
Abstract
Background
Posterior cerebral artery (PCA) P1-2 segment dissecting aneurysms are difficult because regular craniectomy aneurysm clip** or intravascular interventional therapy is not applicable.
Method
We report distal clip** of a PCA P1-2 segment dissection aneurysm with an anterior cerebral artery (ACA) A1-radial artery graft-PCA P2 bypass.
Conclusion
This case demonstrates the value of an ACA-RAG-PCA bypass in the therapy of a PCA dissecting aneurysm.



Similar content being viewed by others


References
Kawashima A, Andrade-Barazarte H, Jahromi BR, Oinas M, Elsharkawy A, Kivelev J, Kubota Y, Kawamata T, Hernesniemi JA (2017) Superficial temporal artery: distal posterior cerebral artery bypass through the subtemporal approach: technical note and pilot surgical cases. Oper Neurosurg (Hagerstown) 13:309–316
Lekovic GP, Ooi YC, Jahan R (2021) Presigmoid transpetrosal approach for superficial temporal artery to distal posterior cerebral artery bypass and trap** of aneurysm. Oper Neurosurg (Hagerstown) 20:E234–E238
Ota N, Goehre F, Miyazaki T, Kinoshita Y, Matsukawa H, Yanagisawa T, Sakakibara F, Saito N, Miyata S, Noda K, Tsuboi T, Kamiyama H, Tokuda S, Kamada K, Tanikawa R (2016) Bypass revascularization applied to the posterior cerebral artery. World Neurosurg 96:460–472
Shenoy VS, Lavergne P, Qazi Z, Ghodke BV, Sekhar LN (2021) Distal basilar artery “umbrella aneurysm” treated by radial artery graft bypass from the external carotid artery to posterior cerebral artery and clip trap**: 2-dimensional operative video. Oper Neurosurg (Hagerstown) 21:E250–E251
Sun Y, Gao K, Shi M, Shang Y, Tong X (2022) Superficial temporal artery-posterior cerebral artery bypass through zygomatic anterior temporal approach for complex posterior cerebral artery aneurysm. World Neurosurg 159:110–119
Acknowledgements
The authors thank Qiang Xu and Yingtao Liu for imaging processing and Geng Xu for intraoperative electrophysiological monitoring support.
Funding
This study was supported by the Outstanding Academic Leaders Program of Shanghai Municipal Commission of Health and Family Planning (No. 2017BR006 to WZ), Clinical Research Plan of SHDC (No. SHDC2020CR2034B to W. Z., No. SHDC2020CR4033 to K. Q.), Shanghai Municipal Science and Technology Major Project (No. 2018SHZDZX01) and ZJ Lab, and CAMS Innovation Fund for Medical Sciences (CIFMS, 2019-I2 M-5–008).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Research involving human participants
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Huashan Hospital Institutional Review Board (HIRB), Fudan University, Shanghai, China.
Informed consent
It represents a video of a surgical case. The patient gave approval for this publication.
Patient consent
The patient gave approval for publication of this case.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Key points
1. It is difficult to clip or reconstruct the intracranial dissecting aneurysm.
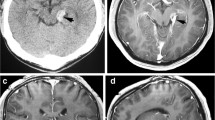
2. Preoperative high-resolution MRI helps operators assess intramural thrombi and atherosclerosis of the aneurysm wall.
3. AcomA and bilateral well-developed A1 allow bypass using the A1 as the donor. A compression test or balloon occlusion test (BOT) should be performed to evaluate AcomA contralateral compensation.
4. The vessel grafts can be the radial artery or the great saphenous vein.
5. Sufficient sylvian fissure and cistern split are needed for intracranial pressure control and donor vascular exposure.
6. Part of the temporal lobe can be removed when P2 exposure is difficult.
7. When the intracranial pressure in a patient with SAH is difficult to decrease, the lamina terminalis can be opened, or lumbar puncture and intraventricular drainage can be placed before surgery.
8. ICG, Doppler, and SEP/MEP are quick measures to determine the bypass patency and limb dysfunction caused by the blood flow change.
9. Intraoperative DSA can be used to assess the bypass patency and aneurysm distal clip**. The hybrid technique also provides a potential salvage selection, such as coiling, to close the aneurysm after bypass.
10. At least one DSA follow-up is required after discharge.
This article is part of the Topical Collection on Vascular Neurosurgery - Aneurysm
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 (MP4 105750 KB) This video illustrates a left posterior cerebral artery P1-2 segment dissecting aneurysm distal clip** via an A1-RAG-P2 bypass.
Rights and permissions
About this article

Cite this article
Liu, P., Shi, Y., An, Q. et al. How I do it: left posterior cerebral artery P1-2 segment dissecting aneurysm distal clip** via an A1-RAG-P2 bypass. Acta Neurochir 164, 2447–2451 (2022). https://doi.org/10.1007/s00701-022-05293-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-022-05293-9