
Abstract
Objectives
We studied the epidemiology of primary bloodstream infections (BSIs), secondary BSIs, and central line-associated BSIs (CLABSIs) and applicability of CDC definitions for primary sources of infection causing secondary BSIs in patients in the neonatal ICU.
Study design
We classified healthcare-associated BSIs (HABSIs) as primary BSIs, secondary BSIs, and CLABSIs using CDC surveillance definitions and determined their overall incidence and incidence among different gestational age strata. We assessed the applicability of CDC definitions for infection sources causing secondary BSIs.
Results
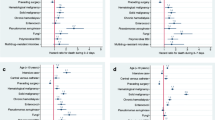
From 2010 to 2019, 141 (32.7%), 202 (46.9%), and 88 (20.4%) HABSIs were classified as primary BSIs, secondary BSIs, and CLABSIs, respectively; all declined during the study period (all p < 0.001). Gestational age <28 weeks was associated with increased incidence of all HABSI types. CDC criteria for site-specific primary sources were met in 137/202 (68%) secondary BSIs.
Conclusions
Primary and secondary BSIs were more common than CLABSIs and should be prioritized for prevention.




Similar content being viewed by others


Data availability
The datasets generated during and/or analyzed during the current study are not publicly available due to privacy reasons relating to the sensitivity of the data collected but are available from the corresponding author on reasonable request and with the permission of the Columbia IRB and NewYork-Presbyterian Hospital.
References
Brady MT. Health care–associated infections in the neonatal intensive care unit. Am J Infect Control. 2005;33:268–75.
Romanelli RMC, Anchieta LM, Mourão MVA, Campos FA, Loyola FC, Mourão PHO, et al. Risk factors and lethality of laboratory-confirmed bloodstream infection caused by non-skin contaminant pathogens in neonates. J Pediatr Versão Em Port. 2013;89:189–96.
Sewell E, Roberts J, Mukhopadhyay S. Association of infection in neonates and long-term neurodevelopmental outcome. Clin Perinatol. 2021;48:251–61.
Pearlman SA. Quality improvement to reduce neonatal CLABSI: the journey to zero. Am J Perinatol. 2020;37:S14–7.
Balla KC, Rao SPN, Arul C, Shashidhar A, Prashantha YN, Nagaraj S, et al. Decreasing central line-associated bloodstream infections through quality improvement initiative. Indian Pediatr. 2018;55:753–6.
Mobley RE, Bizzarro MJ. Central line-associated bloodstream infections in the NICU: successes and controversies in the quest for zero. Semin Perinatol. 2017;41:166–74.
Polin RA, Denson S, Brady MT, Committee on Fetus and Newborn, Committee on Infectious Diseases. Epidemiology and diagnosis of health care–associated infections in the NICU. Pediatrics. 2012;129:e1104–9.
Polin RA, Denson S, Brady MT. Strategies for prevention of health care–associated infections in the NICU. Pediatrics. 2012;129:9.
National Healthcare Safety Network. Bloodstream Infection Event (Central-Line Associated Bloodstream Infection and Non-central Line Associated Bloodstream Infection) [Internet]. cdc.gov; 2021. Available from: https://www.cdc.gov/nhsn/pdfs/pscmanual/4psc_clabscurrent.pdf.
National Healthcare Safety Network. Late Onset Sepsis/Meningitis Event [Internet]. cdc.gov; 2021. Available from: https://www.cdc.gov/nhsn/pdfs/neonatal/losmen/los-men-protocol-508.pdf.
National Healthcare Safety Network. CDC/NHSN Surveillance Definitions for Specific Types of Infections [Internet]. cdc.gov; 2021. Available from: https://www.cdc.gov/nhsn/pdfs/pscmanual/17pscnosinfdef_current.pdf.
National Healthcare Safety Network. Pneumonia (Ventilator-associated [VAP] and non-ventilatorassociated Pneumonia [PNEU]) Event [Internet]. cdc.gov; 2023. Available from: https://www.cdc.gov/nhsn/pdfs/pscmanual/6pscvapcurrent.pdf.
National Healthcare Safety Network. Urinary Tract Infection (Catheter-Associated Urinary Tract Infection [CAUTI] and Non-Catheter-Associated Urinary Tract Infection [UTI]) Events [Internet]. cdc.gov; 2023. Available from: https://www.cdc.gov/nhsn/pdfs/pscmanual/7psccauticurrent.pdf.
National Healthcare Safety Network. Surgical Site Infection Event (SSI) [Internet]. cdc.gov; 2023. Available from: https://www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf.
Coggins SA, Glaser K. Updates in late-onset sepsis: risk assessment, therapy, and outcomes. NeoReviews. 2022;23:738–55.
Stoll BJ, Gordon T, Korones SB, Shankaran S, Tyson JE, Bauer CR, et al. Late-onset sepsis in very low birth weight neonates: a report from the National Institute of Child Health and Human Development Neonatal Research Network. J Pediatr. 1996;129:63–71.
Lee SM, Chang M, Kim KS. Blood culture proven early onset sepsis and late onset sepsis in very-low-birth-weight infants in Korea. J Korean Med Sci. 2015;30:S67.
Hornik CP, Fort P, Clark RH, Watt K, Benjamin DK, Smith PB, et al. Early and late onset sepsis in very-low-birth-weight infants from a large group of neonatal intensive care units. Early Hum Dev. 2012;88:S69–74.
Stoll BJ, Hansen N, Fanaroff AA, Wright LL, Carlo WA, Ehrenkranz RA, et al. Late-onset sepsis in very low birth weight neonates: the experience of the NICHD neonatal research network. Pediatrics. 2002;110:285–91.
Wirtschafter DD, Powers RJ, Pettit JS, Lee HC, Boscardin WJ, Ahmad Subeh M, et al. Nosocomial infection reduction in VLBW infants with a statewide quality-improvement model. Pediatrics. 2011;127:419–26.
Zhou Q, Ong M, Lan M, Ye XY, Ting JY, Shah PS, et al. Decreasing trend in incidence of late onset culture positive bloodstream infections but not late onset meningitis in preterm infants <33 Weeks gestation in Canadian neonatal intensive care unit. Neonatology. 2022;119:60–7.
Pharande P, Lindrea KB, Smyth J, Evans M, Lui K, Bolisetty S. Trends in late‐onset sepsis in a neonatal intensive care unit following implementation of infection control bundle: a 15‐year audit. J Paediatr Child Health. 2018;54:1314–20.
Lee SK, Shah PS, Singhal N, Aziz K, Synnes A, McMillan D, et al. Association of a quality improvement program with neonatal outcomes in extremely preterm infants: a prospective cohort study. Can Med Assoc J. 2014;186:E485–94.
Zipursky AR, Yoon EW, Emberley J, Bertelle V, Kanungo J, Lee SK, et al. Central line-associated blood stream infections and non–central line-associated blood stream infections surveillance in canadian tertiary care neonatal intensive care units. J Pediatr. 2019;208:176–182.e6.
Advani SD, Murray TS, Murdzek CM, Aniskiewicz MJ, Bizzarro MJ. Shifting focus toward healthcare-associated bloodstream infections: The need for neonatal intensive care unit–specific NHSN definitions. Infect Control Hosp Epidemiol. 2019;41:181–6.
van der Zwet WC, Kaiser AM, van Elburg RM, Berkhof J, Fetter WPF, Parlevliet GA, et al. Nosocomial infections in a Dutch neonatal intensive care unit: surveillance study with definitions for infection specifically adapted for neonates. J Hosp Infect. 2005;61:300–11.
Contreras-Cuellar GA, Leal-Castro AL, Prieto R, Carvajal-Hermida AL. Device-associated infections in a Colombian neonatal intensive care unit. Rev Salud Públ. 2007;9:439–47.
Barbadoro P, Marigliano A, D’Errico MM, Carnielli V, Prospero E. Gestational age as a single predictor of health care‒associated bloodstream infections in neonatal intensive care unit patients. Am J Infect Control. 2011;39:159–62.
Auriti C, Ronchetti MP, Pezzotti P, Marrocco G, Quondamcarlo A, Seganti G, et al. Determinants of nosocomial infection in 6 neonatal intensive care units: an Italian multicenter prospective cohort study. Infect Control Hosp Epidemiol. 2010;31:926–33.
Deng C, Li X, Zou Y, Wang J, Wang J, Namba F, et al. Risk factors and pathogen profile of ventilator-associated pneumonia in a neonatal intensive care unit in China: Neonatal VAP: risk and pathogen. Pediatr Int. 2011;53:332–7.
Foglia EE, Lorch SA. Clinical predictors of urinary tract infection in the neonatal intensive care unit. J Neonatal-Perinat Med. 2012;5:327–33.
Robbins M, Trittmann J, Martin E, Reber KM, Nelin L, Shepherd E. Early extubation attempts reduce length of stay in extremely preterm infants even if re-intubation is necessary. J Neonatal-Perinat Med. 2015;8:91–7.
Manuck TA, Rice MM, Bailit JL, Grobman WA, Reddy UM, Wapner RJ, et al. Preterm neonatal morbidity and mortality by gestational age: a contemporary cohort. Am J Obstet Gynecol. 2016;215:103.e1–103.e14.
Murki S, Vardhelli V, Deshabhotla S, Sharma D, Pawale D, Kulkarni D, et al. Predictors of length of hospital stay among preterm infants admitted to neonatal intensive care unit: data from a multicentre collaborative network from India (INNC: Indian National Neonatal Collaborative). J Paediatr Child Health. 2020;56:1584–9.
Swerkersson S, Jodal U, Åhrén C, Sixt R, Stokland E, Hansson S. Urinary tract infection in infants: the significance of low bacterial count. Pediatr Nephrol. 2016;31:239–45.
Kanellopoulos TA, Vassilakos PJ, Kantzis M, Ellina A, Kolonitsiou F, Papanastasiou DA. Low bacterial count urinary tract infections in infants and young children. Eur J Pediatr. 2005;164:355–61.
Alnor AB, Vinholt PJ. Paediatric reference intervals are heterogeneous and differ considerably in the classification of healthy paediatric blood samples. Eur J Pediatr. 2019;178:963–71.
Acknowledgements
The authors would like to acknowledge the support received from the Divisions of Neonatology and Infectious Diseases in the Department of Pediatrics at Columbia University Irving Medical Center. We would also like to acknowledge Sonia Gollerkeri for her contributions to the statistical analyses.
Funding
AAP and IF were supported by the training grant “Training in Pediatric Infectious Diseases” (National Institute of Allergy and Infectious Diseases T32AI007531, PI: Saiman).
Author information
Authors and Affiliations
Contributions
LS was responsible for the conception of this project. AP, EG, KS, SM, IF, LA, SB, and LS were involved in the design and implementation. AP, EG, KS, SM, IF, and LA were responsible for acquisition of data and together with MM, SB, and LS analyzed and interpreted the data. AP was primarily responsible for writing the initial draft of the manuscript, which was edited by LS, SB, EG, and IF. All authors have reviewed the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Paul, A.A., Gentzler, E., Solowey, K. et al. Epidemiology, risk factors, and applicability of CDC definitions for healthcare-associated bloodstream infections at a level IV neonatal ICU. J Perinatol 43, 1152–1157 (2023). https://doi.org/10.1038/s41372-023-01728-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41372-023-01728-y
- Springer Nature America, Inc.
This article is cited by
-
Systematic culture of central catheters and infections related to catheters in a neonatal intensive care unit: an observational study
Scientific Reports (2024)
-
Impact of active surveillance and decolonization strategies for methicillin-resistant Staphylococcus aureus in a neonatal intensive care unit
Journal of Perinatology (2024)