
Abstract
Introduction and Hypothesis
The potential predictors of pelvic floor reconstruction surgery hypothermia remain unclear. This prospective cohort study was aimed at identifying these predictors and evaluating the outcomes associated with perioperative hypothermia.
Methods
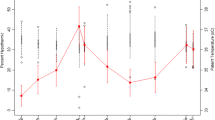
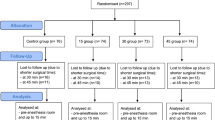
Elderly patients undergoing pelvic floor reconstruction surgery were consecutively enrolled from April 2023 to September 2023. Perioperative temperature was measured at preoperative (T1), every 15 min after the start of anesthesia (T2), and 15 min postoperative (T3) using a temperature probe. Perioperative hypothermia was defined as a core temperature below 36°C at any point during the procedure. Multivariate logistic regression analysis was conducted to determine factors associated with perioperative hypothermia.
Results
A total of 229 patients were included in the study, with 50.7% experiencing hypothermia. Multivariate analysis revealed that the surgical method involving pelvic floor combined with laparoscopy, preoperative temperature < 36.5°C, anesthesia duration ≥ 120 min, and the high levels of anxiety were significantly associated with perioperative hypothermia. The predictive value of the multivariate model was 0.767 (95% CI, 0.706 to 0.828).
Conclusions
This observational prospective study identified several predictive factors for perioperative hypothermia in elderly patients during pelvic floor reconstruction surgery. Strategies aimed at preventing perioperative hypothermia should target these factors. Further studies are required to assess the effectiveness of these strategies, specifically in elderly patients undergoing pelvic floor reconstruction surgery.


Similar content being viewed by others

Data Availability
The datasets used during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ASA:
-
American Standards Association
- BMI:
-
Body mass index
- LOS:
-
Length of hospital stay
- PFD:
-
Pelvic floor dysfunction
- PONV:
-
Postoperative nausea and vomiting
- SAS:
-
Self-rating Anxiety Scale
References
Wilkins MF, Wu JM. Lifetime risk of surgery for stress urinary incontinence or pelvic organ prolapse. Minerva Ginecol. 2017;69(2):171–7.
Abdel-Fattah M, Familusi A, Fielding S, Ford J, Bhattacharya S. Primary and repeat surgical treatment for female pelvic organ prolapse and incontinence in parous women in the UK: a register linkage study. BMJ Open. 2011;1(2):e000206.
Torossian A, Bräuer A, Höcker J, Bein B, Wulf H, Horn EP. Preventing inadvertent perioperative hypothermia. Dtsch Arztebl Int. 2015;112(10):166–72.
Frisch NB, Pepper AM, Rooney E, Silverton C. Intraoperative hypothermia in total hip and knee arthroplasty. Orthopedics. 2017;40(1):56–63.
Ryczek E, White J, Poole RL, Reeves NL, Torkington J, Carolan-Rees G. Normothermic insufflation to prevent perioperative hypothermia and improve quality of recovery in elective colectomy patients: protocol for a randomized controlled trial. JMIR Res Protoc. 2019;8(12):e14533.
Billeter AT, Hohmann SF, Druen D, Cannon R, Polk HC Jr. Unintentional perioperative hypothermia is associated with severe complications and high mortality in elective operations. Surgery. 2014;156(5):1245–52.
Melling AC, Ali B, Scott EM, Leaper DJ. Effects of preoperative warming on the incidence of wound infection after clean surgery: a randomised controlled trial. Lancet. 2001;358(9285):876–80.
Frank SM, Fleisher LA, Breslow MJ, et al. Perioperative maintenance of normothermia reduces the incidence of morbid cardiac events. A randomized clinical trial. JAMA. 1997;277(14):1127–34.
Rajagopalan S, Mascha E, Na J, Sessler DI. The effects of mild perioperative hypothermia on blood loss and transfusion requirement. Anesthesiology. 2008;108(1):71–7.
Bock M, Müller J, Bach A, Böhrer H, Martin E, Motsch J. Effects of preinduction and intraoperative warming during major laparotomy. Br J Anaesth. 1998;80(2):159–63.
Grassi G, Seravalle G, Turri C, Bertinieri G, Dell’Oro R, Mancia G. Impairment of thermoregulatory control of skin sympathetic nerve traffic in the elderly. Circulation. 2003;108(6):729–35.
Vandenbroucke JP, von Elm E, Altman DG, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. Ann Intern Med. 2007;147(8):W163–94.
Zung WW. A rating instrument for anxiety disorders. Psychosomatics. 1971;12(6):371–9.
Desgranges FP, Bapteste L, Riffard C, et al. Predictive factors of maternal hypothermia during Cesarean delivery: a prospective cohort study. Can J Anaesth. 2017;64(9):919–27.
Sultan P, Habib AS, Cho Y, Carvalho B. The effect of patient warming during caesarean delivery on maternal and neonatal outcomes: a meta-analysis. Br J Anaesth. 2015;115(4):500–10.
Kim EJ, Yoon H. Preoperative factors affecting the intraoperative core body temperature in abdominal surgery under general anesthesia: an observational cohort. Clin Nurse Spec. 2014;28(5):268–76.
Long KC, Tanner EJ, Frey M, et al. Intraoperative hypothermia during primary surgical cytoreduction for advanced ovarian cancer: risk factors and associations with postoperative morbidity. Gynecol Oncol. 2013;131(3):525–30.
Horn EP, Bein B, Broch O, et al. Warming before and after epidural block before general anaesthesia for major abdominal surgery prevents perioperative hypothermia: a randomised controlled trial. Eur J Anaesthesiol. 2016;33(5):334–40.
Scott AV, Stonemetz JL, Wasey JO, et al. Compliance with Surgical Care Improvement Project for body temperature management (SCIP Inf-10) is associated with improved clinical outcomes. Anesthesiology. 2015;123(1):116–25.
Yi J, **ang Z, Deng X, et al. Incidence of inadvertent intraoperative hypothermia and its risk factors in patients undergoing general anesthesia in Bei**g: a prospective regional survey. PLoS One. 2015;10(9):e0136136.
Matsukawa T, Kurz A, Sessler DI, Bjorksten AR, Merrifield B, Cheng C. Propofol linearly reduces the vasoconstriction and shivering thresholds. Anesthesiology. 1995;82(5):1169–80.
De Witte JL, Kim JS, Sessler DI, Bastanmehr H, Bjorksten AR. Tramadol reduces the sweating, vasoconstriction, and shivering thresholds. Anesth Analg. 1998;87(1):173–9.
Torossian A, Bein B, Bräuer A, et al. Leitlinie “Vermeidung von perioperativer Hypothermie”—Aktualisierung. 2019. Available online: https://www.awmf.org/awmf-online-das-portal-der-wissenschaftlichen-medizin/awmf-aktuell.html. Accessed on 1 July 2021.
Tekgul ZT, Pektas S, Yildirim U, et al. A prospective randomized double-blind study on the effects of the temperature of irrigation solutions on thermoregulation and postoperative complications in percutaneous nephrolithotomy. J Anesth. 2015;29(2):165–9.
Fischer S, Haas F, Strahler J. A systematic review of thermosensation and thermoregulation in anxiety disorders. Front Physiol. 2021;12:784943.
Lopez MB. Postanaesthetic shivering—from pathophysiology to prevention. Rom J Anaesth Intensive Care. 2018;25(1):73–81.
Jun JH, Chung MH, Jun IJ, et al. Efficacy of forced-air warming and warmed intravenous fluid for prevention of hypothermia and shivering during caesarean delivery under spinal anaesthesia: a randomised controlled trial. Eur J Anaesthesiol. 2019;36(6):442–8.
Sessler DI. Perioperative thermoregulation and heat balance. Lancet. 2016;387(10038):2655–64.
Funding
No funding was received.
Author information
Authors and Affiliations
Contributions
C.-C.Z and Y.J.: study design and writing the paper; X.-F.-Q. performed the statistical analysis; Z.-F.Z. assisted with the English polishing and editing process of the article; R.-Z.S. and X.-Y.L.: patient recruitment and data collection. All authors have read the manuscript and approved the final paper submitted.
Corresponding author
Ethics declarations
Ethics Statement
This single-center, prospective observational study was conducted from 28 April 2023 to 28 September 2023, with approval from the Ethics Committee of Hangzhou Women's Hospital (IRB: 202203–10).
Copyright Transfer Statement
The copyright to this article is transferred to the International Urogynecology Journal when the article is accepted for publication. The copyright transfer covers the exclusive right to reproduce and distribute the article, including reprints, translations, photographic reproductions, microform, electronic form (offline, online) or any other reproductions of a similar nature.
Consent to Publish
Not applicable.
Conflicts of Interest
None.
Additional information
Handling Editor: Holly E. Richter
Editor in Chief: Maria A. Bortolini
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Trial number and registry URL: ChiCTR2300070782; http://www.chictr.org.cn , Principal investigator: Jiang; date of registration: 28 April 2023
Supplementary information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Jiang, Y., Zhou, Zf., Shao, Rz. et al. Perioperative Hypothermia in Elderly Patients During Pelvic Floor Reconstruction Surgery: An Observational Study. Int Urogynecol J (2024). https://doi.org/10.1007/s00192-024-05781-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00192-024-05781-9