz MA, et al. Survival in patients with primary systemic amyloidosis and raised serum cardiac troponins. Lancet. 2003;361(9371):1787–9.
Dispenzieri A, Gertz MA, Kyle RA, et al. Serum cardiac troponins and N-terminal pro-brain natriuretic peptide: a staging system for primary systemic amyloidosis. J Clin Oncol. 2004;22(18):3751–7.
Wong SW, Hegenbart U, Palladini G, et al. Outcome of patients with newly diagnosed systemic light-chain amyloidosis associated with deletion of 17p. Clin Lymphoma Myeloma Leuk. 2018;18(11):e493–9.
Banypersad SM, Fontana M, Maestrini V, et al. T1 map** and survival in systemic light-chain amyloidosis. Eur Heart J. 2015;36(4):244–51.
Boynton SJ, Geske JB, Dispenzieri A, et al. LGE provides incremental prognostic information over serum biomarkers in AL cardiac amyloidosis. JACC Cardiovasc Imaging. 2016;9(6):680–6.
Hotta VT, Giorgi MCP, Fernandes F, et al. Cardiac amyloidosis: non-invasive diagnosis. Rev Assoc Médica Bras. 2020;66(3):345–52.
Fontana M, Pica S, Reant P, et al. Prognostic value of late gadolinium enhancement cardiovascular magnetic resonance in cardiac amyloidosis. Circulation. 2015;132(16):1570–9.
Agha AM, Palaskas N, Patel AR, et al. Cardiac magnetic resonance predicting outcomes among patients at risk for cardiac AL amyloidosis. Front Cardiovasc Med. 2021;8:626414.
Lin L, Li X, Feng J, et al. The prognostic value of T1 map** and late gadolinium enhancement cardiovascular magnetic resonance imaging in patients with light chain amyloidosis. J Cardiovasc Magn Reson. 2018;20(1):2.
Kellman P, Hansen MS. T1-map** in the heart: accuracy and precision. J Cardiovasc Magn Reson. 2014;16:2.
Weingärtner S, Meßner NM, Budjan J, et al. Myocardial T1-map** at 3T using saturation-recovery: reference values, precision and comparison with MOLLI. J Cardiovasc Magn Reson. 2016;18(1):84.
Piechnik SK, Ferreira VM, Lewandowski AJ, et al. Normal variation of magnetic resonance T1 relaxation times in the human population at 1.5T using ShMOLLI. J Cardiovasc Magn Reson. 2013;15:13.
Gertz MA. Immunoglobulin light chain amyloidosis: 2022 update on diagnosis, prognosis, and treatment. Am J Hematol. 2022;97(6):818–29.
Ritts AJ, Cornell RF, Swiger K, et al. Current concepts of cardiac amyloidosis. Heart Fail Clin. 2017;13(2):409–16.
Acknowledgements
We would like to thank all colleagues for hel** us during the current study.
Funding
This work was supported by the National Key Research and Development Program of China (No. 2017YFC0114300).
Author information
Authors and Affiliations
Contributions
(I) Conception and design: Y Liu, Y Dai, C Hu; (II) Administrative support: C Hu; (III) Provision of study materials or patients: L Wang, M Zhu; (IV) Collection and assembly of data: Y Liu, J Zhu, M Chen; (V) Data analysis and interpretation: Y Liu; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the First Affiliated Hospital of Soochow University (No. 2019112), and was adhered to the 1964 Declaration of Helsinki. Written informed consent was obtained from each included individual.
Consent to publish
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liu, Y., Wang, L., Zhu, J. et al. Prognostic value of native T1 and extracellular volume in patients with immunoglubin light-chain amyloidosis. BMC Cardiovasc Disord 24, 112 (2024). https://doi.org/10.1186/s12872-024-03756-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-024-03756-8