
Abstract
Purpose
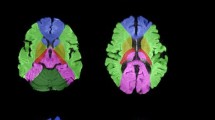
The purpose of this study was to determine if there is an association between the proximal thoracic aortic (ascending aorta and aortic arch) atheroma and ischemic brain lesions on diffusion-weighted magnetic resonance imaging (DW-MRI) after on-pump (ONCAB) and off-pump (OPCAB) coronary artery bypass surgery.
Methods
Patients who underwent ONCAB surgery (n = 13) and who had aortic atheroma > 2 mm were compared to a risk-adjusted prospective cohort of patients (n = 13) undergoing OPCAB surgery. Transesophageal echocardiography and epiaortic scanning were performed to assess the proximal thoracic aorta. Patients were evaluated for new ischemic brain lesions utilizing DW-MRI three to seven days after surgery. The NEECHAM confusion scale was used to evaluate patient consciousness.
Results
The groups were comparable with respect to demographic data, and prevalence of preoperative risk factors. The extent and severity of aortic atheroma was similar in the two groups. The average maximum height of atheroma was 5.0 ± 2.0 mm in the OPCAB and 4.8 ± 1.9 in the ONCAB groups, respectively. The prevalence of new ischemic brain lesions on DW-MRI was 0% in the OPCAB group and 61 % in the ONCAB group (P = 0.001). Patients in the OPCAB group were less confused during the first two postoperative days.
Conclusion
Patients with aortic atheroma > 2 mm may have a lower risk of new ischemic brain lesions as identified by DW-MRI after OPCAB surgery. Patient stratification based upon aortic atheroma burden should be addressed in future trials designed to tailor treatment strategies to improve short- and long-term neurological outcomes in patients undergoing cardiac surgery.
Résumé
Objectif
Déterminer s’il y a une association entre l’athérome de l’aorte thoracique proximale (aorte ascendante et crosse de l’aorte) et les lésions cérébrales ischémiques à l’examen d’imagerie par résonance magnétique pondérée par diffusion (IRM-PD) à la suite du pontage aortocoronarien avec circulation extracorporelle (PACCE) et un PAC à cœur battant (PACCB).
Méthode
Des patients subissant un PACCE (n = 13) et ayant de l’athérome aortique > 2 mm ont été comparés à une cohorte prospective de patients à risque ajusté (n = 13) subissant un PACCB. L’échocardiographie transœsophagienne et le balayage épiaortique ont permis d’évaluer l’aorte thoracique proximale. La présence de nouvelles lésions cérébrales ischémiques a été vérifiée avec l’IRM-PD trois à sept jours après l’opération. La conscience des patients a été évaluée par l’échelle de confusion NEECHAM.
Résultats
Les données démographiques et à la prévalence de facteurs de risque préopératoires intergroupes étaient comparables. L’étendue et la sévérité de l’athérome aortique étaient aussi similaires. La hauteur maximale moyenne de l’athérome était de 5,0 ± 2,0 mm pour le groupe de PACCB et de 4,8 ± 1,9 pour le groupe de PACCE. La prévalence de nouvelles lésions cérébrales ischémiques à l’IRM-PD était de0% avec PACCB et de 61 % avec le PACCE (P = 0,001). Les patients de PACCB étaient moins confus pendant les deux premiers jours postopératoires.
Conclusion
Les patients avec athérome aortique > 2 mm peuvent présenter un risque plus faible de lésions cérébrales ischémiques comme l’a montré l’IRM-PD après le PACCB. La stratification des patients selon le degré d’athérome aortique devrait être étudiée ultérieurement pour adapter les traitements visant à améliorer les résultats à court et à long terme chez les patients qui subissent une intervention chirurgicale cardiaque.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Selnes OA, Goldsborough MA, Borowicz LM, McKhann GM. Neurobehavioural sequelae of cardiopulmonary bypass. Lancet 1999; 353:1601–6.
Newman MF, Kirchner JL, Phillips-Bute B, et al.; Neurological Outcome Research Group; Cardiothoracic Anesthesiology Research Endeavors Investigators. Longitudinal assessment of neurocognitive function after coronary-artery bypass surgery. N Engl J Med 2001; 344:395–402.
Borger MA, Ivanov J, Weisel RD, Rao V, Peniston CM. Stroke during coronary bypass surgery: principal role of cerebral macroemboli. Eur J Cardiothorac Surg 2001; 19:627–32.
Davila-Roman VG, Barzilai B, Wareing TH, Murphy SF, Schechtman KB, Kouchoukos NT. Atherosclerosis of the ascending aorta: prevalence and role as an independent predictor of cerebrovascular events in cardiac patients. Stroke 1994; 25:2010–6.
Mizuno T, Toyama M, Tabuchi N, et al. Thickened intima of the aortic arch is a risk factor for stroke with coronary artery bypass grafting. Ann Thorac Surg 2000; 70:1565–70.
van der Linden J, Had**ikolaou L, Bergman P, Lindblom D. Postoperative stroke in cardiac surgery is related to the location and extent of atherosclerotic disease in the ascending aorta. J Am Coll Cardiol 2001; 38:131–5.
Katz ES, Tunick PA, Rusinek H, Ribakove G, Spencer FC, Kronzon I. Protruding aortic atheromas predict stroke in elderly patients undergoing cardiopulmonary bypass: experience with intraoperative transesophageal echocardiography. J Am Coll Cardiol 1992; 20:70–7.
Tunick PA, Kronzon I. Atheromas of the thoracic aorta: clinical and therapeutic update. J Am Coll Cardiol 2000; 35:545–54.
Djaiani G, Fedorko L, Borger M, et al. Mild to moderate atheromatous disease of the thoracic aorta and new ischemic brain lesions after conventional coronary artery bypass graft surgery. Stroke 2004; 35:e356–8.
Ura M, Sakata R, Nakayama Y, Goto T. Ultrasonographic demonstration of manipulation-related aortic injuries after cardiac surgery. J Am Coll Cardiol 2000; 35:1303–10.
Neelon VJ, Champagne MT, Carlson JR, Funk SG. The NEECHAM confusion scale: construction, validation, and clinical testing. Nurs Res 1996; 45:324–30.
Toner I, Peden CJ, Hamid SK, Newman S, Taylor KM, Smith PL. Magnetic resonance imaging and neuropsy-chological changes after coronary artery bypass graft surgery: preliminary findings. J Neurosurg Anesthesiol 1994; 6:163–9.
Vanninen R, Aikia M, Kononen M, et al. Subclinical cerebral complications after coronary artery bypass grafting. Prospective analysis with magnetic resonance imaging, quantitative electroencephalography, and neuropsychological assessment. Arch Neurol 1998; 55:618–27.
Bendszus M, Reents W, Franke D, et al. Brain damage after coronary artery bypass grafting. Arch Neurol 2002; 59:1090–5.
Restrepo L, Wityk RJ, Grega MA, et al. Diffusion- and perfusion-weighted magnetic resonance imaging of the brain before and after coronary artery bypass grafting surgery. Stroke 2002; 33:2909–15.
Knipp SC, Matatko N, Wilhelm H, et al. Evaluation of brain injury after coronary artery bypass grafting. A prospective study using neuropsychological assessment and diffusion-weighted magnetic resonance imaging. Eur J Cardiothorac Surg 2004; 25:791–800.
Abu-Omar Y, Cifelli A, Matthews PM, Taggart DP. The role of microembolisation in cerebral injury as defined by functional magnetic resonance imaging. Eur J Cardiothorac Surg 2004; 26:586–91.
Bowles BJ, Lee JD, Dang CR, et al. Coronary artery bypass performed without the use of cardiopulmonary bypass is associated with reduced cerebral microemboli and improved clinical results. Chest 2001; 119:25–30.
Lee JD, Lee SJ, Tsushima WT, et al. Benefits of off-pump bypass on neurologic and clinical morbidity: a prospective randomized trial. Ann Thorac Surg 2003; 76:18–25.
Lund C, Hol PK, Lundblad R, et al. Comparison of cerebral embolization during off-pump and on-pump coronary artery bypass surgery. Ann Thorac Surg 2003; 76:765–70.
Watters MP, Cohen AM, Monk CR, Angelini GD, Ryder IG. Reduced cerebral embolic signals in beating heart coronary surgery detected by transcranial Doppler ultrasound. Br J Anaesth 2000; 84:629–31.
Cheng DC, Bainbridge D, Martin JE, Novick RJ; Evidence-Based Perioperative Clinical Outcomes Research Group. Does off-pump coronary artery bypass reduce mortality, morbidity, and resource utilization when compared with conventional coronary artery bypass? A meta-analysis of randomized trials. Anesthesiology 2005; 102:188–203.
Wijeysundera DN, Beattie WS, Djaiani GN, et al. Off-pump coronary artery surgery for reducing mortality and morbidity. Meta-analysis of randomized and observational studies. J Am Coll Cardiol 2005; 46:872–82.
Grossi EA, Bizekis CS, Sharony R, et al. Routine intraoperative transesophageal echocardiography identifies patients with atheromatous aortas: impact on «off-pump» coronary artery bypass and perioperative stroke. J Am Soc Echocardiogr 2003; 16:751–5.
Kapetanakis EI, Stamou SC, Dullum MK, et al. The impact of aortic manipulation on neurologic outcomes after coronary artery bypass surgery: a risk-adjusted study. Ann Thorac Surg 2004; 78:1564–71.
Lev-Ran O, Braunstein R, Sharony R, et al. No-touch aorta off-pump coronary surgery: the effect on stroke. J Thorac Cardiovasc Surg 2005; 129:307–13.
Baker MD, Moody DM, Field AS, Yen YF, Hammon JW, Stump DA. Advanced magnetic resonance imaging techniques of perfusion and diffusion in evaluation of postsurgical brain injury: preliminary results in coronary artery surgery on and off cardiopulmonary bypass. Ann Thorac Surg 2002; 73:S367.
Friday G, Sutter F, Curtin A, et al. Brain magnetic resonance imaging abnormalities following off-pump cardiac surgery. Heart Surg Forum 2005; 8:E105–9.
Singer MB, Chong J, Lu D, Schonewille WJ, Tuhrim S, Atlas SW. Diffusion-weighted MRI in acute subcortical infarction. Stroke 1998; 29:133–6.
Guadagno JV, Calautti C, Baron JC. Progress in imaging stroke: emerging clinical applications. Br Med Bull 2003; 65:145–57.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests: None declared.
Rights and permissions
About this article
Cite this article
Djaiani, G., Fedorko, L., Cusimano, R.J. et al. Off-pump coronary bypass surgery: risk of ischemic brain lesions in patients with atheromatous thoracic aorta. Can J Anesth 53, 795–801 (2006). https://doi.org/10.1007/BF03022796
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03022796