
Abstract
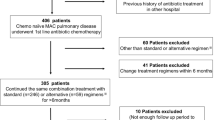
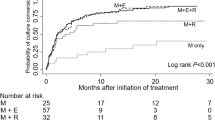
Despite recent advances in chemotherapy, the treatment of pulmonary Mycobacterium avium complex (MAC) disease remains unsatisfactory. Judging from its MIC, fluoroquinolones including gatifloxacin (GFLX) are expected to demonstrate efficacy against MAC disease. However, there have been few clinical studies using fluoroquinolones. Therefore, a prospective study to evaluate the clinical efficacy and safety of a fluoroquinolone-containing regimen for the treatment of pulmonary MAC disease was conducted. In this trial, patients with pulmonary MAC disease received protocol-guided combined chemotherapy with rifampin (RFP) and ethambutol (EB) plus either GFLX or clarithromycin (CAM). Adult patients who fulfilled the criteria of the ATS definition of pulmonary MAC disease were enrolled in this study. The patients provided their informed consent, and treatments were administered for 1 year. Of 27 patients enrolled from three facilities, 14 patients were treated with the CAM-containing regimen and 13 patients were treated with the GFLX-containing regime. Four patients did not complete the 1-year treatment because of adverse events. Nine patients (64.3%) in the CAM group and 11 patients (84.6%) in the GFLX group achieved eradication of pathogens. Adverse events were observed more frequently in the GFLX group than in the CAM group. However, there were no severe adverse events in either group. The long-term results showed a similar relapse rate between the CAM and GFLX groups. The fluoroquinolone-containing regimen demonstrated both high efficacy and relative safety for pulmonary MAC disease that was similar to that of the CAM-containing regimen, which is considered to be the standard regimen.
Similar content being viewed by others

References
Medical Section of the American Lung Association. Diagnosis and treatment of disease caused by nontuberculous mycobacteria. Am J Respir Crit Care Med 1997;156:S1–S25.
Griffith DE, Aksamit T, Brown-Elliott BA, Catanzaro A, Daley C, Gordin F, et al. ATS Mycobacterial Diseases Subcommittee; American Thoracic Society; Infectious Disease Society of America. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007;175:367–416.
McGrath EE, McCabe J, Anderson PB. American Thoracic Society; Infectious Diseases Society of America. Guidelines on the diagnosis and treatment of pulmonary non-tuberculous mycobacteria infection. Int J Clin Pract. 2008;62:1947–55.
Wallace RJ Jr, Brown BA, Griffith DE, Girard WM, Murphy DT. Clarithromycin regimens for pulmonary Mycobacterium avium complex: the first 50 patients. Am J Respir Crit Care Med. 1996;153:1766–72.
Griffith DE, Brown BA, Girard WM, Griffith BE, Couch LA, Wallace RJ Jr. Azithromycin-containing regimens for treatment of Mycobacterium avium complex lung disease. Clin Infect Dis. 2001;32:1547–53.
Tanaka E, Kimoto T, Tsuyuguchi K, Watanabe I, Matsumoto H, Niimi A, et al. Effect of clarithromycin regimen for Mycobacterium avium complex pulmonary disease. Am J Respir Crit Care Med. 1999;160:866–72.
Corpe RF. Surgical management of pulmonary disease due to Mycobacterium avium–intracellulare. Rev Infect Dis. 1981;3:1064–7.
Moran JF, Alexander LG, Stauh EW, Young WG, Sealy WC. Long-term results of pulmonary resection for atypical mycobacterial disease. Am Thorac Surg. 1983;35:597–604.
Kobashi Y, Yoshida K, Miyashita N, Niki Y, Oka M. Relationship between clinical efficacy of treatment of pulmonary Mycobacterium avium complex disease and drug-sensitivity testing of Mycobacterium avium complex isolates. J Infect Chemother. 2006;12:195–202.
Kobashi Y, Matsushima T, Oka M. A double-blind randomized study of aminoglycoside infusion with combined therapy for pulmonary Mycobacterium avium complex disease. Respir Med. 2007;101:130–8.
Wallace RJ Jr, Nash DR, Steele LC, Steingrube V. Susceptibility testing of slowly growing mycobacteria by a microdilution MIC method with 7H9 broth. J Clin Microbiol. 1986;24:976–81.
Park-Wyllie LY, Juurlink DN, Kopp A, Shah BR, Stukel TA, Stumpo C, et al. Outpatient gatifloxacin therapy and dysglycemia in older adults. N Engl J Med. 2006;354:1352–61.
Cynamon MH, Sklaney M. Gatifloxacin and ethionamide as the foundation for therapy of tuberculosis. Antimicrob Agents Chemother. 2003;47:2442–4.
Sano C, Tatano Y, Shimizu T, Yamabe S, Sato K, Tomioka H. Comparative in vitro and in vivo antimicrobial activities of sitafloxacin, gatifloxacin and moxifloxacin against Mycobacterium avium. Int J Antimicrob Agents. 2011;37:296–301.
Kohno Y, Ohno H, Miyazaki Y, Higashiyama Y, Yanagihara K, Hirakata Y, et al. In vitro and in vivo activities of novel fluoroquinolones alone and in combination with clarithromycin against clinically isolated Mycobacterium avium complex strains in Japan. Antimicrob Agents Chemother. 2007;51:4071–6.
Bermudez LE, Kolonoski P, Petrofsky M, Wu M, Inderlied CB, Young LS. Mefloquine, moxifloxacin, and ethambutol are a triple-drug alternative to macrolide-containing regimens for treatment of Mycobacterium avium disease. J Infect Dis. 2003;187:1977–80.
Horiguchi T, Kondo R, Miyazaki J, Shiga M, Sugiyama M, Handa M, Munekata E. Antibacterial activity and clinical efficacy of sparfloxacin in Mycobacterium avium–intracellulare complex infection. J Int Med Res. 2004;32:530–9.
Jenkins PA, Campbell IA, Banks J, Gelder CM, Prescott RJ, Smith AP. Clarithromycin vs ciprofloxacin as adjuncts to rifampicin and ethambutol in treating opportunist mycobacterial lung diseases and an assessment of Mycobacterium vaccae immunotherapy. Thorax. 2008;63:627–34.
Wallace RJ, Brown BA, Griffith DE, Girard WM, Murphy DT, Onyi GO, et al. Initial clarithromycin monotherapy for Mycobacterium avium–intracellulare complex lung disease. Am J Respir Crit Care Med. 1994;149:1335–41.
Dautzenberg B, Piperno D, Diot P, Trufot-Pernot C, Chauvin JP. Clarithromycin Study Group of France. Clarithromycin in the treatment of Mycobacterium avium patients without AIDS. Chest. 1995;107:1035–40.
Iseman MD. Medical management of pulmonary diseases caused by Mycobacterium avium complex. Clin Chest Med. 2002;23:633–41.
Acknowledgments
We appreciate the assistance of Dr. Brian Quinn for editing the English in this manuscript.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Fujita, M., Kajiki, A., Tao, Y. et al. The clinical efficacy and safety of a fluoroquinolone-containing regimen for pulmonary MAC disease. J Infect Chemother 18, 146–151 (2012). https://doi.org/10.1007/s10156-011-0303-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10156-011-0303-5