
Abstract
Background
Segmental hypoplasia of liver is an infrequently encountered congenital anomaly which is clinically indolent and detected incidentally on cross sectional imaging or abdominal surgery which can have a myriad of surgical and medical implications. The unique radiological manifestations and associated complications makes it a diagnostically challenging entity.
Case presentation
We report a case of a middle-aged female presenting with complaints of non-specific abdominal pain for two years in which we reported the presence of segmental hypoplasia of right lobe complicated by development of portal hypertension incidentally detected on ultrasound examination which was followed up and confirmed on cross sectional imaging.
Conclusions
In this case report, we present a unique instance of congenital segmental hypoplasia of the liver, highlighting the intricacies of its radiological presentation, potential clinical implications, and the challenges associated with its diagnosis. By examining this rare anomaly, we aim to contribute to the growing body of knowledge surrounding hepatic developmental disorders, fostering a deeper understanding of the clinical spectrum, and facilitating improved patient care through enhanced diagnostic awareness.
Similar content being viewed by others


Background
Segmental hypoplasia of liver is a rare and underdiagnosed congenital anomaly with an incidence of 0.005% [1] with no specific clinical symptoms to alert the treating physician. Diagnosis is mostly reliant on cross-sectional imaging and hence radiologists should be aware of this rare albeit important congenital anomaly along with its associated complications. This case report aims to highlight the radiological manifestations of this anomaly along with the associated challenges with its diagnosis and briefly touch upon the clinical and surgical caveats in such patients.
Case presentation
A 45-year-old Indian lady presented to medicine outpatient department of Safdarjung Hospital, New Delhi, India with complaints of recurrent episodes of abdominal pain for the past two years. Ultrasound whole abdomen with colour and spectral doppler examination of spleno-portal axis was performed on a high-resolution ultrasound scanner [Philips Affiniti 70G] which revealed enlarged left lobe of liver measuring 5 cm × 19.5 cm with non-visualization of anterior segments of right lobe of liver resulting in hypoplastic right lobe and posterior segment of right lobe measuring 5.6 cm × 7.9 cm (Fig. 4a). Liver appeared normal in echotexture with no focal lesions. Portal vein was dilated in caliber (14.5 mm, Fig. 4b) showing normal spectral doppler waveform with dilated left branch of portal vein along with few periportal collaterals and an enlarged spleen(14 cm) suggestive of portal hypertension. The patient did not have ascites. Gall bladder was partially distended with echo free lumen, common bile duct was not dilated. Contrast enhanced triple phase CT (computed tomography) scan of abdomen was acquired from domes of diaphragm to ischial tuberosities with multiplanar reconstruction done on a 256 slice multidetector CT scanner [Somatom Definition Flash, Siemens Erlangen, Germany] after administration of intravenous contrast [70 mL of non-ionic iodinated contrast (350 mg/ mL Iohexol)]. CECT (contrast enhanced computed tomography) revealed absence of Couinoids segments VII and VIII of right lobe of liver with the space being filled by omental fat resulting in hypoplastic right lobe of liver with relative enlargement of the left lobe and volume redistribution (Fig. 1a). The caudate lobe was normal. The main portal vein was dilated with its right branch being smaller with absence of anterior branch of right portal vein (Fig. 2b). Multiple dilated tortuous abnormal collateral vessels were detected in periportal, peripancreatic and perisplenic location. Hepatic veins and IVC were normal in caliber and contrast opacification. The liver was however normal in attenuation and enhancement with normal smooth surface. No focal liver lesions or dilatation of intra hepatic biliary radicles was present. The gall bladder was malpositioned postero-superiorly between hypoplastic right lobe and hepatic flexure (Figs. 1b and 3a]. Gall bladder was normal in size, shape with normal wall thickness, intraluminal attenuation and enhancement (Fig. 1b). The right kidney was located at a higher position as compared to left (Fig. 2a). CE-MRI scan was done on a 3 Tesla MRI scanner [GE healthcare, Milwaukee, WI, USA] and findings were well correlated with previous CT findings showing hypoplastic right lobe of liver (Figs. 3 and 5). Liver parenchyma showed normal signal intensity on all pulse sequences. No history of any previous abdominal surgery, chronic liver disease, abdominal trauma, prior hepatic infection/abscess or intake of hepatotoxic medication was present. All liver and renal functional tests were within normal range. After excluding these acquired causes of liver atrophy, notable absence of vascular supply to right lobe from right anterior portal vein and associated positional anomalies of adjacent organs supported the fact that hypoplasia was indeed congenital. Patient was managed conservatively and followed up on out patient basis for monitoring of portal hypertension and requirement of therapeutic interventions.

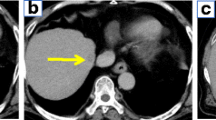
a Axial post contrast CT image shows hypoplastic anterior segments of right lobe and hypertrophied left lobe of liver (long white arrow). Colonic interposition is seen between right lobe of liver and right hemidiaphragm (small white arrow). b Axial CECT image shows ectopic gall bladder lying postero-superiorly between hypoplastic right lobe and Hepatic flexure (white arrow)

a Coronal CECT image shows higher position of right kidney as compared to left kidney (white arrow). b MIP reconstructed CT image shows smaller caliber right branch of Portal vein with absence of right anterior segmental branches. Dilated left branch and main portal vein is seen with normal post contrast opacification (white arrow)

a Axial T2w fat saturated MRI image showing colonic interposition between right lobe of liver and right hemidiaphragm and ectopic location of gall bladder (white arrow). b Axial T2w MRI image showing enlarged left lobe of liver (small white arrow) and an enlarged bulky spleen (splenic index of 760) (long white arrow)

a Ultrasound image of abdomen showing enlarged left lobe of liver with hypoplastic right lobe (white arrow). b Ultrasound image showing dilated main portal vein (long white arrow) with caliber of 14.5 mm with few dilated branches of left portal vein (small white arrow)

a Axial CE-T1w MRI image showing hypoplastic right lobe with absence of anterior segments with space being occupied by omental fat and hepatic flexure (white arrow). b MIP reconstructed CE-T1w MRI image showing formation of main portal vein with smaller caliber of right portal vein and larger caliber of left portal vein (white arrow)
Discussion
The liver is divided into a larger right lobe and a smaller left lobe by the falciform ligament and the fissures for the ligamentum teres and ligamentum venosum. Advanced imaging methods have improved our understanding of hepatic anatomy, including vascular and biliary structures. Agenesis or underdevelopment of the liver, particularly the right hepatic lobe, is a rare anomaly. In autopsy studies, the incidence of lobar aplasia or hypoplasia is reported to be 0.005% [1]. About 65 cases of aplasia or hypoplasia of the right hepatic lobe have been documented in medical literature [2]. The diagnosis of complete agenesis of a hepatic lobe can be made when none of the intraparenchymal structures- the portal vein, hepatic vein or intrahepatic bile ducts are visible [3]. When at least one of the three structures are visible it is rather atrophy/hypoplasia of a segment[3]. In our case right hepatic vein was present, right branch of portal vein was present but was smaller in caliber compared to left branch owing to absence of right anterior poral vein.
It is frequently associated with other anomalies of hepato-biliary system alongside the misplacement of adjacent organs that could be erroneously interpreted as pathological. Most common associations include an ectopic location of gallbladder, colonic interposition between liver and right hemidiaphragm, elevated right kidney, enlarged left hepatic lobe and caudate lobe, diaphragmatic hernia, and persistent umbilical vein [4]. This case showed an ectopic gallbladder lying postero-superiorly between the hypoplastic right lobe and the hepatic flexure (suprahepatic location), other previously reported locations were retrohepatic or subhepatic [2]. Retrohepatic, intrahepatic and retroduodenal ectopic locations of gall bladder have also been reported with isolated left lobe agenesis [5].These findings must be reported to alert the surgeon about these anatomical variations which have implications in laparoscopic cholecystectomy, while not being a contraindication it may require different placement of laparoscopic instruments [6, 7]. Colonic interposition and higher position of right kidney were also seen in this case (Fig. 3a).
Complications include formation of gallstones, biliary strictures, development of portal hypertension [2, 3, 8, 9]. The likely etiology of portal hypertension in these cases appears to be an imbalance between portal inflow and the reduced capacity of the portal vascular bed due to decreased number of intrahepatic portal branches coupled with an increase in vascular resistance of right portal vein branches. The compensation mechanism to prevent portal hypertension acts by increasing the density of left lobe vasculature [7]. In the current case main portal vein and left branch were dilated with multiple peripancreatic, perisplenic and perigastric tortuous collaterals. No gallstones or bile duct stricture was present.
The diagnosis of hepatic hypoplasia holds significant importance in the context of liver transplantation, influencing both pre-transplant assessments and the overall transplantation process. Accurate diagnosis helps in determining the size and configuration of the liver graft. Knowledge of the variations in vascular and biliary configuration is crucial during transplantation to prevent complications such as vascular thrombosis or bile duct complications. This knowledge significantly contributes to surgical planning, reduces the risk of complications, and ultimately improves the overall success and outcomes of liver transplantation procedures [10].
Our patient had abnormal hepatic morphology characterized by small right lobe with enlarged left lobe, portal hypertension and splenomegaly, hence differential diagnosis of liver cirrhosis, cholangiocarcinoma, idiopathic portal hypertension, prior surgical resection, prior hepatic trauma/infection were considered and excluded by clinical history, laboratory and imaging findings. Therefore, the cause of hepatic hypoplasia being congenital is more feasible.
Conclusions
Liver segmental hypoplasia is a rare and unique abnormality with vital imaging findings and associated organ malpositions and potential complications such as portal hypertension which radiologists need to interpret and communicate to the clinicians for timely management of these patients and averting serious surgical complications.
Availability of data and materials
Data sharing is not applicable to this article, as no datasets were generated or analyzed during the current study.
Abbreviations
- CT:
-
Computed tomography
- CECT:
-
Contrast enhanced computed tomography
- IVC:
-
Inferior vena cava
- MRI:
-
Magnetic resonance imaging
- CE-MRI:
-
Contrast enhanced magnetic resonance imaging
References
Sato N, Kawakami K, Matsumoto S, Toyonaga T, Ishimitsu T, Nagafuchi K et al (1998) Agenesis of the right lobe of the liver: report of a case. Surg Today 28:643–646
Kabaroudis A, Papaziogas B, Atmatzidis K, Argiriadou E, Paraskevas A, Galanis I et al (2003) Hypoplasia of the right hepatic lobe combined with a floating gallbladder. Acta Chir Belg 103:425–427
Chou CK, Mak CW, Lin MB, Tzeng WS, Chang JM (1998) CT of agenesis and atrophy of the right hepatic lobe. Abdom Imaging 23:603–607
Swarup MS, Bhatt S, Tandon A, Mandal S (2018) Segmental hypoplasia of liver: the importance of radiologic recognition and reporting despite masterly inactivity. Egypt J Radiol Nucl Med 49:1–3
Kanwal R 3rd, Akhtar S (2021) Left hepatic lobe agenesis with ectopic gallbladder. Cureus 13(7):e16131
Fujimoto Y, Ohya Y, Irie T, Kumamoto S, Tuji A, Nakamura S et al (2019) Hypogenesis of right hepatic lobe in a laparoscopic cholecystectomy for acute gallstone cholecystitis: a case report. Intractable Rare Dis Res 8:146–149
Feleke AA, Birhanu FA, Tirfe FW, Molla YD (2024) Agenesis of the right lobe of the liver: a case report. J Med Case Rep 18:19
Alicioglu B (2015) Right liver lobe hypoplasia and related abnormalities. Pol J Radiol 80:503–505
Nacif LS, Buscariolli YDS, D’Albuquerque LAC, Andraus W (2012) Agenesis of the right hepatic lobe. Case Rep Med. https://doi.org/10.1155/2012/415742
Tadros MY, Louka AL (2018) Postoperative imaging of living donor liver transplantation complications. Egypt J Radiol Nucl Med 49:4–11
Acknowledgements
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
NB was responsible for conception and design of the work and critical revision of the article. AB was responsible for literature search, writing the initial draft and figures. All authors were directly involved in the radiological evaluation of the case in discussion.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no financial or personal relationships that may have inappropriately influenced them in writing this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bandyopadhyay, A., Bansal, N. A rare case of congenital right lobar segmental hepatic hypoplasia complicated by portal hypertension: a radiologic perspective. Egypt J Radiol Nucl Med 55, 101 (2024). https://doi.org/10.1186/s43055-024-01271-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-024-01271-6