
Abstract
Study design:
Mixed methods, using the Modified Delphi Technique and Expert Panel Review.
Objective:
To evaluate the utility and relevance of the International Spinal Cord Injury (SCI) Core and Basic Data Sets for children and youth with SCI.
Setting:
International.
Methods:
Via 20 electronic surveys, an interprofessional sample of healthcare professionals with pediatric SCI experience participated in an iterative critical review of the International SCI Data Sets, and submitted suggestions for modifications for use with four pediatric age groups. A panel of 5 experts scrutinized the utility of all data sets, correlated any modifications with the develo** National Institute of Neurological Disorders and Stroke (NINDS) pediatric SCI Common Data Elements (CDE) and distributed final recommendations for modifications required to the adult data sets to the International SCI Data Set Committee and the associated Working Groups.
Results:
Two International SCI Data Sets were considered relevant and appropriate for use with children without any changes. Three were considered not appropriate or applicable for use with children, regardless of age. Recommendations were made for five data sets to enhance their relevance and applicability to children across the age groups, and recommendations for seven data sets were specific to infants and younger children.
Conclusions:
The results of this critical review are significant in that substantive recommendations to align the International SCI Core and Basic Data Sets to pediatric practice were made.
Sponsorship:
This project was funded by the Rick Hansen Institute Grant# 2015-27.
Similar content being viewed by others

Introduction
Although there has been significant work on the development of spinal cord injury (SCI) outcomes instruments for adults,1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11 attention to instruments that are developed, validated and standardized for children with SCI remains relatively low and fragmented. The void in agreed upon and psychometrically sound outcome instruments, and the lack of standardization for collecting and recording clinical data limit the ability to evaluate treatment effectiveness, prognosticate the impact of SCI on function and compare outcomes across children and practice patterns. One way to fill this void is to evaluate existing tools that have psychometrically sound support in adult SCI for potential utility for children with SCI. For instance, the motor, sensory and anorectal examinations of the International Standards for Neurological Classification of SCI (ISNCSCI) were originally developed for adult SCI,12 but later field-tested in children with SCI to establish reliability and define the youngest age at which administration of the examinations is feasible.13 Likewise, the Walking Index of Function-II14 and the Spinal Cord Independence Measure-III Self-Report (SCIM-III-SR)15 were developed and validated for adult SCI and later field-tested and validated in children.16, 17 Most recently, pediatric recommendations have been embedded into the National Institutes of Neurologic Disorders and Stroke (NINDS) SCI Common Data Elements.18 Advantages of expanding the applicability of robust adult SCI measures to children, when applicable, include the ability to conduct longitudinal monitoring and compare outcomes across the age span, the potential opportunity for youth to participate in clinical trials, and avoidance of exuberant costs associated with develo** and validating new measures.
The International SCI Data Sets establish a standard for obtaining clinical data that aligns with the International Classification of Functioning, Disability and Health (ICF) and facilitates comparisons of health-related data among adults with SCI.19 The uniform structure of the data sets supports consistency in data collection that allows for the pooling of information worldwide. Additionally, the data sets can serve as a resource for healthcare centers or countries when develo** or upgrading SCI data bases, or for clinicians advancing their SCI-related knowledge.19 The International SCI Data Sets have the potential to make a global impact and are easily assessable to healthcare professionals via the International Spinal Cord Society (ISCoS) website (www.iscos.org.uk.international-sci-data-sets).
Although the existing International SCI Data Sets have a degree of applicability to children who have sustained an SCI, there are additional and different considerations that would need to be addressed for full utility when recording data specific to children aged 0–21 years. Pediatric-onset SCI has additional manifestations that are unique to children. As examples, children are vulnerable to SCIWORA (SCI without radiographic abnormality)20 and the multiple physical immaturities of the spine result in susceptibility of children, especially ages 9 to 16, to multi-level, non-contiguous spinal injuries.21 Also, there is high occurrence of orthopedic complications such as neuromuscular scoliosis and hip dislocation/subluxation.22, 23, 24 Factors associated with the developmental level of the child at the time of injury also impact the ability for a child or parent to respond to questions that require comparison between current level of function and the level of function prior to injury. For instance, very young children with SCI, who would not be expected to have had achieved bowel and bladder control, walking, or sexual activity due to their young age, would not be able to respond. Additionally, at the time of data collection, the child’s stage of cognitive, language and emotional development would likely impact their ability to self-report symptoms such as pain, headache associated with autonomic dysreflexia (AD) and lightheadedness secondary to orthostatic hypertensions. Similarly, children can begin self-reporting about function at approximately 8 years of age.25 Finally, it would seem especially important when collecting data about children to include information related to the family/caregivers and siblings. Family/Caregivers of people who have an SCI experience lower quality of life and are at risk for depression, social isolation and financial stress.26 Though pediatric SCI family/caregiver literature is limited, one study by Valenca, et al.,27 suggests a high caregiver burden with decreased quality of life, as well as increased symptoms of anxiety and depression for caregivers of children with myelomeningocele.
The International SCI Data Sets are organized into one Core Data Set28 and 19 Basic Data Sets.29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46 The Core Data Set standardizes the collection and reporting of the minimum clinical variables that are considered essential during the first inpatient stay after sustaining an SCI.28 In contrast, the International SCI Basic Data Sets define the minimal variables that should be collected in highly relevant areas of routine clinical practice (e.g. spinal interventions and surgical procedures, bowel function, upper-extremity function), at each outpatient encounter.29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46 In addition to the Core and Basic Data Sets, Extended Data Sets have been developed specifically to support research within particular areas.
The International SCI Core and Basic Data Sets could be of great value to pediatric SCI clinicians. Specifically, they would provide clinicians with a common and standardized method for assessing and recording key clinical findings in children. Furthermore, implementation as part of usual care would result in benchmarking capabilities within and across centers, thereby hel** to prognosticate outcomes of care. With the ability to prognosticate, clinicians’ use of anticipatory guidance would be informed by evidence, and parents and youth with SCI would be better prepared for the future. The International SCI Data Sets would be equally valuable to pediatric researchers by creating a common language and by enabling aggregation of data across studies. However, since only a few of the International SCI Data Sets considered children during initial development, prior to widespread pediatric use, a systematic review for relevance of the data sets to children and youth should be conducted. Thus, this paper describes the methods used to systematically review the International SCI Data Sets for relevance to children, and discusses the results of the review, and the recommendations for better alignment of the data sets for pediatric utility.
Materials and methods
The Modified Delphi Technique,47 an iterative critical review process whereby a set of carefully selected items are presented to a field of experts in order to solicit specific information, was used to conduct an iterative review of each of the International SCI Core and Basic Data Sets. Purposeful and snowball sampling were used to recruit pediatric content experts. Health professionals (for example, physicians, psychologists, occupational therapists) with experience in SCI were identified by the investigators through their professional networks and professional organizations, including the American Spinal Injury Association, and the International Spinal Cord Society (purposeful sampling). Those identified were invited via electronic mail (e-mail) to complete a maximum of 20 surveys associated with review of one Core and 19 Basic International SCI Data Sets. Hyperlinks to each survey were sent in waves of three-to-four through individual e-mail invitations distributed over the course of 12 weeks. Participants were encouraged to forward each survey invitation to their colleagues with SCI expertise (snowballing technique) in order to increase the pool of respondents. Surveys were accessed and completed anonymously via survey monkey (https://www.surveymonkey.com/home/). Participants were given one month from the receipt of each survey to submit their response.
Each survey contained seven close-ended demographic questions and one open-ended demographic question (indicate the city, state and country where you practice). The data set-specific instructions included links to the specified data set and the original article associated with the development of the data set, both located within the ISCoS website. The participants were instructed to do the follows: (1) review the data set via the link, (2) consider the variables within the data set for four specified age groups: 0–5 years, 6–12 years, 13–15 years and 16–21 years, (3) submit any suggestions for deletion or addition of variables, and/or changes in how variables are coded. Include the rationale for the change and any references that support the rationale. Using this open-ended format, participants were directed to insert their responses into a content box or use an embedded link to anonymously upload a document with their responses.
The responses from round one were organized by data set, variable within the data set, and age group-specific recommendations. In round two, a table illustrating these results was distributed via a single e-mail to the survey participants in order to elicit further feedback. Two participants offered responses that were integrated into the recommendations. Due to the minimal substantive response in round two, the modified Delphi review was completed.
The final data were presented to a panel of five experts in SCI, including members of the International SCI Data Set Committee. In a two-day meeting, the panel further analyzed the recommendations gathered within the Modified Delphi Technique process. The panel scrutinized the utility of each data set and each variable within each data set, for each of the four pediatric age groups. At the same meeting, these pediatric specific modifications were correlated with the develo** NINDS pediatric SCI Common Data Elements (CDE),48 to ensure harmonization of recommendations. Final recommendations for modifications and further action items were collated and distributed to the International SCI Data Sets Committee Chair for review by the working committees associated with each data set, and integration into future-revised versions of the adult data sets.
Statement of ethics
This study was approved by the Thomas Jefferson University Institutional Review Board.
Results
There were a total of 121 responses across the 20 data set surveys in round 1 of the survey distribution. The responses were submitted anonymously from among the 36 invited participants and their chosen colleagues with expertise in pediatric SCI. Participants could respond to as many as 20 surveys. When a summary of the suggested changes for all 20 round-one data set surveys were sent to participants in the 2nd round of the review, 2 responses were returned. As detailed in Table 1, half of all round 1 responses indicated their primary profession as physician. The majority of responses report greater than 10 years of experience working with pediatric SCI; most responses also report working with more than 25 children with SCI annually (Table 1). Four countries were represented with 60% of responses indicating a geographic location within the United States (US), although 26% of respondents did not report location. In round 2, one US-based physician and one US-based psychologist, both with over 15 years of pediatric SCI experience responded.
The Endocrine and Metabolic Functions, and Skin and Thermoregulation International Data Sets were considered relevant and appropriate, without any changes for use with children across the four age groups, whereas the Activity and Participation, Quality of Life, Pain, Female Sexuality and Reproduction, and Male Sexuality International Data Sets were considered not appropriate or applicable for use with children, regardless of age group. For items on any of the data sets that require self-report, a recommendation was made to provide explicit guidelines for who would provide the response using the following language: 'Where specified, as appropriate in pediatrics, self-report will be primarily by parent for age groups 0–5; and by primarily child for age groups 6–11(parent report, secondary), 12–15 (parent report, supplemental) and 16 and older (parent report, optional).'
As shown in Table 2, there were recommendations for five data sets that would enhance their relevance and applicability to children across the age groups. Two new variables were recommended for the Spinal and Interventions & Procedures Basic Data Set, and one new variable was recommended for the Spinal Column Basic Data Set and Pulmonary Basic Data Set. A recommendation was also made to add response codes of 'unknown' and 'suspected' for some variables, and explicit instructions for their use. In the Pulmonary Basic Data Set, it was recommended to add a comment that provides guidance on how to obtain smoking history in children and youth.
As summarized in Table 3, there were recommended modifications to seven of the International Data Sets that were specific to infants and younger children. The majority of recommended modifications included adding a response option of 'not applicable' or 'unknown', and corresponding comments about age and developmental appropriateness of the variable. In the Urinary Tract Infection (UTI) Basic Data Set, the recommendation was made to add 'fussiness and irritability' as one of the response options for the variable 'signs and symptoms of UTI' as these are manifestations of UTI in children. Similarly, a recommendation was made to change the variable name 'Uneasiness, headache or perspiration during defecation' (Bowel Function Basic Data Set) to 'Uneasiness, headache, fussiness and irritability.' It was recommended to add a response 'Birth Injury' for Injury Etiology in the Core Data Set, and 'Hip instability, subluxation and pelvic obliquity' to the Musculoskeletal Basic Data Set.
Discussion
A systematic and iterative review of the International SCI Data Sets that were originally developed for adults was conducted by international pediatric content experts. The goal was to establish pediatric recommendations for the data sets so that they could be used to facilitate the ability to pool pediatric data worldwide and thereby provide a mechanism for comparisons and benchmarks of a relatively large number of children with SCI. As was done for the pediatric review of the SCI NINDS CDE,48 we reviewed the International SCI Basic Data Sets for each of the four age groups defined by DeVivo and colleagues (2011),38 owing to the importance of growth and development, and their influence on the relevance of each variable, and the feasibility of collecting the information using the standardized codes.
While the International Endocrine and Metabolic Functions Basic Data Set and Skin and Thermoregulation Basic Data Sets were felt to be appropriate for children without any modification, the other data sets that focus on body functions were viewed as highly relevant to pediatric practice, and require only a few easily achieved modifications. The addition of response codes 'Unknown' and 'Not Applicable' for variables that cannot or should not be obtained in infants and children is a simple modification that is needed for several variables in The Lower Urinary Tract Function, Urinary Tract Infection, Urodynamics, Upper Extremity, Bowel Function and Musculoskeletal Basic Data Sets. The recommended inclusion of comments that correspond with 'Unknown' and 'Not Applicable' would increase the likelihood of standardization. As an example, several variables in the Bowel Function Basic Data Set address methods and frequency of bowel programs, and frequency of fecal incontinence, which are areas of little relevance for infants and young children who developmentally would not be expected to be continent even without an SCI. A response option of 'Not Applicable', and a corresponding comment that provides an indication of the age range where continence is expected, would potentially help with recording the clinical data accurately over time. Likewise, in the Musculoskeletal Basic Data Set, a response option of 'Not Applicable' for the question 'Do any of the above musculoskeletal challenges interfere with your activities of daily living' would allow pediatric clinicians to systematically record musculoskeletal impairments in very young children child, without having to comment on the impact on activities of daily living (ADL). Once the child ages, and engagement in ADL is expected, the response could be recorded differently on a repeated administration. The argument is somewhat similar for adding the response option 'Suspected' for variables such as heterotrophic ossification and AD, where the condition is suspected, but difficult to confirm in children due to the inability to express symptoms such as headache in children of 5 years of age and younger. In this instance, however, it is an addition to reflect the nonspecific manifestations of AD or lack of normative references, and insufficient data.
There were other recommendations. Additional variables that are highly relevant to pediatric SCI were created for the Core Data Set (birth injury), Musculoskeletal Basic Data Set (hip instability, subluxation, pelvic obliquity), Spinal Interventions and Procedures Basic Data Set (non-surgical treatment, cervical traction and immobilization; stabilization via wire/instrumentation without fusion), Spinal Column Basic Data Set (SCIWORA) and Pulmonary Basic Data Sets (Exposure to tobacco at home). Although rare (1 per 60 000 births), birth injuries are usually due to difficult deliveries, result in tetraplegia and may be associated with a brachial plexus injury or hypoxic ischemic encephalopathy.49 Following pediatric review of the NINDS SCI CDE,48 birth injury was added as a variable to the domain of 'Injury History', and a birth injury-specific case report form (CRF) was developed. Likewise, tobacco exposure at home was added to the NINDS SCI CDE following pediatric review.48 Including these two variables in the International SCI Data Sets strengthens the harmonization of the SCI International Data Sets and the NINDS CDE. The addition of a variable to monitor hip instability/subluxation and pelvic obliquity aligns the Musculoskeletal Basic Data Set with standard of care, where routine, longitudinal surveillance of the hip is the mainstay of orthopedic management for children with SCI due to its high occurrence,50, 51 especially in children who are injured at younger than 10 years of age.52 Likewise, the additional variables in the Spinal Interventions and Procedures and Spinal Column Basic Data Sets strengthen the alignment of the data sets with pediatric standard of care. Spine stabilization in young children often involves halo immobilization with or without traction and/or surgical stabilization without fusion.53, 54 As children may undergo both immobilization and surgery, it was recommended to add a comment for the response options 'Check all that Apply.' Despite the regular use of Magnetic Resonance Imaging, and other advanced imaging, SCIWORA is still a term used in pediatric practice to describe pediatric SCI without plain radiographic or computerized tomography scan findings,20 and hence it was developed as a new variable to be added to the Spinal Column Basic Data Set.
In addition to adding new variables, recommendations were made to change the variable name 'Uneasiness, headache, or perspiration during defecation' (Bowel Function Data Set version 2.0) to 'Uneasiness, headache, fussiness, irritability during defecation', and to include 'fussiness and irritability' as a response option for 'Signs and Symptoms of UTI' (Urinary Tract Infection Basci Data Set). These recommendations were based on the work by Hickey and colleagues,55 who studied clinical symptoms in children and adolescents with SCI during episodes of AD, and found an association between fussiness/irritability and UTI and AD in very young children.
The Pulmonary and Urinary Tract Imaging Data Sets were not recommended for the 0- to 5-year age group, and the Activity and Participation, Quality of Life, Pain, Female Sexuality and Reproduction, and Male Sexuality International Data Sets were considered inappropriate for each of the four pediatric age groups. Inclusion of pediatric expertise on the committees that review and revise the Pulmonary, Urinary Tract Imaging, Female Sexuality and Reproduction and Male Sexuality International Data Sets is planned. Development of Pain Quality of Life and Activity and Participation Data Sets for Children requires commitment from one or several people to bring together pediatric content experts and engage them in a sustaining and productive fashion, until completion of the work.
There was a glaring void in data sets for other highly relevant areas in pediatric SCI, including upright and wheeled mobility, school, caregivers and siblings. Future work on develo** pediatric quality of life and activity and participation data sets could possibly include school and siblings. Adult and pediatric experts working to revise the International SCI Basic Data Sets are currently collaborating with experts associated with the NINDS CDE for SCI to develop common data sets for caregivers and mobility.
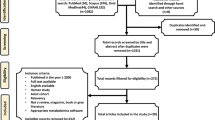
Moving forward, the pediatric recommendations will be integrated into the existing International SCI Core and Basic Data Sets through a systematic process (Figure 1) that will involve careful consideration of the pediatric recommendations by each of the appropriate International SCI Data Set working committees at the time these working committees review the adult core and basic data sets and modify them to reflect new knowledge or practice patterns. All of the new changes, including the pediatric recommendations, will be reviewed and endorsed by the international SCI community, prior to solidification of the revised data set. The Bowel Function Basic Data Set has recently been reviewed, and revisions including the pediatric recommendations from the work described in this paper were integrated and will be disseminated as version 2.0 of this data set.56 Moreover, as a way to better facilitate pediatric considerations into the revisions of the International Core and Basic Data Sets, a pediatric content expert has been added to the International SCI Data Sets Committee, and will serve to ensure inclusion of pediatric content experts on working groups. Work is planned to develop pediatric training cases, and to educate pediatric providers about the International SCI Data Sets, and their uses.

Iterative Review Process for International SCI Data Sets Pediatric Recommendatios. CDE, Common Data Elements; NINDS, National institute of Neurologic Disorders and Stoke; SCI, spinal cord injury.
Conclusion
Recommendations to align the International SCI Core and Basic Data Sets to pediatric practice have been provided to the International SCI Data Sets Committee chair to distribute to working groups that are reviewing and updating the International SCI Core and Basic Data Sets. These working groups will review the recommendations, and embed them into subsequent versions of the data sets prior to release. Working groups to create new pediatric data sets are needed for pain, quality of life, activity and participation. Further work is needed to develop SCI data sets for school, caregiver/parent and youth, and pediatric training cases for the data sets need to be developed to support clinical uptake and use.
Data archiving
There were no data to deposit.
References
Jackson AB, Carnel CT, Ditunno JF, Read MS, Boninger ML, Schmeler MR et al. Gait and Ambulation Subcommittee. Outcome measures for gait and ambulation in the spinal cord injury population. J Spinal Cord Med 2008; 31: 487–499.
Miller WC, Sakibara BM, Noonan VK, Tawashy AE, Aubut JL, Curt A et al. SCIRE: Outcome Measures. 2010; Available from www.scireproject.com./sites/default/files/outcomemeasures.pdf.
Hill MR, Noonan VK, Sakakibara MB, Miller WC, the SCIRE Research Team. Quality of life instruments and definitions in individuals with spinal cord injury: a systematic review. Spinal Cord 2010; 48: 512–521.
Lam T, Noonan V, Eng JJ . A systematic review of the functional ambulation outcomes in spinal cord injury. Spinal Cord 2008; 46: 246–254.
Noonan VK, Miller WC, Noreau L . A review of instruments assessing participation in the person with spinal cord injury. Spinal Cord 2009; 47: 435–446.
Sakakibara BM, Miller WC, Orenczuk SG, Wolfe DL, the SCIRE Research Team. A systematic review of depression and anxiety measures using in individuals with spinal cord injury. Spinal Cord 2009; 47: 841–851.
Alexander M, Anderson K, Biering-Sorensen F, Blight F, Bryce T, Creay G et al. Outcome measures in spinal cord injury. Recent assessment and recommendations for future directions. Spinal Cord 2009; 47: 582–591.
Anderson KD, Aito S, Atkins M, Biering-Sorensen F, Charlifue S, Curt A et al. Functional recovery measures for spinal cord measures for spinal cord injury: an evidence based review of clinical practice and research. J Spinal Cord Med 2008; 31: 133–144.
Furlan JC, Noonan V, Singh A, Fehlings MG . Assessment of disability in patients with acute traumatic spinal cord injury: a systematic review of the literature. J Neurotrauma 2011; 28: 1413–1430.
Magasi S, Post MW . A comparative review of contemporary participation measures’ psychometric properties and content coverage. Arch Phys Med Rehab 2010; 91: S17–S28.
Tulsky D, Kisala PA, Victorson D, Tate D, Heinemann AW, Amtmann D et al. Develo** a contemporary patient-reported outcomes measure for spinal cord injury. Arch Phys Med Rehabil 2011; 92 (10 S): S44–S51.
Kirshblum SC, Burns SP, Biering-Sorensen F, Donovan W, Graves DE, Jha A et al. International standards for neurological classification of spinal cord injury (Revised 2011). J Spinal Cord Med 2011 34: 535–546.
Mulcahey MJ, Vogel L, Betz R, Samdani A, Chafetz R, Gaughan J . The international standards for neurological classification of spinal cord injury: psychometric evaluation and guidelines for use with children and youth. Phys Med Rehabil 2011; 92: 1264–1269.
Ditunno PL, Ditunno JF . Walking index for spinal cord injury (WISCI-II): scale revision. Spinal Cord 2001; 39: 654–656.
Calhoun C, Mulcahey MJ . Validity and reliability of the Walking Index of Function in children with spinal cord injury. Pediatric J Phys Medicine and Rehab 2012; 5: 275–279.
Fekete C, Eriks-Hoogland I, Baumberger M, Catz A, Itzkovich M, Luthi H et al. Development and validation of a self-report version of the spinal independence measure (SCIM III). Spinal Cord 2013; 51: 40–47.
Mulcahey MJ, Calhoun C, Vogel L, Kelly E, Sinko. R . The Spinal Cord Independence Measure Self Report for Youth. Spinal Cord 2016; 54: 204–2012.
Biering-Sorensen F, Alai S, Anderson K, Charlifue S, Chen Y, DeVivo M et al. Common data elements for spinal cord injury clinical research: a National Institute for Neurological Disorders and Stroke project. Spinal Cord 2015; 53: 265–277.
Biering-Sørensen F, Charlifue S, DeVivo M, Noonan V, Stripling T, Wing P . International spinal cord injury data sets. Spinal Cord 2006; 44: 530–544.
Lustrin ES, Karakas SP, Ortiz AO, Cinnamon J, Castillo M, Vaheesan K et al. Pediatric cervical spine: normal anatomy, variants, and trauma. Radiographics 2003; 23: 539–560.
Mortazavi MM, Dogan S, Civelek E, Tubbs RS, Theodore N, Rekate H et al. Pediatric multilevel spine injuries: an institutional experience. Childs Nerv Syst 2011; 27: 1095–1100.
Rink P, Miller F . Hip instability in spinal cord injury patients. J Pediatric Orthopedics. 1990; 10: 583–587.
Vogel LC, Krajci KA, Anderson CJ . Adults with pediatric onset spinal cord injury: part 2: musculoskeletal and neurological complications. J Spinal Cord Med 2002; 25: 117–123.
McCarthy J,J, Chafetz RS, Betz RR, Gaughan J . Incidence and degree of hip subluxation/dislocation in children with spinal cord injury. J of Spinal Cord Med 2004; 27 (Supp 1): S80–S83.
Mulcahey MJ, Calhoun C, Riley A, Haley SM . Children’s reports of activity and participation after sustaining a spinal cord injury: a cognitive interviewing study. Dev Neurorehabil 2009; 12: 191–200.
Adelman RD, Tmanova LL, Delgado D, Dion S, Lachs MS . Caregiver burden: a clinical review. J Am Med Assoc 2014; 311: 1052–1060.
Valenca MP, de Menezes TA, Calado AA, de Aguiar Cavalcanti G . Burden and quality of life among caregivers of children and adolescents with meningomyelocele: measuring the relationship to anxiety and depression. Spinal Cord 2012; 50: 553–557.
DeVivo M, Biering-Sørensen F, Charlifue S, Noonan V, Post M . Strip International Spinal Cord Injury Core Data Set. Spinal Cord 2006; 44: 535–540.
Alexander MS, Biering-Sørensen F, Elliott S, Kreuter M, Sønksen J . International spinal cord injury female sexual and reproductive function basic data set. Spinal Cord 2011; 49: 787–790.
Alexander MS, Biering-Sørensen F, Elliott S, Kreuter M, Sønksen J . International spinal cord injury male sexual function basic data set. Spinal Cord 2011; 49: 795–798.
Biering-Sørensen F, Charlifue S, DeVivo M, Noonan V, Post M, Stripling T et al. International Spinal Cord Injury Data Sets. Spinal Cord 2006; 44: 530–534.
Biering-Sørensen F, Craggs M, Kennelly M, Schick E, Wyndaele JJ . International Lower Urinary Tract Function Basic Spinal Cord Injury Data Set. Spinal Cord 2008; 46: 325–330.
Biering-Sørensen F, Craggs M, Kennelly M, Schick E, Wyndaele JJ . International urodynamic basic spinal cord injury data set. Spinal Cord 2008b; 46: 513–516.
Biering-Sørensen F, Craggs M, Kennelly M, Schick E, Wyndaele JJ . International urinary tract imaging basic spinal cord injury data set. Spinal Cord 2009; 47: 379–383.
Biering-Sørensen F, Krassioukov A, Alexander MS, Donovan W, Karlsson A-K, Mueller G et al. International spinal cord injury pulmonary function basic data set. Spinal Cord 2012; 50: 418–421.
Biering-Sørensen F, Burns AS, Curt A, Harvey LA, Mulcahey MJ, Nance PW et al. International spinal cord injury musculoskeletal basic data set. Spinal Cord 2012; 50: 797–802.
Charlifue S, Post MW, Biering-Sørensen F, Catz A, Dijkers M, Geyh S et al. International spinal cord injury quality of life basic data set. Spinal Cord 2012; 50: 672–675.
Devivo MJ, Biering-Sørensen F, New P, Chen Y . Standardization of data analysis and reporting of results from the International Spinal Cord Injury Core Data Set. Spinal Cord 2011; 49: 596–599.
Dvorak MF, Wing PC, Fehlings MG, Vaccaro AR, Itshavek E, Biering –Sorenson F et al. International spinal cord injury spinal column injury basic data set. Spinal Cord 2012; 50: 817–821.
Goetz LL, Cardenas DD, Kennelly M, Bonne Lee BS, Linsenmeyer T, Moser C et al. International spinal cord injury urinary tract infection basic data set. Spinal Cord 2013; 51: 700–704.
Krassioukov A, Alexander MS, Karlsson AK, Donovan W, Mathias CJ, Biering-Sørensen F . International spinal cord injury cardiovascular function basic data set. Spinal Cord 2010; 48: 586–590.
Krogh K, Perkash I, Stiens SA, Biering-Sørensen F . International bowel function basic spinal cord injury data set. Spinal Cord 2009; 47: 230–234.
Krogh K, Perkash I, Stiens SA, Biering-Sørensen F . International bowel function extended spinal cord injury data set. Spinal Cord 2009; 47: 235–241.
Lee BB, Cripps RA, Woodman RJ . Development of an international spinal injury prevention module: application of the international classification of external cause of injury to spinal cord injury. Spinal Cord 2010; 48: 498–503.
Biering-Sørensen F, Bryden A, Curt A, Friden J, Harvey LA, Mulcahey MJ et al. International spinal cord injury upper extremity basic data set. Spinal Cord 2014; 52: 652–657.
Widerström-Noga E, Biering-Sørensen F, Bryce TN, Cardenas DD, Finnerup NB, Jensen MP et al. The international spinal cord injury pain basic data set (version 2.0). Spinal Cord 2014; 52: 282–286.
Dalkey NC, Rourke DL Experimental assessment of Delphi procedures with group value judgments In: Dalkey NC, Rourke DL, Lewis R, Snyder D (eds). Studies in the Quality of Life: Delphi and Decision-Making. Lexington Books: Lexington, MA, USA. 1972.
Mulcahey MJ, Vogel LC, Sheikh M, Arango-Lasprilla JC, Augutis M, Garner E et al. Recommendations for the National Institute for Neurologic Disorders and Stroke spinal cord injury common data elements for children and youth with SCI. Spinal Cord (e-pub ahead of print 15 November 2016; doi:10.1038/sc.2016.139).
Medlock MD, Hanigan WC . Neurologic birth trauma, intra-cranial, spinal cord, and brachial plexus injury. Clin Perinatol 1997; 24: 845–857.
Rink P, Miller F . Hip instability in spinal cord injury patients. J Pediatr Orthop 1990; 10: 583–587.
Vogel LC, Krajci KA, Anderson CJ . Adults with pediatric onset spinal cord injury: part 2: musculoskeletal and neurological complications. J Spinal Cord Med 2002; 25: 117–123.
McCarthy JJ, Chafetz RS, Betz RR, Gaughan J . Incidence and degree of hip subluxation/dislocation in children with spinal cord injury. J Spinal Cord Med 2004; 27 (Supp 1): S80–S83.
Rebok G, Riley A, Forrest G, Starfield B, Green B, Robertson J et al. Elementary school-aged children’s reports of their health: A cognitive interviewing study. Qual Life Res 2001; 10: 59–70.
Riley AW . Evidence that school-age children can self- report on their health. Ambul Pediatr 2004; 4 (Suppl 4): 371–376.
Hickey KJ, Vogel LC, Willis KM, Anderson CJ . Prevalence and etiology of AD in children with spinal cord injuries. J. Spinal Cord 2004; 27: S54–S60.
Krogh K, Emmanuel A, Perrouin-Verbe B, Korsten MA, Mulcahey MJ, Biering-Sørensen F . International spinal cord injury bowel function basic data set (Version 2.0). Spinal Cord (e-pub ahead of print 14 February 2017; doi:10.1038/sc.2016.189).
Acknowledgements
Professionals who participated in the Modified Delphi Technique are acknowledged for their expertise and contributions to the recommendations. The study was funded by the Rick Hansen Institute Grant #2015-27, (Mulcahey, PI).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
Dr VKN is an employee of Rick Hansen Institute. The remaining authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Carroll, A., Vogel, L., Zebracki, K. et al. Relevance of the international spinal cord injury basic data sets to youth: an Inter-Professional review with recommendations. Spinal Cord 55, 875–881 (2017). https://doi.org/10.1038/sc.2017.14
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2017.14
- Springer Nature Limited